Air pollution mechanisms of action of main air




























 - Pre senium: (60")












 Tanathology: describing mechanism of dying, which lead to irreversible desintegration of")


 perzistent state of cerebral death (supratentorial parts) - cortex has")
- Slides: 54
Air pollution – mechanisms of action of main air born irritants Assoc. Professor Jana Plevkova, MD, Ph. D, 2011
Respiratory system It s open system in permanent contact with atmospheric air, and all components it comprises by every breath someone takes Physiological components of atmospheric air are oxygen, nitrogen, carbon dioxide, water vapors and some inert gases – other than these are considered as being pollutants It is well known and defined relationship between particular airborn irritants and airway diseases cigarette smoke – cancer, chronic bronchitis alergenes – bronhcial asthma, hyperreactivity particles of minerals – pneumoconiosis mikroorganisms – infectious diseases physical properties of inhaled air – temperature, humidity
Defensive and protective airway mehanisms protective – they prevent pollutants from entry to the airways defensive – they try to eliminate noxas and mucus out of the airways reflex & nereflex mechanisms breathing pattern changes apnoic reflex sneezing sniffing exspiration reflex cough bronchoconstriction warm/humidity countercurrent filtration of particles Waldayer ly filter airways fluids with AM prop. MCT immunocompetent cells proteases/antiproteases oxidants/antioxidants
Historically recognized episodes of air pollution Meuse Valley in Belgium in 1930 Donnora, Pensylvania USA 1948 London 1948 In the past, most of the air born pollutants, mainly sulfur oxides were products of coal combustion (for heating purposes) in private houses Recognized bad impacts on human health pushed government in GB to establishment of regulations in the force to decrease air pollution – so they established „Clean Air Act“ in 1956 – the consequence was switch from coal heating to gas heating, thus reducing negative impact on human health
Main sources of outdoor pollution - combustion of fossile fuels - traffic – lots of cars, crowded in cities - industry – mainly petrochemical and metalurgical industry - volacnic erruptions, forrest wildfires Lets say – these are molecules coming mainly from traffic and industry and they influence pupulation of particular region
Main sources of indoor pollution There had been identified more than 300 volatile substances in the buildings – considered as being indoor pullutants they come from building materials stains, panitings cleaners, fumes cigarette smoke In the 1980 „sick building syndrome“ had been described – its defined as onset and progression of any symptoms and signs induced by the stay in these „polluted – contamind“ spaces with increased concentration of indoor pollutants (headache, weakness, fatigue, dizziness, nausea) Presence of considerable concentration of indoor polutants is usually underestimated. The evidence could be growing incidence of occupational respiratory diseases.
Classification of air born pollutants based od physical and chemical properties 1. gases ( example: O 3, NO 2, SO 2, CO) 2. vapors, fumes, aerosols – chlorine, Cd. O, acid aerosols 3. anorganic particles – niclkel, asbestos, sillicon - compounds 4. oranic particles (polleen, cirn dust, benzpyren) 5. radioactive gases (radon) and radionuclides 6. mixtures – cigarette smoke, diesel engines exhalates
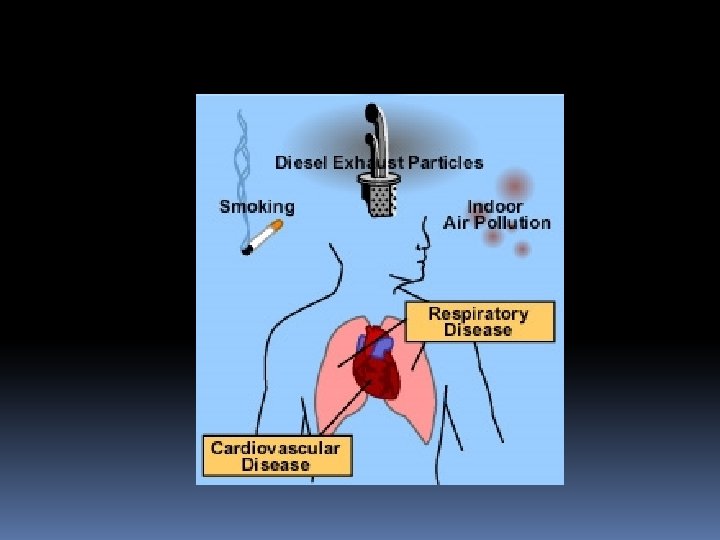
Impact on human health Final impact of air born irritants depends on atmosphere, which significantly change properties of pollutants Important is also humidity, sun shine (photoeffect), presence of different microparticles in the atmosphere, which may turn primary pollutants into secondary pollutants, some of them are even more toxic The question is – if they are so heterogenic with different chemical properties, how do they influence airways? Why do they induce similar symptoms? And have similar effects? TRPA 1 channel – expressed on afferent nerves in airways. Is relevant for majority of air born pollutants, they activate the channel by covalent modification of the AA on the N terminus of the molecule Activation of TRPA 1 induces the sensation of airway irritation, chest tightness, urge to cough, may interfere with pathogenesis of inflammatory processes through neurogenic inflammation
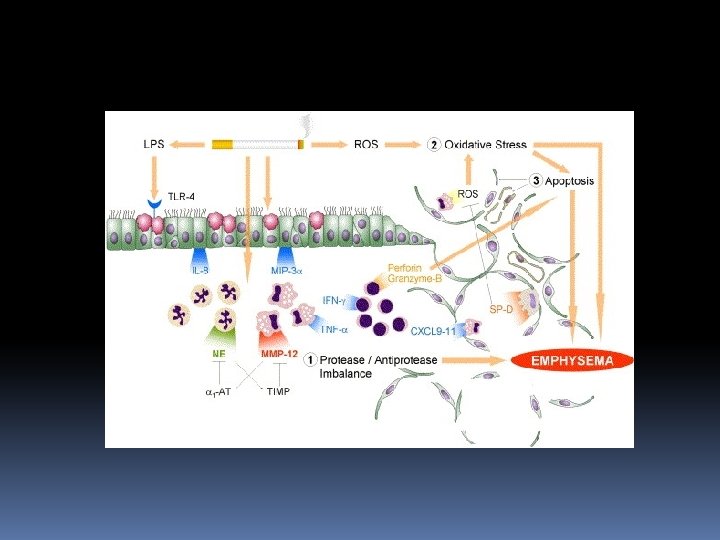
Source: http: //www. ncbi. nlm. nih. gov/pmc/articles/PMC 2735846/figure/F 1/
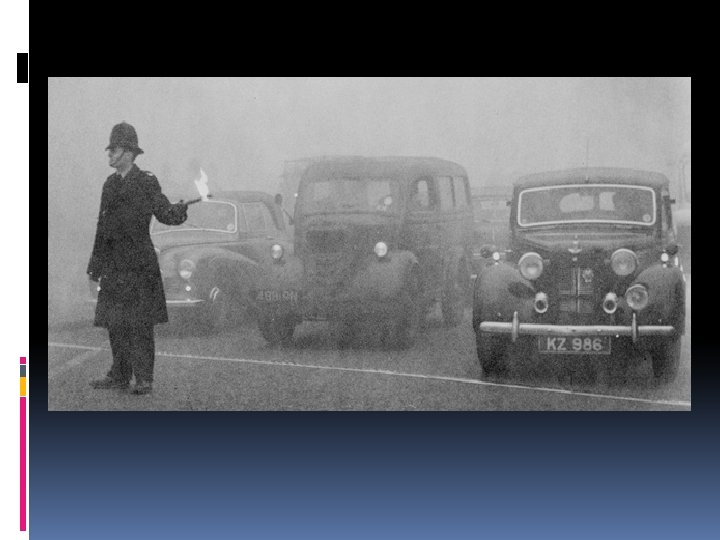
Types of air pollution London type - historic term describing air pollution in London in 50 ´s - sulphur oxides, aerosols of sulphuric acid and particular salts, particles from combustion of fossile fuels, mainly coal Annual mean pollution in London, 1958 -1974
Los - angeles type - Primary source for this kind of pollution is traffic a lots of cars in cities, crowded and busy traffic – produced pollutants are mainly nitrogen oxides and aromatic carbohydrates Sun shine – (UV component) is critical for the creation of secondary compounds, pollutans, with increased toxic capabilities like ozone, aldehydes, ketones, peroxyacylnitrites
Air quality index
Entrance of the pollutants to the body At rest and mild physical exercise humans preffere nasal breathing turbulent airflow counter current heat/moisture exchange impaction and filtration of corpuscular pollutants dilution of gases Pharmacokinetics depends on the solubility and secondary chemical processes in the superficial fluid layer, and also on capabilities of pollutants for difusion Deposition of corpuscular pollutants depends on aerodynamic diameter, Larger particles are trapped within the upper airways, while smaller penetrate deeper to the airways
Pollutants may initiate protective and defensive reflexes (sneezing, coughing, urge to cough, sensation of airway irritation, dyspnoe, chest tightness High concentration of irritants may induce overproduction of mucus with altered chemical properties (viscosity) and dysregulation of cilliary movemement – leading to disturbances of MCT The result might be stagnation of the mucus, obliteration of small diameter airways, with possible growth of bacteria In case that pollutants hit the alveolar system it may lead to activation of alveolar macrophages, which induce inflammytory and fibrotic response of the lung tissue Activation of proteases, oxidative stress – direct damage to the lung tissue
Toxic influences Sulphur dioxide SO 2 is completely resorbed in the nasal cavity and upper airways In peripheral airways it may work in transformed form, absorbed on particles, or in form of acid aerosol, and it may slow down or completelly stop MCT Irritation of the vagus nerve terminals may lead to bronchoconstriction In case of repeated exposition to lower concentrations – chronic inflammatory changes might be induced by activation of proteolytic enzymes, mediators and reactive oxygen species released from inflammatory cells
Ozone Represents appx 50% of all oxidizing substances In case of nasal breathing 80% of ozone is absorbed in upper airways Deep breathing, or oral breathing may bring ozone deeper to the lungs Acute exposure induces inflammatory changes with PMN infiltration and epithelial shedding Longer exposition may increase permeability of airway epithelium It contributes significantly to airway hyperreactivity
Nitrogen oxides Important environmental pollutant, but also indoor in case of gas operating owens or cookers Easily penetrates to the peripheral airways Decreases resistance agianst bacteria, and may damage alveolar macrophages In combination with O 3 a SO 2 enhances bronchoconstrictory reaction in asthmatics
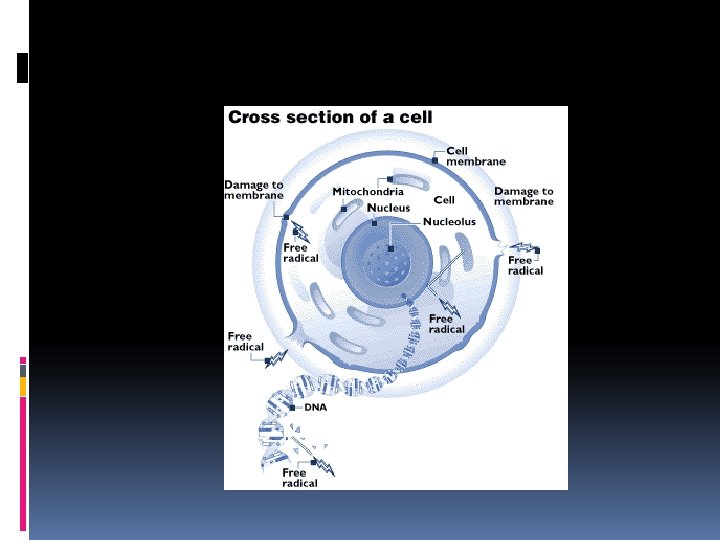
Mechanisms of action Production of reactive oxygen species in the tissues – oxidative stress, with direct damages to the membranes, peroxidation Oxidants react with molecules present in the superficial musocal fluid (unsaturated fatty acids, cholesterol, tryptophane and other) with production of ROS, aldehydes and peroxides Release of chemotactic factors – attraction of immunocompetent cells Oxidative stress causes lipid peroxidation thus increasing permeability of cell membranes
Diesel engines The most important souce for PM 10 Corpuscular pollutants are danagerous because they are capable to prolong the contact of any other pollutans absorbed to them, attached to them with the mucosa – allergenes for example. Interaction of PM 10 & polleen grain – release of specific proteines - submicroscopic allergenes
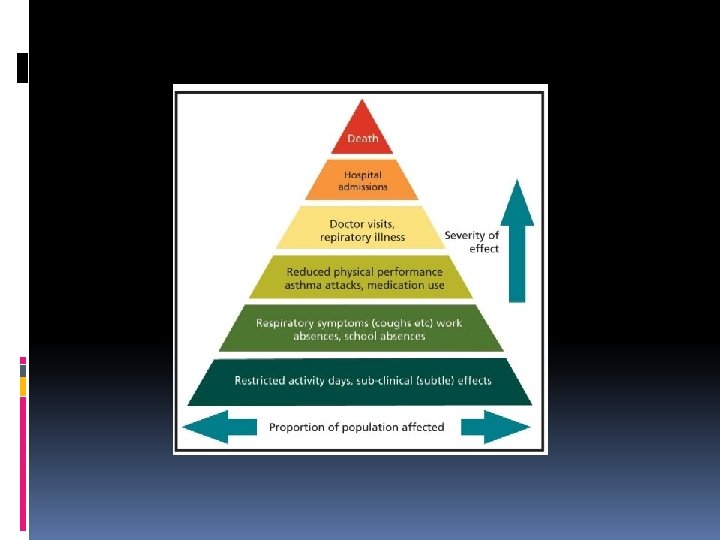
The role in pathogenesis of airway diseases Morbidity & mortality – in case of respiratory and cardiovascular diseases we can see an increase of them, mainly due to unpleasant weather conditions The rise correlates with the rise of O 3 & SO 2 Pollutants are being considered the risk factors for chronic respiratory diseases
London in the winter 1962
RADS – reactive airway dysfunction syndrom Brooks described consequences of acute exposure to air born irritants as an onset of symptoms similar to asthma in predisposed individuals cough, wheezing, irritation of airways, chest tightness in the interval up to , tla na hrudi a dýchavice do 24 hodín po expozícii iritanto hours after irritant exposure lung function test may reveal limitation of exspiratory airflow positive methacholine provocation test The most common causes for RADS are gases solubile in watter with drop of p. H (sulphur and nitrogen oxides), which have same time high oxidizing potential, formaldehyde, paraformaldehyde, isocyanates, organic volatile substances, chemicals for desinfection – mainly with chlorine, and many other
Relationship between airway diseases and pollutants Astma a alergies, chronic respiratory diseases Risk factors a) Irritation of mucosa may lead to airway hyperreactivity (neurogenic inflammation) b) Toxic effects on epithelium – increase of its permeability for inhaled aerosols, alergenes, and disturbances of MCT – all of these may lead to longer exposure to allergenes without appropriate airway cleaning excerbation of asthma, COPD, occupational diseases
Neurogenic inflammation Pollutants/irritants stimulate airway nerves via ion channels such are TRP channels, or acid sensing channels – nerves – mainly C fibers share afferent information to the central nervous system, but same time, they can release neuropeptides – neurokinin A, neurokinin B, Substance P, CGRP, VIP and many other. These neuropeptides could further stimulate nerves around, and also have proinflammatory potential – they can induce vasodilatation, constriction of bronchial smooth musles, increase glandular activity, increase epithelial permeability Ongoing chronic inflammation in ariways – even at subclinical level – may lead to airway hyperreactivity
TRPA 1 relevant molecules induce neurogenic inflammation
An example for cigarette smoke induced lung damage via activated macrophages & neutrophils, with reease of proteases, matrixmetaloproteases MMPs – leading to COPD
PATHOPHYSIOLOGY OF AGEING, TERMINAL STATES AND DYING
Ageing Aging is gradual process of the progressive decrease of vitality, increase of vulnerability of tissues, leading to death It is a process which is mandatory for every living creature, from the very begining of its existence Speaking in medical terms - it is a complex of somatic changes since the end of the growing and maturation phase till the death of the organism Same time the organism is undergoing aging processes, we can say, there is increased incidence of diseases, so it is difficult to say, which changes are due to aging only, and which are due to associated diseases
WHO – categories - Middle age: (45 - 59 yrs) - Pre senium: (60 - 74 yrs) - Senium (old): (75 - 89 yrs) - Very old more than 90 yrs
Population is aging increased and improved quality of life in senior categories better diagnostic options and treatment of diseases which were fatal before
100 1980 % survivors 1930 1900 1840 50 0 0 20 40 60 80 100 age in years
Mortality in 80 -89 yrs interval within 1950 -1995 Japan France Sweden U. K. U. S. A.
MAIN CHARACTERISTICS OF AGEING 1. Rise of mortality with age 2. Changes of biochemical processes 3. Progressive weakness of physiological functions 4. Decreased ability of adaptation 5. Increased susceptibility to many diseases
Somatic changes during ageing At the cellular level - the number of postmitotic cells declines, and cells which are still capable of mitosis decrease their activity At the tissue level – disturbance of the tissue structure, increase of the cells volume whereas their count is reduced, decrease of the ellastine content, increased accumulation of „altered“ colagene, thickness of IST – limitation in oxygen and substrate supply
Organ changes Myocardium – hypertrophy & fibrosis, disturbances of valves, decrease of CO Vessels – increased rigidity of arteries due to disturbed ratio between collagen and eelstic fibres, deposition of calcium + ATS leads to increased periheral resistance – rise of BP Blood – anaemia die to decreased Fe reabsorbtion, rise of RBC sedimentation, decrease count and activity of WBC, increased tendency to blood clotting due to changed PLT properties Kidneys – decrease of GF & Q in kidneys, creatinin not increased, bc of muscle atrophy (no much sources for creatinin) Respiratory system – decreased compliance, VC, worse diffusion properties, attenuated defensive reflexes + MCT – increased risk for respir, infections
Organ changes Git – dysphagia, hiatal hernia, diverticulosis, reduced motility, digestion and reabsorbtion of nutrients, liver atrophy with decreased functions Endocrinne system – decrease of STH, changes of FSH LH after menopause, decrease of T 3, decreased glucose tolerance, fibrosis and sclerosis of B cells Skelet and muscles – atrophy for both, decreased ablitities for cartilage regeneration Skin – atrophy & decreased regeneration capabilities of epidermis, wrinkles due to lack of ellastic structures and decreased amount of subcutaneous fatty tissue, grey hair due to decreased melanin synthesis NS – neuronal atrophy, inadequate supply by oxygen and substrates, disturbanced of brain main arteries, , NS – neuropathy Decreased abilities of senses Metabolism – decreased speed, decreased production of heat
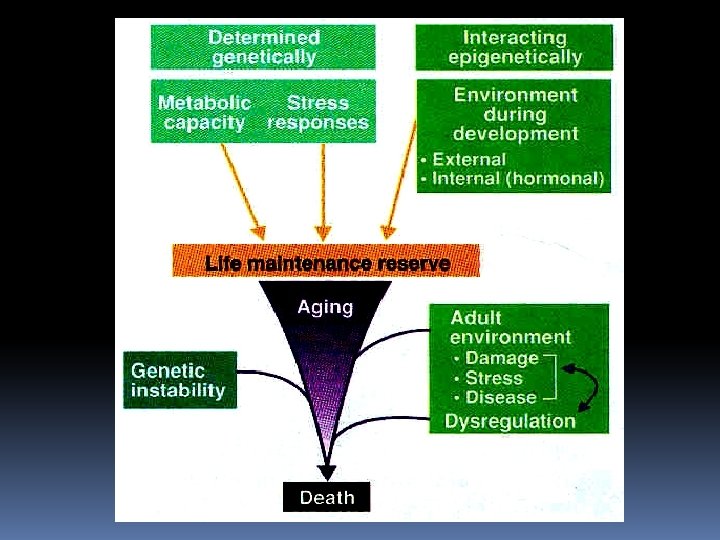
Theories of ageing systematic punishment of tissues at molecular, cellular, and finally organ level 1. Nutrishment immediatelly after the birts influences duration of life 2. Accumulation of somatic mutations – correlation between ability to repair damaged DNA and duration of the life 3. Increased exposure to stress factors may lead to premature ageing 4. As the age goes, there is an accumulation of toxic metabolic products - peroxides & ROS, glycation of macromolecules -Decreased ability of antioxidant and reparative processes – leading to accumulation of potentially „ bad“ molecules
Genetic factors all species have geneticly determined duration of life, & its more or less constant & its number of mitotic processes in particular cells is limited defect synthesis of proteins – gene products due to increased number of somatic mutations same time, reparation of DNA is limited ageing genes – indirect evidences
Lessons we have learned from disorders such Wislons´s syndrom or progeria suggest that aging is multifactorial process based on genetics. We also have information for longevity subjects.
Immune factors Increased number of somatic mutations induces changes of expression of surface antigenes – thus IS is not able to recognize them – and takes them as strangers Whereas immunity decreases with age, activity of autoimmune processes is on rise We can see increased production and release of cytokines – mainly Il 1, Il 6, TNF Increased amount of growth factors - TGF , IGF, b. FGF – those may contribute to unregulated overproduction of extracellular matrix and amyloid deposition to the organs, and vessels – progression of fibrotic changes
genetic predisposition inflammation diseases & tissue damage healthy food accumulation of cell deffects healthy life style štýl random changes at the level of macromolecules stress, oxidation stress environmental pollution, smoking food, toxins, conservants
TERMINAL STATES (TS) Tanathology: describing mechanism of dying, which lead to irreversible desintegration of organism 1. Preagonal stage: interaction of 2 antagonistic efforts a) One leading to the dezintegration of the organism due to pathological processess (hypoxia, acidosis, hypoperfusion) b) Second represent defensive and compensatory mechanisms (tachypnoe, tachycardia, vasoconstriction, hypertension) -Exhaustion of compensatory reactions leads to -preterminal apnoe, lack of EEG activity, AV blocks with preautomatic pause, hypotension and tissue hypoperfusion
2. Agonal stage chaotic function of different systems, which is not responsing to cortical control and regulatory mechanisms, subcortical centres and reflex mechanism are more common a) gasping b) Adamsov - Stokesov syndrome c) unconsciousness 3. Clinical death: unconsciousness, apnoe, asystolia - CPR may lead to fully recovery of all functions, limiting factor is TIME – 30 min of CPR, sometimes even longer in hypothermia
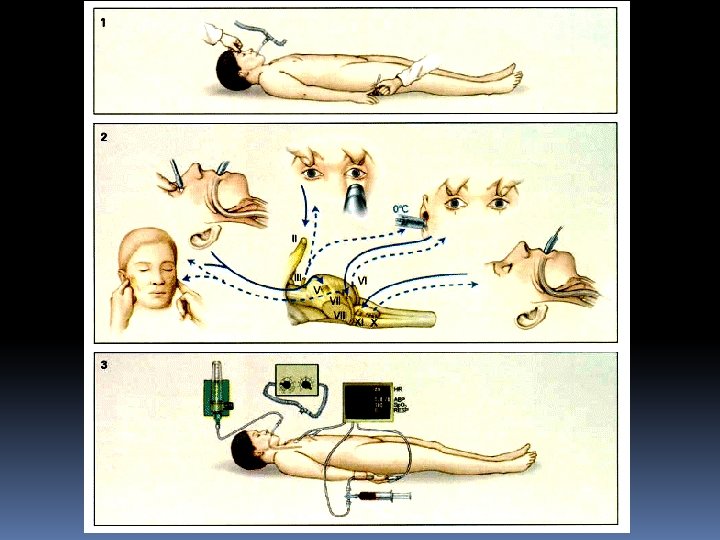
4. Biological death Onset and development of irreversible pathological changes, depends on the vulnerability of tissues and their Sensitivity to the lack of oxygen BRAIN death Lack of spontaneous breathing for 15 min Lack of voluntary and unvoluntary movements Lack of reflexes (brain), spinal reflexes might be present Lack of cortical and brainstem evoked potentials Mydriasis with no fotoreaction - Most important tests: isoelektric EEG, no brain perfusion detected by radiography, increase of ICP, decreased a - v O 2 difference in cerebral circulation
Vegetative state (apalic syndroma) perzistent state of cerebral death (supratentorial parts) - cortex has been damaged, and this is irreversible in case that brainstem is working we can have spontaneous breathing, reflex swallow, spontaneous eyes open, movement of eyes in a way suggesting the patient is watching you and does react