AKI Definition Stages RIFLE vs AKIN Causes and

 • Causes")









")

 A 50 -year-old man (who smoked one pack of cigarettes/day x")





- Slides: 25
AKI
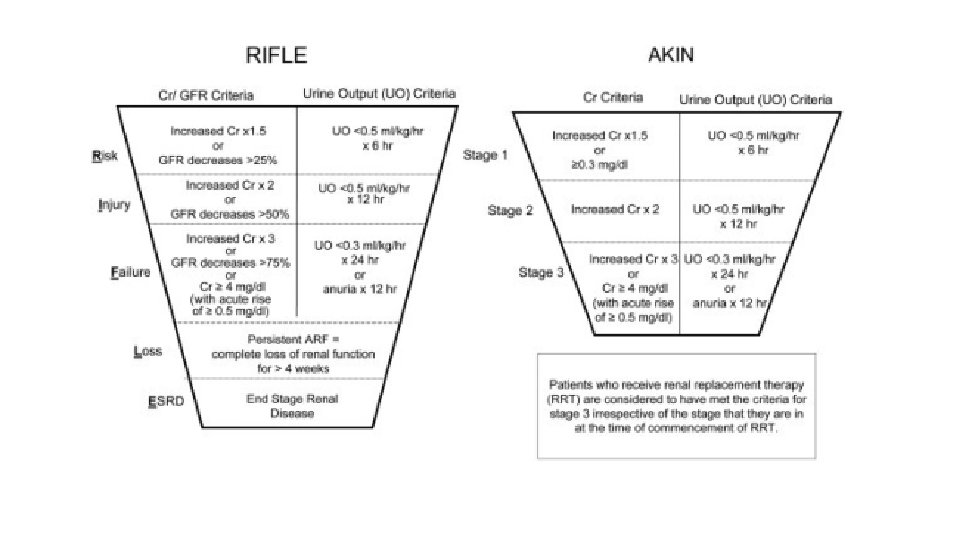
• Definition : • Stages : ( RIFLE vs. AKIN ) • Causes and classification : Pre-renal Renal Post- renal • Clinical manifestations and Complication • Management and indications for RRT
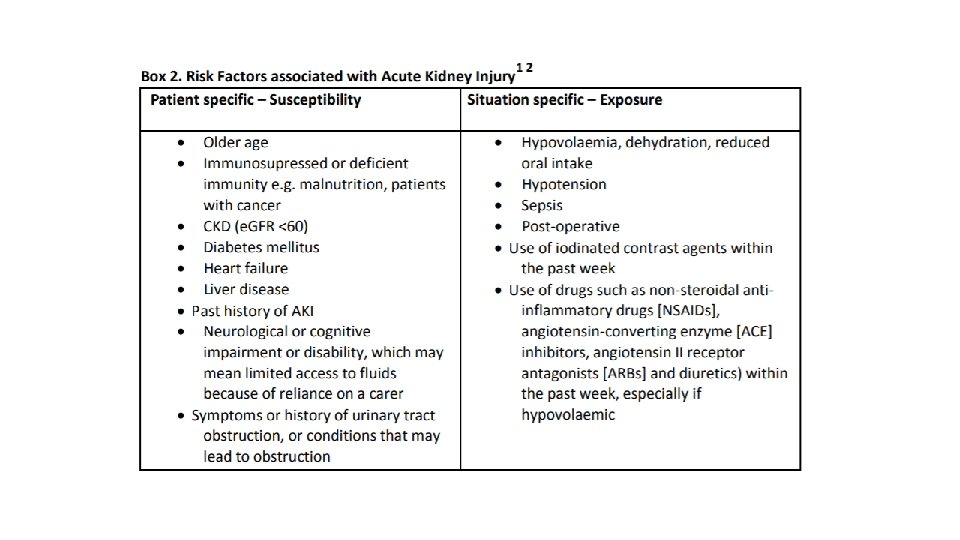
Etiology • prerenal causes decreased renal perfusion (e. g. , hemorrhage, congestive heart failure, and diuretic use , gastroenteritis …. etc. ) ( most common cause in outpatient settings ) • intrarenal causes acute tubular necrosis ( most common intra renal cause , and most common cause of AKI in hospitalized patients ) ischemia and toxic causes interstitial nephritis glomerulonephritis vasculitis hemolytic uremic syndrome cholesterol emboli ……………. . etc. . • postrenal causes urinary flow obstruction (e. g. , benign prostatic hyperplasia and nephrolithiasis) post-operative secondary to bladder manipulation and anesthesia , bladder scans should be performed followed by urinary catheterization
Clinical manifestations and complications • Signs and symptoms related to the underlying disease ( examples? ) • Symptoms of uremia , which are ? • Decreased urine output. • Symptoms of volume overload , which are ? • Muscle weakness , arrhythmias , due to electrolyte and acid base disturbances ( namely hyperkalemia ).
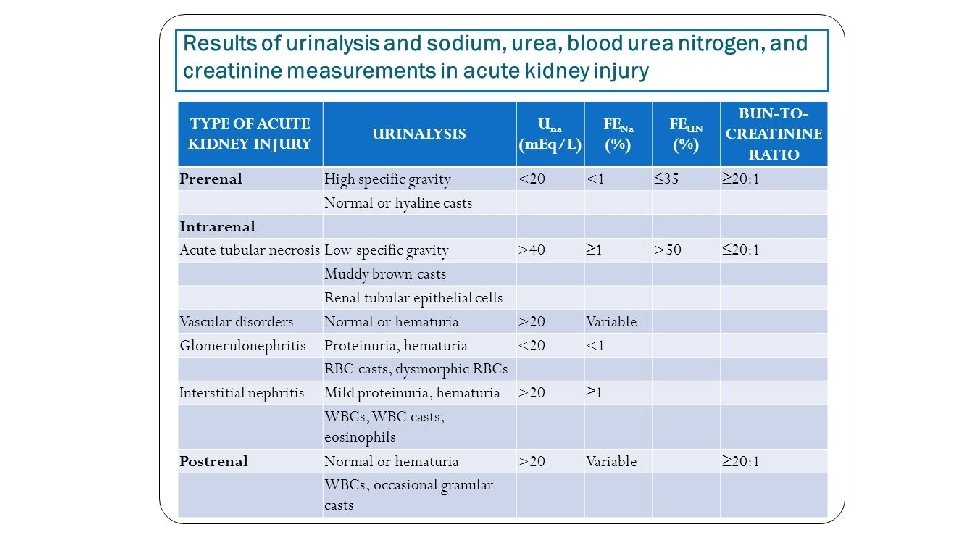
• What laboratory test should be done to help in reaching a diagnosis and possible underlying cause ?
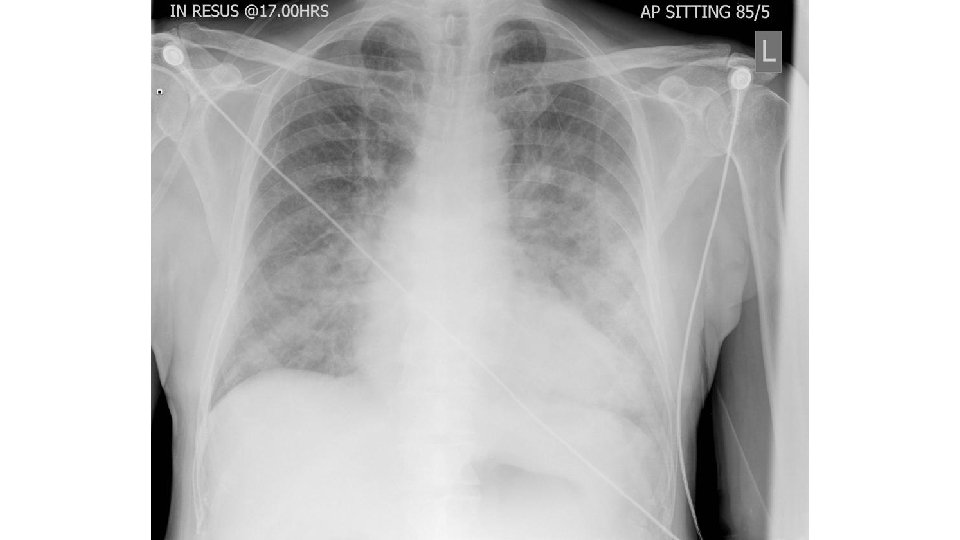
• A 69 -year-old male presents to the emergency department for sudden shortness of breath that came on while he was sleeping. He currently is short of breath, but denies any chest pain, arm pain, or jaw pain. The patient has a past medical history of hypertension, obesity, diabetes, and GERD. The patient states he has not filled his prescriptions for any of his medications in months and cannot remember what his medications are. A chest radiograph is obtained and is seen in Figure B. Lab values at admission are below: Serum: Na+: 139 m. Eq/L K+: 4. 0 m. Eq/L Cl-: 100 m. Eq/L HCO 3 -: 24 m. Eq/L BUN: 22 mg/d. L Glucose: 72 mg/d. L Ca 2+: 9. 9 mg/d. L Mg 2+: 1. 5 m. Eq/L Creatinine: 0. 9 mg/d. L
• The patient is started on appropriate treatment and his symptoms resolve. He is recovering on the medicine floor. His laboratory values are ordered and are below: Serum: Na+: 137 m. Eq/L K+: 3. 5 m. Eq/L Cl-: 100 m. Eq/L HCO 3 -: 26 m. Eq/L BUN: 39 mg/d. L Glucose: 70 mg/d. L Ca 2+: 9. 7 mg/d. L Mg 2+: 1. 5 m. Eq/L Creatinine: 1. 5 mg/d. L The patient states that he has not urinated in the past 24 hours. Which of the following is the most likely cause of this patient's current presentation?
a. b. c. d. e. Furosemide Intrarenal kidney injury Urinary tract obstruction Chronic kidney disease Cholesterol emboli
Question 2 • A 24 -year old female with no past medical history presents to her primary care doctor complaining of a fever. The fever started two days ago, though she was unable to take temperatures at home and has just felt “hot. ” Review of systems is positive for fatigue, arthralgia, and decreased urine output in the last day or so. She recently completed a course of trimethoprim-sulfamethoxazole for an uncomplicated urinary tract infection. Vital signs are temperature 101. 3 F, heart rate 104 bpm, blood pressure of 114/74, and respiratory rate of 18. Physical exam is significant for a diffuse, non-pruritic maculopapular rash on the torso, but is otherwise normal.
• Lab studies show the following: Sodium 141 m. Eq/L Potassium 4. 4 m. Eq/L Chloride 99 m. Eq/L Bicarbonate 23 m. Eq/L BUN 30 mg/dl Creatinine 2. 1 mg/dl Glucose 102 mg/dl Urinalysis shows pyuria w/many eosinophils and no bacteria. What is the most likely etiology of this patient’s chemistry abnormalities?
A. Decreased renal perfusion secondary to dehydration B. Post-obstructive nephropathy C. Granulomatosis with polyangiitis (Wegener’s disease) D. Sloughing of tubular epithelium into the tubule E. Allergic immune response in the renal interstitium
Question 3 • A 19 -year-old woman is hospitalized for acute kidney injury (AKI) associated with bloody diarrhea that developed after she returned from a trip to South America. She also has nausea, vomiting, abdominal pain, fever, chills, and decreased urine output. Medical history is otherwise unremarkable, and she takes no medications. • On physical examination, temperature is 37. 8°C (100. 0°F), blood pressure is 135/90 mm Hg, and pulse rate is 110/min. The oral mucosa is dry. There is diffuse abdominal pain with guarding. The remainder of the physical examination is normal. • Laboratory studies show haptoglobin 8 mg/d. L (80 mg/L), hemoglobin 5. 2 g/d. L (52 g/L), leukocyte count 20, 000/µL (20 × 109/L), platelet count 36, 000/µL (36 × 109/L), reticulocyte count 7. 8%, serum creatinine 5. 7 mg/d. L (504 µmol/L) and lactate dehydrogenase 2396 units/L. Peripheral blood smear showed many schistocytes and urinalysis many erythrocytes and erythrocyte casts. Urine protein creatinine ratio is 0. 5 mg/mg. • Which of the following is the most likely cause of this patient's acute kidney injury? • A. Acute tubular necrosis B. Hemolytic uremic syndrome C. Postinfectious glomerulonephritis D. Scleroderma renal crisis
Question 4 • A 74 -year-old man was hospitalized 3 days ago for extensive, no purulent cellulitis of the right lower extremity and is now being evaluated for acute kidney injury. He has hypertension, hyperlipidemia, and peripheral vascular disease. His hypertension has been poorly controlled; his last office blood pressure measurement was 165/92 mm Hg. Medications are lisinopril, metoprolol, hydrochlorothiazide, amlodipine, pravastatin, and aspirin. On admission, cefazolin was initiated. • The patient is now afebrile, and his blood pressure has not exceeded 118/60 mm Hg since admission. There is no evidence of orthostasis. The cellulitis has improved since admission. • Since admission, his serum creatinine level has progressively increased from 1. 5 mg/d. L (133 µmol/L) to 2. 7 mg/d. L (239 µmol/L). • Other laboratory studies show urine sodium 45 m. Eq/L (45 mmol/L) (normal range for men, 18301 m. Eq/L [18 -301 mmol/L]), fractional excretion of sodium 2. 3% and fractional excretion of urea 51%. Urinalysis shows specific gravity 1. 015, trace protein, no erythrocytes or leukocytes, occasional granular casts. Kidney ultrasound is normal. • Which of the following is the most likely cause of this patient's acute kidney injury? • A. Acute interstitial nephritis B. Cholesterol emboli C. Normotensive ischemic acute kidney injury D. Prerenal azotemia
Question 5 4) A 50 -year-old man (who smoked one pack of cigarettes/day x 30 years) was admitted with a history of chronic sinusitis, microscopic hematuria and a rapidly rising serum creatinine concentration. Chest x-ray showed a possible cavitary lesion in the right upper lung field. The most likely diagnosis is: a) Lung cancer b) Pauci-immune rapidly progressive glomerulonephritis c) Wegener’s granulomatosis d) Macroscopic polyarteritis nodosa e) Anti-GBM disease
Question 6 • A 76 -year-old male presents to the emergency room. He had influenza and now presents with diffuse muscle pain and weakness. His past medical history is remarkable for osteoarthritis for which he takes ibuprofen, and hypercholesterolemia for which he takes lovastatin. Physical examination reveals blood pressure of 130/90 with no orthostatic change. The only other finding is diffuse muscle tenderness. Laboratory data include BUN: 30 mg/d. L Creatinine: 6 mg/d. L K: 6. 0 m. Eq/L Uric acid: 18 mg/d. L Ca: 6. 5 mg/d. L PO 4: 7. 5 mg/d. L UA: hematuria ( strongly positive ), 2+ protein. Microscopic study shows muddy brown casts and 0 to 2 RBC/HPF (red blood cells/high power field). Which of the following is the most likely diagnosis? a. Nonsteroidal anti-inflammatory drug-induced acute renal failure (ARF) b. Volume depletion c. Rhabdomyolysis-induced ARF d. Urinary tract obstruction e. Hypertensive nephrosclerosis
Question 7 • A 67 y old male is evaluated in the hospital for a rise in serum creatinine , • He was hospitalized for pneumonia 2 days ago and improving on levothyroxine therapy , • He has experienced no episodes of hypotension during his illness , his only other medication is prazosin for BPH , • On O/E his BP is 144/75 , pulse 64 bpm , BMI 34 , • The abdomen is non-tender , normal bowel sounds and suprapubic fullness noted , his urine output is around 1200 during the last 24 hours ,
• Labs : Serum cr : 1. 9 mg/dl ( 1. 2 on admission ) K : 5. 7 Urine analysis : specific gravity 1. 011 , PH: 6, trace leukocyte esterase , 0 -3 rbcs , 0 -5 leukocytes Which of the following is the most appropriate diagnostic test to perform : A- fractional excretion of sodium B-kidney biopsy C-kidney ultrasound D- serum creatinine kinase level
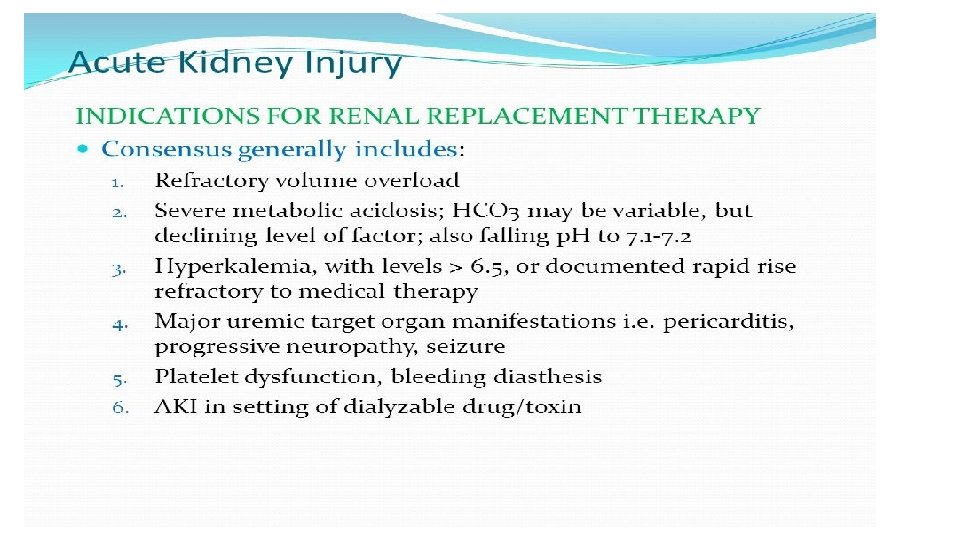
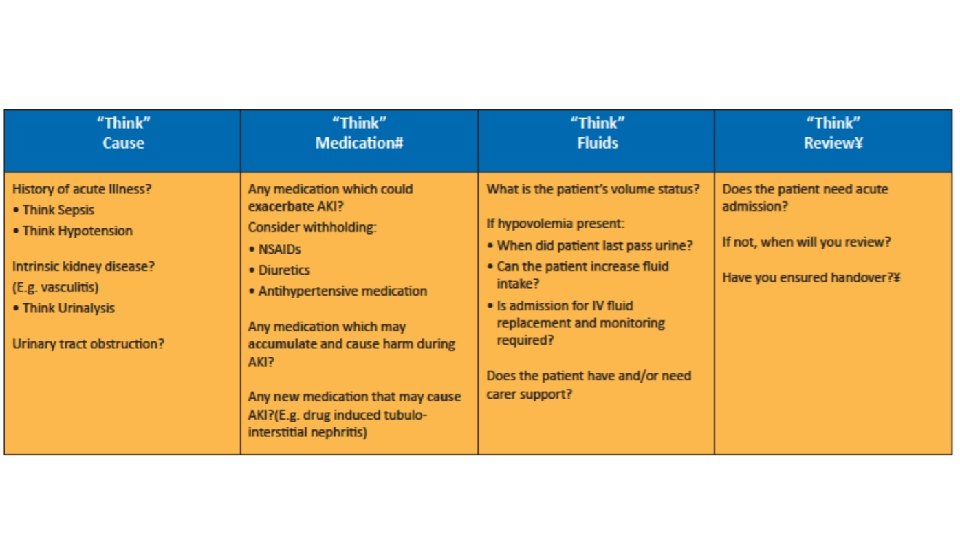
How should AKI be managed ?
Thank you