Alcohols DR BABAK MASOUMI ASSISTANT PROFESSOR OF EMERGENCY

Alcohols DR BABAK MASOUMI ASSISTANT PROFESSOR OF EMERGENCY MEDICINE ESFAHAN UNIVERSITY OF MEDICAL SCIENCES 2011

Types of alcohol Beer n Wine n Spirits n Vodka n Gin n Whiskey n Rum n n n n Ethanol / Ethyl alcohol Methanol / Methyl alcohol Isopropanol / Isopropyl alcohol Ethylene glycol Propylene glycol Fusel oil

Ethanol H H H C C H H Ethyl Alcohol OH

. The ethanol concentration in distilled spirits is traditionally listed in terms of proof. In the United States, this expression represents twic PROOF: The ethanol concentration in distilled spirits is traditionally listed in terms of proof. n In the United States, this expression represents twice the percentage concentration; for example, 80 proof is equivalent to 40% ethanol by volume. n

Methanol H H C H Methyl Alcohol OH

Methanol Poisoning n n A product of wood distillation, it is a component of many paint removers, varnishes, shellacs, windshield washing fluids, and antifreeze formulations. Methanol poisoning has resulted from the consumption of contaminated whiskey, accidental ingestion by desperate alcoholics, or intentional ingestion during suicide attempts.

Methanol Poisoning Methanol is also present in measurable but small amounts in wine and distilled spirits, accounting for the fact that low levels may be detectable in the blood after binge drinking. n Methanol's toxicity is due to the formation of two toxic metabolites, formaldehyde and formic acid. n

Methanol

Ethylene glycol
, preservative, and")
Ethylene Glycol Ethylene glycol has many commercial uses as a coolant (antifreeze), preservative, and glycerine substitute; it has also been used in lacquers, cosmetics, polishes, and detergents. n Ethylene glycol's toxicity is the result of the formation of two toxic metabolites, Glycoaldehyde and Glycolic acid. n

Ethylene Glycol / Methanol Ethylene Glycol

Isopropanol / Isopropyl alcohol

Isopropanol / Isopropyl alcohol Isopropanol= isopropyl alcohol and 2+propanol. n It is also used widely in industry as a solvent and disinfectant , component of a variety of skin and hair products, jewelry cleaners, detergents, paint thinners, antifreeze. Poisoning usually results from ingestion. n

Isopropanol / Isopropyl alcohol May also occur after inhalation or dermal exposure in poorly ventilated areas—for example, during alcohol sponge bathing. n Its principal metabolite, acetone, does not cause the eye, kidney, cardiac, or metabolic toxicity caused by the metabolites of methanol and ethylene glycol. n

Isopropanol / Isopropyl alcohol n n n Isopropanol is approximately twice as potent as ethanol in causing central nervous system depression and its duration is two to four times that of ethanol. After ethanol, it is the second most commonly ingested alcohol. Though more toxic than ethanol, it is considerably less so than methanol or ethylene glycol.

Propylene glycol

Production of Alcohol Fermentation – Sugar to Alcohol and Carbon dioxide C 6 H 12 O 6→ 2(CH 3 -CH 2 -OH) + 2 CO 2

ETHANOL n n n Ethanol is the most frequently used and abused intoxicant in the United States and most other societies. Nearly three-quarters of adult Americans consume at least one alcoholic drink each year. Beer ranks as the fourth most popular beverage in terms of volume consumed, after soft drinks, milk, and coffee.

Some Current Facts: Ø 7. 4% of adult population in U. S. alcoholic Ø $185 Billion – cost of alcohol abuse in U. S. Ø 100, 000 deaths annual in U. S. related to Ø $1. 2 Billion spent on wine, beer and liquor advertisements in U. S.

ETHANOL n n n One-quarter of the victims of interpersonal trauma report alcohol use by their assailants. Alcohol abuse as reported by the injured woman is the strongest predictor for acute injury related to domestic violence. The prevalence and lifelong risk of alcohol abuse or dependence are 7 and 13 percent.

Ancient Awareness "You will conceive and bear a son…now then be careful to take no wine or strong drink and to eat nothing unclean". Bible - Judges 13: 3 -4

IN IRAN

Pharmacology and Metabolism Ethanol is a CNS depressant which inhibits neuronal activity. n Alcohol intoxication is associated with the depression of the excitatory neurotransmitter glutamate and alcohol increases the inhibitory activity of the neurotransmitters -aminobutyric acid (GABA) and glycine. n

Pharmacology and Metabolism n The clinically observed crosstolerance that exists between ethanol and other sedative-hypnotic agents, including benzodiazepines and barbiturates, appears related to the similar affects that these agents have on brain chemistry.

Pharmacology and Metabolism Ethanol absorption : n In the mouth and esophagus to a small extent. n In the stomach and large bowel to a moderate extent. n In the proximal portion of the small bowel chiefly absorbed.

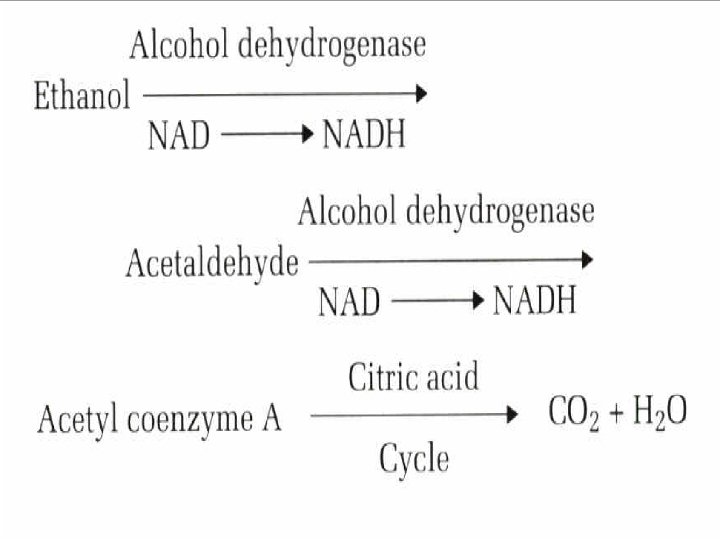
Pharmacology and Metabolism n n Approximately 2 to 10 percent of ethanol may be excreted by the lungs, in urine, or in sweat, the proportion being dependent on blood concentration. The Reminder of ethanol metabolized to acetaldehyde in the liver by one of two pathways.
In the cell, cytosol alcohol dehydrogenase with nicotinamide adenine dinucleotide as")
Pharmacology and Metabolism 1)In the cell, cytosol alcohol dehydrogenase with nicotinamide adenine dinucleotide as a cofactor produces acetaldehyde, which in turn is metabolized by aldehyde dehydrogenase. 2) The second pathway, which is clinically significant at high blood ethanol concentrations and has increased activity with repeated exposures to ethanol, is a microsomal alcohol oxidizing system.

Gender-related differences in the metabolism n n Gender-related differences in the metabolism of ethanol explain the considerably higher blood ethanol levels in women versus men after similar dosing on a gram-per-kilogram basis. Women have a smaller volume of distribution (0. 6 L/kg) for ethanol than men (0. 7 L/kg) and have decreased first-pass metabolism of ethanol because their gastric walls contain less alcohol dehydrogenase than do those of men.


Opioid/Sedative/Ethanol Toxidrome n Common Signs: Coma, respiratorydepression, miosis, hypotension, bradycardia, hypothermia, pulmonary edema, decreased Bs, hyporeflexia.

Acute Effects • • CNS Depressant Depression of inhibitory control Vasodilation, warm, flushed, reddish skin Emotional outbursts Decreased memory & concentration Poor judgment Decreased reflexes Decreased sexual response

Clinical Features n Symptoms and signs of ethanol intoxication include slurred speech, nystagmus, disinhibited behavior, central nervous system depression including coma, and decreased motor coordination and control.

Clinical Features n A lowering of blood pressure or even hypotension with resultant reflex tachycardia are common secondary to a decrease in total peripheral resistance or as a result of volume loss. Changes in posture may result in syncope. However, when hypotension is present, other causes must be considered.

Clinical Features Because of the phenomenon of tolerance, blood alcohol levels correlate poorly with degree of intoxication. n While death from respiratory depression may occur in unhabituated individuals at concentrations of 400 to 500 mg/d. L, it is not uncommon for some alcoholics to appear minimally intoxicated at blood concentrations as high as 400 mg/d. L. n
 =Volume Ingested(ml)× Ethanol Concentration × /0. 6 × Weight")
n n Blood Ethanol Concentration(mg/dl) =Volume Ingested(ml)× Ethanol Concentration × /0. 6 × Weight Accordingly, each 1 ounce of 100 proof whiskey, 12 ounces of beer, or 4 ounces of a typical table wine consumed by a 70 -kg man should theoretically raise the blood ethanol concentration by approximately 30 mg/d. L.
 Little demonstrable effect <30 Mild euphoria, minimal")
Blood Ethanol Concentration Manifestations Clinical (mg/d. L) Little demonstrable effect <30 Mild euphoria, minimal central nervous system effects, subjective 30 -50 sensation of cutaneous warmth Relaxation, jocularity, gregariousness, cutaneous flushing, prolongation 50 -80 of reaction time Statutory intoxication in many jurisdictions 80 -100 Loquacity, animation, exuberance, exaggerated emotional responses, 100 -200 uninhibited behavior, impaired judgment Sedation interrupted by periods of boisterous or antisocial behavior, nausea, 200 -300 emesis, dysarthria, horizontal nystagmus, impaired visual pursuit, diplopia, ataxia Unstable station and gait, incoherent speech, somnolence, impairment of protective airway reflexes, incontinence, obtundation, stupor 300 -400 >400 Coma, loss of protective reflexes, respiratory depression, death

Clinical Features Although most states have adopted 80 or 100 mg/d. L as the legal definition of intoxication for the purposes of driving a motor vehicle. n There is considerable evidence to suggest that impairment may be seen with levels as low as 5 mg/d. L, especially in unhabituated individuals. n

Clinical Features A mild lactic acidosis may be seen. n However, significant acidosis should never be attributed to alcohol intoxication, and should prompt an aggressive search for another cause. n In the presence of volume depletion, a mild contraction alkalosis may be noted, as may pre-renal azotemia. n

Treatment n Management of acute ethanol intoxication consists of attending to associated injuries or medical illness and observation until clinical sobriety is attained. n A careful examination should be performed to evaluate for complicating injuries or medical conditions.

Treatment: n Ethanol levels are not necessarily required for mild or moderate intoxication when no other abnormality is suspected. It is appropriate in all patients with depressed level of consciousness or altered mental status. n The most appropriate fluid is D 5 NS.

Treatment Hypoglycemia should be excluded by a bedside glucose determination. n In the event of severe depression of mental status, causes other than alcohol ingestion must be considered, especially subdural hematoma, which can occur in the absence of external signs of trauma. n

Treatment n Fluid administration does not hasten alcohol elimination. n Intravenous access for fluid administration alone is unnecessary in uncomplicated cases of mild to moderate intoxication unless clinical signs of volume depletion are present.

Treatment n Any alcoholic with CNS depression, even if apparently attributable to intoxication, should receive thiamine. n Folate and other vitamins are indicated only if there are clinical signs or laboratory confirmation of deficiency.

Treatment n Ethanol does not bind to Activated charcoal, which should be administered only if other substances have been ingested that are adsorbable.

Treatment n n Careful and serial observation is crucial, as in the vast majority of uncomplicated cases rapid improvement occurs over a few hours. Mental status that fails to improve and any deterioration should be considered secondary to other causes and evaluated aggressively.

Treatment n Respiratory depression may result in carbon dioxide retention, which on rare occasion may require intubation.

Treatment n Unhabituated patients eliminate ethanol from the bloodstream at a rate of 15 to 20 mg/d. L per h. n Alcoholics average 25 to 35 mg/d. L per h.

Treatment n Alcoholics should be questioned about concomitant drug use. In the past, ethylene glycol or methanol was occasionally substituted for or combined with ethanol. Today Cocaine has clearly become the most common concomitant drug used by alcoholics.

Treatment n The risk of sudden death among users of both drugs simultaneously may be as high as 20 times that with cocaine alone.

Treatment n n n Ethanol is the most common cause of an osmolar gap. The concomitant presence of an anion-gap (AG) metabolic acidosis may help characterize the presence of a coingestant. Methanol and ethylene glycol poisoning are associated with significant widened AGtype acidosis.

Disposition n Morbidity and mortality in association with acute intoxication are predominantly the result of injuries, often motor vehicle collisions related to ethanolinduced deficits in judgment or physical capabilities.

Disposition n Patients with acute ethanol intoxication alone rarely require hospital admission. Questions frequently arise over alcoholics who appear clinically sober while still having considerable blood ethanol concentrations. Medical judgment of mental competence should not be confused with any particular blood alcohol concentration level.

Disposition n Patients whose intoxication has resolved to the extent that they do not constitute a danger to themselves or others, and who will not be responsible for their own transportation, may be discharged on their own recognizance or preferably in the company of responsible friends or relatives who can assist them and take some responsibility for their care.
 can")
Disposition n Discharge (after excluding significant abnormal laboratory values or suspected head injury) can be considered if a concerned, sober adult is willing to take responsibility for and remain with the patient for the next 24 to 48 hours.

Disposition n Patients who are to drive themselves home should have ethanol levels close to zero, not merely below a given state's legal level for driving, as there is theoretical potential for psychometric disability at very low levels, and the potential liability for the emergency physician is unfortunately huge.


- Slides: 59