Allogeneic Stem Cell Transplantation for bcrabl negative Myeloproliferative

Allogeneic Stem Cell Transplantation for bcr/abl negative Myeloproliferative Neoplasm MPN Horizons 2016, 11 -13 November 2016, Belgrade, Serbia Nicolaus Kröger University Hamburg Medical Center Dept of Stem Cell Transplantation
 CML bcr-abl + Polycythemia Essent. vera Thrombocythemia")
Myeloproliferative Neoplasm (Diseases of hematopoetic stem cell) CML bcr-abl + Polycythemia Essent. vera Thrombocythemia bcr-abl - Primary Myelofibrose
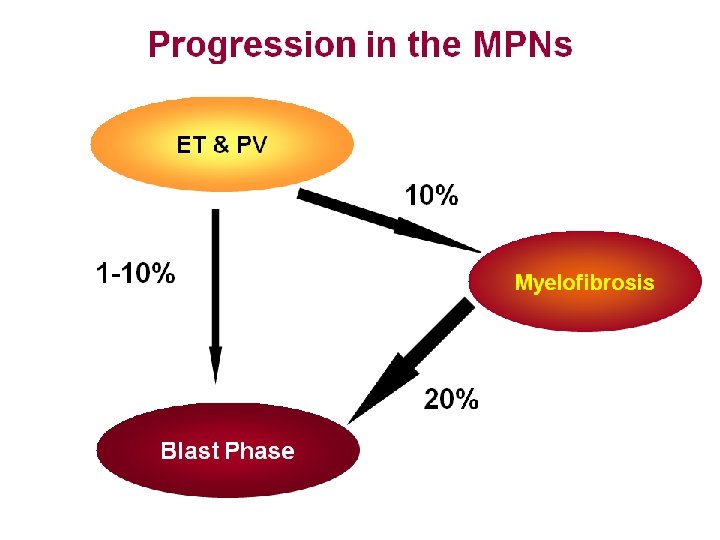

Treatment Options • Can PV, ET or Myelofibrosis be cured? Answer: Yes, but currently only by allogeneic stem cell transplantation

Treatment Options Why to treat and what is the treatment goal? 1. ET: Prevent thrombosis 2. PV: Prevent thrombosis Reduce symptoms such as pruritus and symptoms of large spleen 3. Myelofibrosis: a) Reduce symptoms such as weakness, splenomegaly, weight loss, night sweat, anemia, bone pain, b) Cure

Which patient should be considered for allogeneic stem cell transplantation? PV general: no indication for allogeneic SCT ET general: no indication for allogeneic SCT Except: Transformation to post ET/PV MF Transformation to Acute Leukemia Myelofibrosis: yes : depending on status of the disease, donor availability and also on age

What can be achieved by Allogeneic Stem Cell Transplantation? 1. Complete hematological remission including molecular remission 2. Resolution of splenomegaly and constitutional symptoms 3. Regression of bone marrow fibrosis 4. Long-term survival (cure)

before allo MF-3 day +100 MF-0

Treatment Options for MPN: Allogeneic Stem Cell Transplantation • What is Stem Cell Transplantation?

Hematopoesis Bone Marrow Pluripotente Stem Cell Multipotente Stem Cell Megakaryocyt Blood Platelets Erythroblast Erythrocytes Hematopoietic Stem Cell (neuronal, mesenchymal) Myeloid Progentitor-cell Granulocyte Monocyte T-Lymphocyte Lymphoide Stem Cell prä T-Cell B-Lymphocyte prä B-Cell

Stem Cell Transplantation Stem Cell autologous allogeneic

Why is Allogeneic Stem Cell-Transplantation curative and why are there complication? T-Cells Graft versus Host (Gv. HD) Donor Recipient CD 34+ stemcells Graft versus Myelofibrosis Effect

How to decide for allogeneic stem cell transplantation? Allografting treatment related morbidity and mortality potential cure Consider also: 1. Life expectancy without transplantation ? 2. Cure rate with transplantation ? 3. alternative options?

Risk scoring system Factors Score • Age > 65 years DIPSS: Dynamic International Prognostic Scoring System for PMF 1 • Constitutional symptoms 1 • Hb < 10 g/d. L 2 • Leukocytes > 25 x 109/L 1 • Blood blasts > 1% 1 Risk groups • Low 0 • Intermediate-1 1 -2 • Intermediate-2 3 -4 • High ≥ 5 Passamonti F et al. , Blood 2010, 115: 1703 -8

Survival by DIPSS category Scott B L et al. , Blood 2012; 119: 2657 -2664

Prerequisation for Allogeneic Stem Cell Transplantation • HLA-compatible donor
")
Need for a donor to perform allogeneic stem cell transplantation 1. Syngeneic (identical twin) 2. HLA-identical sibling 3. HLA-compatible unrelated donor

Hematopoietic Stem Cell Transplantation HLA-identical sibling

Unrelated Donor Register Worldwide more than 20 million volunteers 80 - 90% probability to find a suitable stem cell donor (for caucasian)
 n= 14950 allogeneic SCT Passweg et al")
Transplant activity Europe 2013 (EBMT data base) n= 14950 allogeneic SCT Passweg et al BMT 2015

How do we get the malignant cells out and the new stem cells into the patient? Bone Marrow Pluripotente Stem Cell Multipotente Stem Cell Megakaryocyt Blood Platelets Erythroblast Erythrocytes Hematopoietic Stem Cell (neuronal, mesenchymal) Myeloid Progentitor-cell Granulocyte Monocyte T-Lymphocyte Lymphoide Stem Cell prä T-Cell B-Lymphocyte prä B-Cell

Hematopoietic Stem Cell Source Bone Marrow Peripheral Blood 1% 0, 05% Cord Blood

Hematopoietic Stem Cell Source Bone Marrow Peripheral Blood 1% 0, 05% Cord Blood

Conditioning Three Aims: Allow engraftment of donor stem cells Immunosuppression Reduce tumorload Anti-tumor activity Myeloablation Total Body irradiation and high dose chemotherapy

Conditioning Three aims: Engraftment of Stem Cells Kill tumor-cells Immunosuppression Anti-tumor activity Myeloablation Provide space for new stem cells Fludarabin T-lymphocyte of donor

Patient Donor Conditioning Stem Cells Stem Cell Transplantation Aplasia

inpatient (ca. 4 weeks Patient Donor Conditioning Stem Cells Stem Cell Transplantation Aplasia Engraftment outpatient (> 1 year) Immunological reconstitution

inpatient (ca. 4 weeks Patient Donor Conditioning Stem Cells Stem Cell Transplantation Aplasia Engraftment outpatient (> 1 year) Immunological reconstitution

inpatient (ca. 4 weeks Patient Donor Conditioning Stem Cells Stem Cell Transplantation Aplasia Engraftment outpatient (> 1 year) Immunological reconstitution
 Ruxolitinib approval")
Allogeneic SCT in PMF (Passweg et al. , EBMT ) Ruxolitinib approval

Scenario of allogeneic SCT in Myelofibrosis Pre-transplant strategies Transplantation strategies 1. reduce spleen size. by JAK inhibitor consider splenic irradiation or splenectomy in refractory patients with excessive spleen volume 1. select patients according to DIPSS intermediate 2 / high risk 2. consider high risk molecular marker for intermediate 1 patients 3. perform conditioning with toxicity or dose-reduced regimen according to age and comorbidities 2. improve constitutional symptoms by JAK inhibitors 3. improve iron overload by pre-transplant chelation 4. select optimal donor MRD → MUD → alternative donor Post-transplant strategies 1. monitor molecular marker post transplant to assess minimal residual disease (MRD) 2. consider early discontinuation of immunosuppression or donor lymphocyte infusion in case of MRD 3. consider JAK inhibition in case of severe Gv. HD (within clinical trial)

Acknowledgement Haefaa Alchalby Tatjana Zabelina Anita Badbaran Boris Fehse Thomas Stübig Ioanna Triviai Francis Ayuk Max Christopeit Christine Wolschke Yves Chalandon Eduardo Olavarria Anja van Biezen Donal Mc. Lornan Marie Robin Kavita Raj Giovanni Barosi Tiziano Barbui Dominik Wolf Staff of the Department of Stem Cell Transplantation University Hospital Hamburg European Leukemia Net (ELN) Members of the EBMT/ELN consensus panel Chronic Malignancies Working Party of the European Group for Blood and Marrow Transplantation (EBMT) University Hospital Bonn Francesco Passamonti
- Slides: 34