Alternative Access Suprasternal TAVR Is it needed Isaac




 It pays")



















- Slides: 26
Alternative Access: Suprasternal TAVR Is it needed? Isaac George, M. D. Surgical Director, Structural Heart and Valve Center New York Presbyterian Hospital – Columbia University Medical Center
Disclosures: Isaac George M. D. Consulting: Cardio. Mech Mitre. Medical Atricure WL Gore Associates Vdyne Neptune Medical
TAVR now is not like TAVR 10 years ago… • Valve technology is better 10% 1 -2% • Sheath sizes have decreased significantly!
Sheath Size Can Contribute to Major Vascular Complications A Sheath to Femoral Artery Ratio (SFAR) ≥ 1. 05 is a Predictor of both VARC Major Vascular Complications and 30 -Day Mortality Hayashida, K et al. JACC CV Int 2011
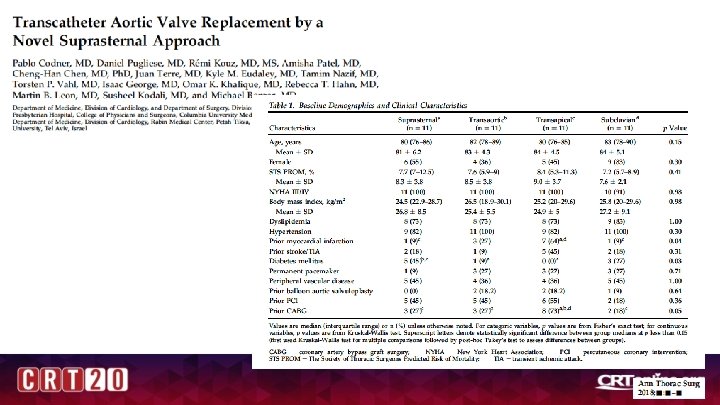
There may be a mortality penalty for Transthoracic TAVR (Transapical, direct aortic) It pays to stay out of the chest Smith et al. ACC 2016
“Alternative” Alternative Access has flourished Subclavian TAVR – Evolut R Trans-Caval TAVR – Sapien 3 L Carotid– TAVR
“Alternative” Alternative Access has flourished Shockwave
Is there a need? Subclavian not possible in all patients Ø Subclavian artery is often small too to use, sheath can be occlusive Ø Subclavian access may compromise LIMA-LAD flow Ø Angulation often difficult from LSCL (esp for Core. Valve) Ø Complications can be catastrophic! Transcarotid may have high stroke rates Ø Lots of arch manipulation with wires Ø Inherent risk of stroke via carotid manipulation Transcaval/Shockwave requires a lot of resources Ø Expensive!! Ø High experience level
Advantages of Suprasternal Access Direct surgical cutdown through a small incision Quick: <45 min total skin to skin Easily compatible with any valve delivery system Good for reops, CABG, prior thyroid, prior XRT No violation of thoracic cavity Can walk patients immediately after procedure (no catheters in groin) • Straight line from access to the annulus • • •
• • Procedural Steps Left IJ neck line and pacer Surgical cutdown Acccess artery with needle, 7 F sheath Cross valve, stiff wire Insert valve sheath Deploy Remove sheath and tie under rapid pacing Final Angiogram
Supra-sternal Aortic Access – Sapien 3
Direct Inominate Artery Approach
Clinical Experience • • • Procedural description outlining Aegis use 35 pts Mean procedure time 90 min Total hospital LOS 4 days PPM 3 pts, 1 minor vascular complication
Length of Stay DC location
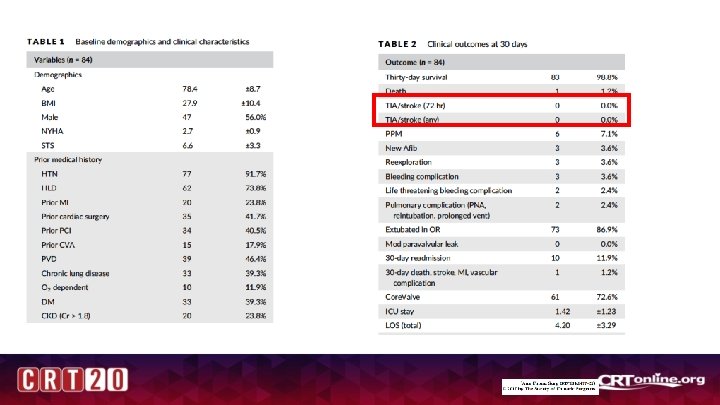
• • 3 year time frame 84 pts Total volume ~1604 pts Other alt access: 43
• • • 9 pts BMI 50 No deaths, reinterventions LOS 3 -5 days Extubated in OR
Indications • • Poor femoral access Morbidly obese Good for Reop OK for prior CABG Caveats Must tolerate GA Must have calcium free ostia >6 -7 cms depth fixed neck Exclusions : 1 -2 cases per year/20 -30 alt access/550 -600
Final Thoughts • Suprasternal TAVR provides access to the innominate artery for TAVR • Quick surgical access • Direct deployment without angulation issues • Ideal for anyone at high risk for vascular complication, obese patients, or require early mobilization • First-line approach after TF
Case 1: Evolute
Inominate Artery Anatomy
Deployment
Case 2: Sapien 3
Inominate Artery Anatomy
Deployment