Airway regional anesthesia for awake fiberoptic intubation From

Airway regional anesthesia for awake fiberoptic intubation From Regional Anesthesia and Pain Medicine, Vol 27, No (March-April), 2002: pp 180 -192 by R 2 黃信豪
 n n Providing anesthetic care to the patient with a difficult airway")
Introduction (1) n n Providing anesthetic care to the patient with a difficult airway keenly interests anesthesiologists. The difficult airway often provokes much anxiety and trepidation.
 • 1. 2. 3. 4. 5. 6. 7. 8. Difficult airways arise")
Introduction (2) • 1. 2. 3. 4. 5. 6. 7. 8. Difficult airways arise from multiple causes: small mouth Receding jaw Reduced mouth opening due to radiation therapy Jaw fracture Previous head and neck surgery Difficulty in neck extension due to prior cervical fusion or advanced osteoarthritis Neck extension is contraindicated in patients with unstable cervical spines due to fx. , rheumatoid arthritis, Down syndrome, etc. Patients who cannot be intubated using direct laryngoscopy due to anatomical variations, even though their airway exam appears normal.
 n In the situation where the airway must be controlled anesthesia must")
Introduction (3) n In the situation where the airway must be controlled anesthesia must be delivered via an endotracheal route, intubation through the use of a flexible fiberoptic bronchoscope is a commonly chosen method

Innervation of the Airway n 1. 2. 3. 4. 5. The airway is divided into: Nasal cavities Oral cavities Pharynx ( consisting of the naso-, oro-, and hypopharynx) Larynx Trachea


Innervation of the Airway – Nose n a. b. n The nasal cavity is entirely innervated by fibers garried by branches of the trigeminal nerve. Ant. Parts of the nasal cavity and the septum – ant. ethmoidal nerve ( a br. of the ophthalmic nerve) The remaining parts of the nasal cavity and the septum – br. of the maxillary nerve, including lateral posterior superior, inferior posterior, and nasopalatine nerves. These branches are relayed through the sphenopalatine ganalion which is situated in the pterygoid fossa lateral to the sphenopalatine foramen at the level of the crest of the superior turbinate

Innervation of the Airway – pharynx n a. b. c. d. Mainly innervated by glossopharyngeal nerve Visceral fibers – posterior third of the tongue, the fauces and tonsillae, epiglottis Special visceral sensation – posterior third of the tongue and soft palate Sympathetic fibers – derived form the carotid plexus and the cervical sympathetic trunk Efferent motor fibers – innervate the stylopharyngeus muscle and join the pharyngeal plexus.
 The superior laryngeal nerve dividing into internal")
Innervation of the Airway – larynx (1) The superior laryngeal nerve dividing into internal and external branch. a. internal br. – through a foramen in the n thyrohyoid membrane and provides visceral sensory and secretomotor innervation to the larynx above the true cords. b. external br. – supplies with motor fibers of the cricothyroid muscle.
 n a. b. c. d. Recurrent laryngeal")
Innervation of the Airway – larynx (2) n a. b. c. d. Recurrent laryngeal nerve providing both structures with fibers for visceral sensation, motor and secretomotor innervation, and sympathetic branches. it enters the larynx by passing the lower border of the inferior constrictor m. of pharnyx. it supplies all muscle of the larynx except cricothyroid and conveys visceral sensation to the cords and infraglottic regions. it is the motor nerve of all intrinsic muscles of the larynx except the cricothyroid muscle.


The airway reflexes The aforementioned nerves participate in several brainstem-mediated reflex arcs. 1. gag reflex – triggered by mechanical and chemical n stimulation of areas innervated by the glosso-pharyngeal nerve, and the efferent motor arc is provided by the vagus nerve and its branches to the pharynx and larynx. 2. glottic closure reflex – elicited by selective stimulation of the superior laryngeal nerve, and efferent arc is the recurrent laryngeal nerve. – exaggeration of this reflex is called laryngospasm. 3. cough – the cough receptors located in the larynx and trachea receive afferent and efferent fibers form the vagus nerve.

Preparation of the patient n Explanation n Sedation n Anti-sialagogues

Explanation The reasons for proceeding with an awake fiberoptic intubation 2. The potential complications 3. The type of airway anesthesia that will be provided 4. Possible alternatives to the proposed anesthetic 1.

Sedation n Adequate sedation is important and advantageous in both the anesthetizing of the airway as well as during the intubation. A calm and comfortable patient is much more likely to cooperate with the anesthesiologist during the procedures. Agents used to produce sedation generally fall into 2 group: benzodiazepines and opioids.

About Benzodiazepines n Advantages: 2. Significant sedation and amnesia Prevent seizure activity in the event of local anesthetic toxicity. n Disadvantages: 1. 2. n Produce unconsciousness Patients can not be cooperative. Midazolam has much to recommend due to quick onset, fairly short duration of action, and lack of pain with injection.

About Opioids n Advantages: 2. Providing analgesia Can help blunt airway reflexes, especially coughing. n Disadvantages: 1. 2. It do not provide amnesia Can cause significant respiratory depression. n Fentanyl, with its relative hemodynamic 1. stability, low cost, and familiarity to most anesthesiologists, is frequently used. Small doses(0. 5~2 mcg/kg) are suggestted.

The antagonists of sedation agents n n Naloxone : 0. 04~0. 4 mg. For opioiddependent patients, as its use can precipitate withdrawal. Flumazenil : up to 5 mg. It may be associated with the production of seizures.

Anti-sialagogues n n n Decreasing oral secretions will aid in the placing and effectiveness of topical agents. Fiberoptic intubation is much easier if excess secretions are not obscuring the operator’s view. For these purpose, glycopyrrolate is the one that is most commonly used due to its lack of CNS effects and relatively lesser likelihood of producing tachycardia.

Local anesthetics n 1. 2. 3. 4. There are three most often used local anesthetic with or without the use of vasoconstrictors: Cocaine Benzocaine Lidocaine vasoconstrictors

Local anesthetics – cocaine n n n Unique in having intrinsic vasoconstrictor properties. It can provide both anesthesia and can help control the bleeding that frequently accompanies instrumentation of the nasal passages. Possible adverse effects: tachycardia, hypertension, dysrhythmias, and seizures

Local anesthetics – benzocaine n n n A water-insoluble ester that is frequently used in a 20% spray to produce anesthesia in mucous membranes. Advantages: 1. available in commercially prepared aerosol applicator; 2. easy to apply to the oral mucosa; 3. produces anesthesia in 15 to 30 seconds. Disadvantages: 1. short duration (5~10 mins); 2. associated with the production of methemoglobinemia after as little as a total of 4 seconds of spraying.

Local anesthetics – lidocaine n n n The most widely used local anesthetic in the world. Advantages: 1. ready availability; 2. relatively low CNS and cardiac toxicity; 3. quick onset; 4. clinically useful duration of action (30 -60 mins for topical application and 1 to 2 hours after infiltration). Disadvantages: 1. toxic plasma levels (>5 mcg/ml) can be reached when moderate amounts of high concentration solutions are used; 2. caution must be used in patients with hepatic dysfunction.

Local anesthetics – vasoconstrictors The advantages of vasoconstrictors with local anesthetics: 1. to prolong the duration of nerve blocks 2. causes mucosal vasoconstriction, which improves visualization during the procedure and helps limit bleeding. n

Topical anesthesia n Spraying n Direct application
 n 1. 2. If nasal intubation is planned, 2")
Topical anesthesia: direct application (1) n 1. 2. If nasal intubation is planned, 2 methods of applying local anesthetics are popular: Cotton-tipped swabs soaked in either lidocaine or cocaine and placed superiorly and posteriorly in the nasopharynx. Then left for several minutes to block the branches of the ethmoidal and trigeminal nerves. Coating a nasal airway with viscous lidocaine mixed with a vasoconstrctor.
 n n n Gargling – not often cover the")
Topical anesthesia: direct application (2) n n n Gargling – not often cover the larynx or trachea adequately. Aspiration – a simple, safe, and effective method of anesthetizing the upper airway. Indirect laryngoscopy and Fiberoptic bronchoscope – for hypopharynx structure anesthetized.
 n n Often more difficult to perform, and carry a higher")
Nerve blocks (1) n n Often more difficult to perform, and carry a higher risk of complications than the above mentioned methods. The common complications of nerve blocks are: bleeding, nerve damage, and intravascular injection.
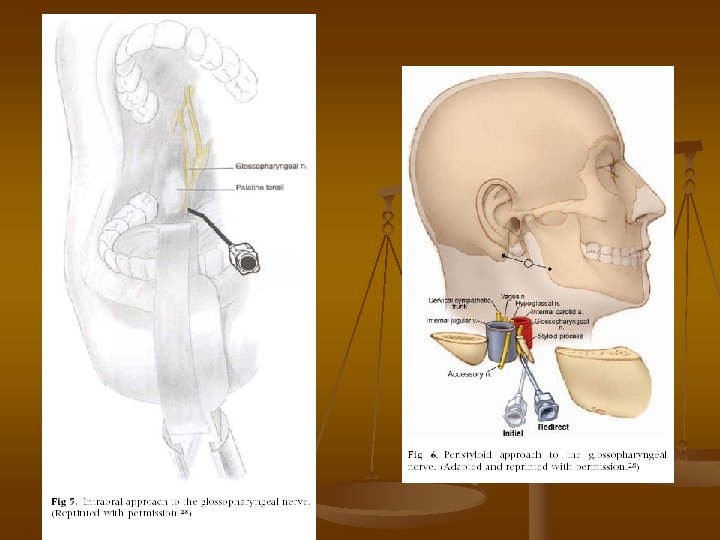
 There are 3 blocks used for upper airway anesthesia: 1. glossopharyngeal")
Nerve blocks (2) There are 3 blocks used for upper airway anesthesia: 1. glossopharyngeal block – for oropharnyx. 2. superior laryngeal block – larynx above the cords. 3. translaryngeal block – larynx and trachea below the cords. n

Glossopharyngeal block n There are two way to approach: 1. intra-oral – need enough mouth opening 2. peristyloid – require the ability to distinguish the bony landmarks. n For both approaches, careful aspiration for blood must be carried out prior to injection because the glossopharyngeal nerve is closely associated with the internal carotid a. in these locations and even a very small amount of local anesthetic can cause seizures.

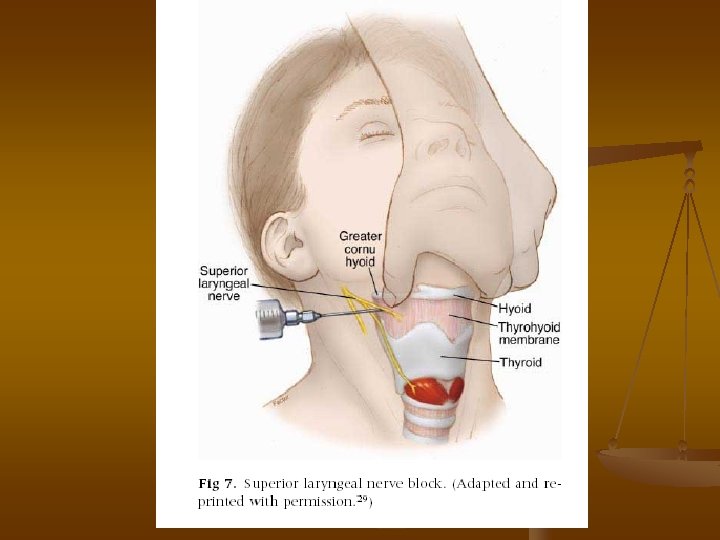
Superior laryngeal block n n n Performing this block requires some degree of neck extension. Need the ability to identify the greater cornu of the hyoid bone and superior cornu of the thyroid cartilage. The hyoid bone can be easily fractured if excess pressure is applied.

Translaryngeal block n n n This is more correctly described as a method of topically applying local anesthetic to the trachea and larynx. The coverage of this method is spotty and is most often inadequate for fiberoptic intubation. The method requires access to the ant. neck and some extension of the head, so that the cricothyroid membrane can be identified.


Thank you for your attention !!
- Slides: 36