Alternatives to allogeneic blood transfusions Preoperative autologous blood

Alternatives to allogeneic blood transfusions • Preoperative autologous blood donation • Acute normovolaemic haemodilution • Supportive administration of iron and/or recombinant human erythropoietin • Intraoperative cell salvage

Transfusion Guideline

Components • • • Whole Blood Packed RBCs Washed RBCs Deglycerolized RBCs Platetes Leukocyte concentration FFP(fresh frozen plasma) Cryoprecipitate Albumin
 vs a Liberal regimen (transfusion trigger <10")
Restrictive regimen (transfusion trigger <7 g/d. L) vs a Liberal regimen (transfusion trigger <10 g/d. L) • Observational study with 15, 534 patients by Malone: -RBC transfusion was associated with increased mortality, admission to ICU and ICU length of stay • it is generally agreed that the haemoglobin level in a bleeding patient should be maintained at 7– 8 g/d. L at least.

Suggested Transfusion Guidelines for Red Blood Cells -Hemoglobin <8 g/d. L or acute blood loss in an otherwise healthy patient with signs and symptoms of decreased oxygen delivery with two or more of the following: Estimated or anticipated acute blood loss of >15% of total blood volume (750 m. L in 70 -kg male) Diastolic blood pressure <60 mm Hg Systolic blood pressure drop >30 mm Hg from baseline Tachycardia (>100 beats/min) Oliguria/anuria -Hemoglobin <10 g/d. L in patients with known increased risk of coronary artery disease or pulmonary insufficiency who have sustained or are expected to sustain significant blood loss -Symptomatic anemia with any of the following: Tachycardia (>100 beats/min) Mental status changes Evidence of myocardial ischemia including angina Shortness of breath or dizziness with mild exertion Orthostatic hypotension -Unfounded/questionable indications: To increase wound healing To improve the patient’s sense of well-being 7 g/d. L < hemoglobin <10 g/d. L (or 21% < hematocrit < 30%) in otherwise stable, asymptomatic patient Mere availaility of pre-donated autologous blood without medical indication
 platelet count <10, 000/㎣ (for")
Suggested Transfusion Guidelines for Platelets -Recent (within 24 hours) platelet count <10, 000/㎣ (for prophylaxis) -Recent (within 24 hours) platelet count <50, 000/㎣ with demonstrated microvascular bleeding (“oozing”) or a planned surgical/invasive procedure -Demonstrated microvascular bleeding and a precipitous fall in platelet count -Adult patients in the operating room who have had complicated procedures or have required more than 10 units of blood AND have microvascular bleeding. Giving platelets assumes adequate surgical hemostasis has been achieved. -Documented platelet dysfunction (e. g. , prolonged bleeding time greater than 15 minutes, abnormal platelet function tests) with petechiae, purpura, microvascular bleeding (“oozing”), or surgical/ invasive procedure -Unwarranted indications: Empirical use with massive transfusion when patient is not having clinically evident microvascular bleeding (“oozing”) Prophylaxis in thrombotic thrombocytopenic prupura/hemolytic-uremic syndrome or idiopathic thrombo-cytopenic purpura Extrinsic platelet dysfunction (e. g. , renal failure, von Willebrand’s disease)

Suggested Transfusion Guidelines for Fresh Frozen Plasma Treatment of multiple or specific coagulation factor deficiency with abnormal prothrombin time and/or activated partial thromboplastin time -Abnormal specific factor deficiency in the presence of one of the following: Congenital deficiency of AT-III; prothrombin, factors Ⅴ, Ⅶ, Ⅸ, Ⅹ, and XI; protein C or S; plasminogen or antiplasmin -Acquired deficiency related to warfarin therapy, vitamin K deficiency, liver disease, massive transfusion, or disseminated intravascular coagulation -Also indicated as prophylaxis for the above if a surgical/invasive procedure is planned -Unwarranted indications: Empirical use during massive transfusion if patient does not exhibit clinical coagulopathy Volume replacement Nutritional supplement Hypoalbuminemia -
 • developed as haemostatic agent for use in")
Recombinant activated factor VII (r. FVIIa) • developed as haemostatic agent for use in haemophilia patients • r. FVIIa plasma concentrations of 25 nmol/L: Haemostasis is induced • binds to the phospholipid structures of activated platelets at the site of injury , thereby directly activates factors IX and X-> leads to the enhancement of thrombin(thrombin burst)


Major HBP Surgery • HBP malignancy • Liver Transplantation • Liver injury

HBP Malignancy
, HCC")
Transfusion: Prognostic Factor • Colorectal, breast, gastric, periampullary(pancreas, Ao. V, distal CBD, duodenum), HCC • Immmunosuppression • Tf 은 사실 the extensiveness of the operation을 반영하나 이를 정량화 하기 어려우므로 결국 Tf을 최소화하려는 노 력이 중요

Tech aspects of Hepatectomy • Inflow vascular occlusion • Low CVP • Liver resection devices : CUSA, waterjet, harmonic scalpel, Ligasure • Local acting agent: fibrin glue, collagen, topical thrombin

Inflow vascular occlusion

Liver resection devices
")
Transfusion in Liver Transplantation(LT)

Bleeding during LT • Inevitable massive bleeding during LT : about two thirds Because of -long operation time, wide op. field -thrombocytopenia, abnormal coagulation -multiple collateral circulation

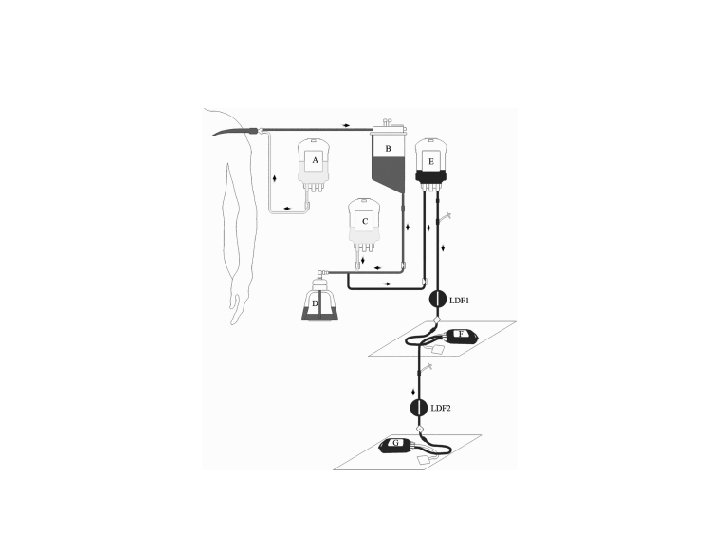
Cell Saver

Potential Hazards Cell Saver in LT • Viral reinsertion • High risk for systemic dissemination of tumor cells

Cell Saver during LT in Pts with HCC


Liver Trauma

Liver Trauma • Liver: most frequently injured abdominal organ

Early signs of shock • altered level of consciousness • delayed capillary refilling, mottled skin as a consequence of reduced peripheral perfusion • oliguria

Massive hemorrhage

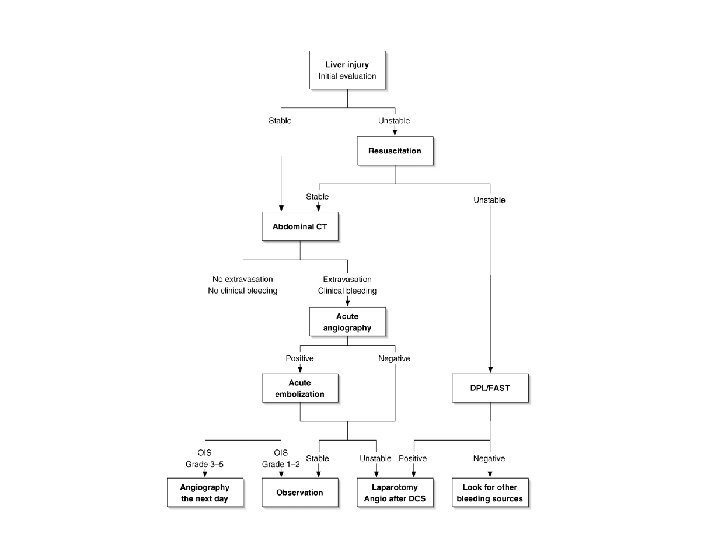
Management of Liver Trauma • • • - Early diagnosis Proper resuscitation Tx conservative management Intervention surgery

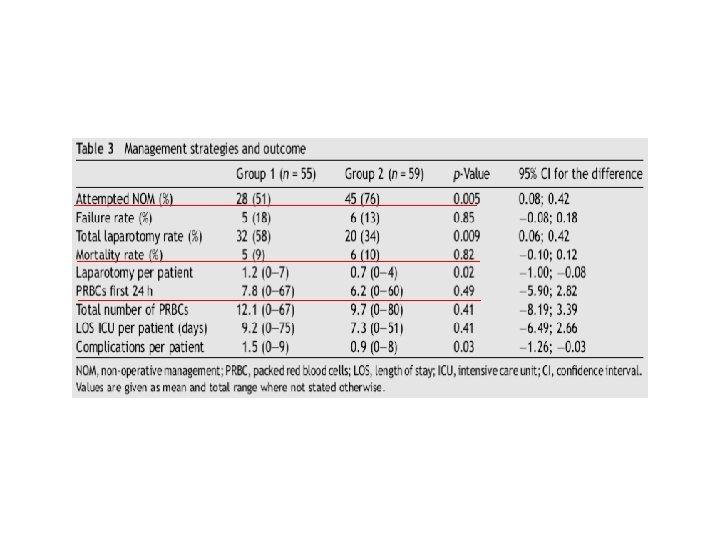
Liver injuries–—Improved results with a formal protocol including angiography

• Group 1: patients who were haemodynamically unstable and had intraabdominal haemorrhage were operated on immediately • Group 2: the existing treatment policy was formalised in a protocol introducing angiography in severe liver injuries

Conclusion • Transfusion need should be assessed on a case by case basis: empirical use not warranted • Meticulous hemostasis during elective surgery • Proper and prompt decision (esp. liver trauma) • Use alternatives to allogeneic blood transfusions if possible • Cooperation with anesthesiologist
- Slides: 37