Alcohol use alcohol problems and alcoholism public health

Alcohol use, alcohol problems and alcoholism – public health research and epidemiology Andreas Lundin Department of Public Health Sciences Karolinska Institutet andreas. lundin@ki. se
 Injuries (self")
Background Alcohol use causes various outcomes: - Toxic effects (self and offspring) Injuries (self and external) Mental disorders (cognitive and depressive) Alcoholism is a special disorder that require consumption, is surrounded by moral, is largely reversible Alcohol consumption is together with sex, age and smoking a common confounder Measuring alcohol use and disorder is difficult

Disposition Definitions ”Instruments” Validity Bias

Definition Epidemiological studies encompass sociological as well as medical traditions A continious or dichotomous approach No definition represent the ”truth” Apparent dual attitude towards alcohol use
 Alcohol abuse/harm Alcohol problems Risk use,")
Definition Alcoholism, alcohol use disorder Alcohol dependence (addiction) Alcohol abuse/harm Alcohol problems Risk use, hazardous use Alcohol use, moderate use Abstaining

Definition 1. Abstainers and non-current drinkers - Abstaining not norm in many countries - Easily defined - Life time and last year - Heterogenous group(s) - A poor reference group?

Definition 2. Alcohol problems - defined by ”consequences” of drinking - which problems are attributable and by whom? - E. g. , arrested for drunk driving – a consequence of alcohol, or - Have you lost a partner due to drinking? - Getting into arguements with wife?
 End product of alcohol use (? )")
Definition 3. Alcoholism (alcohol use disorder, addiction) End product of alcohol use (? ) Dependence (and abuse) Disorders/diagnosis Symptoms/consequences +feelings and behaviour Symptom count
 Two diagnostic systems: - International Classification of")
Definition Alcohol use disorder (Dependence and Abuse) Two diagnostic systems: - International Classification of Disease (ICD, WHO) - Diagnostic and Statistical Manual of Mental Disorders (DSM, APA)
 Three or more of")
Definition Dependence: ICD-10 diagnostic criteria for research (similar to DSM-IV) Three or more of the following manifestations should have occurred together for at least 1 month or, if persisting for periods of less than 1 month, should have occurred together repeatedly within a 12 -month period: A strong desire or sense of compulsion to take the substance; Impaired capacity to control substance-taking behaviour in terms of its onset, termination, or levels of use, as evidenced by the substance being often taken in larger amounts or over a longer period than intended, or by a persistent desire or unsuccessful efforts to reduce or control substance use; A physiological withdrawal state when substance use is reduced or ceased, as evidenced by the characteristic withdrawal syndrome for the substance, or by use of the same (or closely related) substance with the intention of relieving or avoiding withdrawal symptoms; Evidence of tolerance to the effects of the substance, such that there is a need for significantly increased amounts of the substance to achieve intoxication or the desired effect, or a markedly diminished effect with continued use of the same amount of the substance; Preoccupation with substance use, as manifested by important alternative pleasures or interests being given up or reduced because of substance use; or a great deal of time being spent in activities necessary to obtain, take or recover from the effects of the substance; Persistent substance use despite clear evidence of harmful consequences as evidenced by continued use when the individual is actually aware, or may be expected to be aware, of the nature and extent of harm.
 criterias based on social consequences (+risk")
Definition Abuse or harmful use - DSM (abuse) criterias based on social consequences (+risk taking). Non overlapping symptoms with dependence, in some versions in the presence of dependence. - ICD (harmful use) physical or mental damage in the absence of dependence. Harmful use commonly, but not invariably, has adverse social consequences; social consequences in themselves, however, are not sufficient to justify a diagnosis of harmful use.

DSM-5 Do not separate symptoms of dependence or abuse New name – Alcohol Use Disorder Lower cut point (2 or more of 11) Introduces a severity scale (simple count)
 - pre-disorder but not necessarily pre-problems")
Definition Hazardous use, - not a disorder (yet…) - pre-disorder but not necessarily pre-problems - use: frequency, amount, pattern (high consumption, binge drinking) - Central to public health

Instruments How do we measure use, riskuse and disorder? Registers? Surveys? Tests?

Instruments Main source of knowledge: Psychiatric epidemiologic samples Random samples Diagnostic instruments Ideally interview by psychiatrist Commonly interview by trained nurse using structured interviews Expensive

Instruments Common psychiatric samples based on interviews: National Epidemiologic Survey on Alcohol and related Conditions (AUDADIS) The National Comorbidity Survey (CIDI) Australian National Survey of Mental Health and Well-Being (CIDI) Canadian National Survey of Mental Health and Well-Being (CIDI) NEMESIS (CIDI) Health Mental Health Survey (CIDI) Women Alcohol Göteborg (CIDI-SAM) (Sweden) PART (SCAN) (Stockholm)
 - Used for stratified")
Instruments Screening instruments - Often developed in primary care (two-stage) - Used for stratified random sampling (double phase) - Often as proxies for diagnoses (diagnostic tool) in Public Health Epidemiology - Alcohol disorder or alcohol use

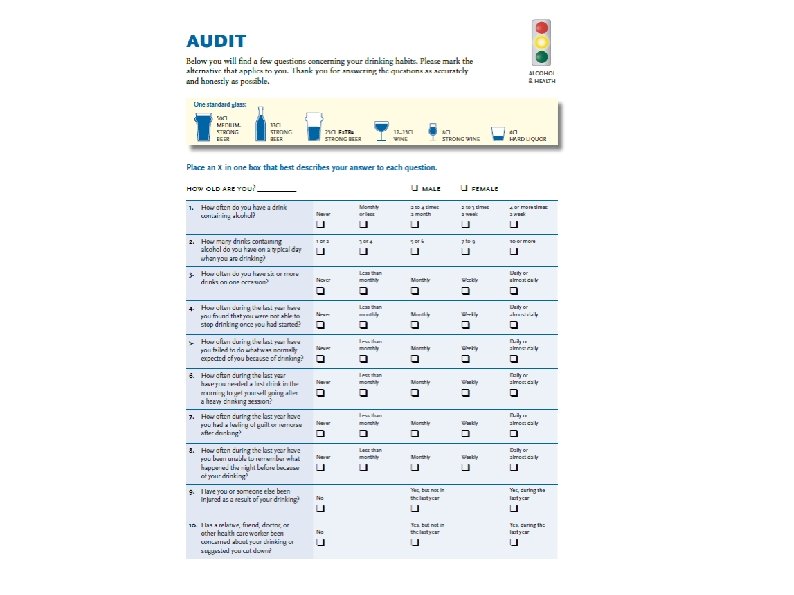
Instruments AUDIT – the Alcohol Use Disorder Indentification Test MAST – Michigan Alcohol Screening Test CAGE (Cut down, Annoyed, Guilt, Eye-opener) index-sum indicating severity or probability of problem drinking, approximation of disorder, or risk use (interpretation).

Alcohol problems-single items - in public health & occupational medicine • Do you have alcohol problems? • Would you like to cut down on you drinking? • Ever in any treatment or program (like AA)? • ?

Hazardous use and Alcohol consumption Hazardous use commonly measures with consumtion patterns Manu countries have national recommendations, for Sweden: No more than 9 standard drinks for women, 14 for men/week Standard drink (Sweden) = 12 gram pure alkohol (about 330 ml beer/120 ml wine/40 ml spirits) US standard drink = 14 g Australia standard drink = 10 g
 • Quantity, beverage specific or not • Frequency, open or graded •")
Quantity-Frequency (QF) • Quantity, beverage specific or not • Frequency, open or graded • Time period, e. g last week, typical week/month, current normal, previous heavier

Quantity and Frequeny Swedish national health survey
 e. g. small beer: 13")
Stockholm PHQ Alcohol in g = vol * (ABV*density) e. g. small beer: 13 g = 0. 33 l * (0. 05 *789 g/l) Note: sometimes all days in the week is listed, sometimes drinks, always normal week

Binge drinking Hazardous drink pattern: episodic excessive drinking, heavy episodic drinking: Commonly 5/4 -definition (US) In the Stockholm public health queistionnaires typically:

Frequency of intoxication Appears in The Swedish National Public Health Questionnaire Subjective, or individual 2 -3 times a month was considered risky

Consumption and dependence Dependence 18 -64 year olds M: 4. 9% W: 3. 2%
")
Bias If sensitivity and specificity is equally poor in two populations (no systematic missclassification) RRs are underestimated Using such a variable as control variable leads to residual confounding If the two populations have different sensitivity and specificity, RR could be over or under estimates (or completely artificial) KAREN T. COPELAND, HARVEY CHECKOWAY, ANTHONY J. Mc. MICHAEL AND ROBERT H. HOLBROOK. 1977. BIAS DUE TO MISCLASSIFICATION IN THE ESTIMATION OF RELATIVE RISK. AMERICAN JOUBNAL OF EPIDEMIOLOGY Vol. 105, No. 5 These are worth thinking about since alcohol is a common confounder

Bias Sources: Non participation Self-assessment Social desirability Denial

andreas. lundin@ki. se
- Slides: 30