AIM Why important Intervention Intensive Nursing care stroke






 C=Thalamus hemorrhage")
 เลอด Brain )12%( เนอสมอง )78%(")







 •")
 2. Central 3. Cingulate (subfalcine) 4. Transcalvarial -")
 ถกกด หผปวยเสยชวตไดในเวลาอนรวดเรว")













- Slides: 51
AIM �Why important ? �Intervention �Intensive �Nursing ? care ?
stroke
HEMORRHAGIC STROKE � hemorrhagic stroke มอตราการเสยชวตสงประมาณ รอยละ 305 -0 ในชวงระยะ 30 วน � Ischemic stroke มอตราการเสยชวตว นประมาณรอย ละ 20 )Ref: grysiewicz RA. epidemiology of ischemic and hemorrhage stroke. Neurol Clin 2008( ในชวงระยะ 30 วน
CAUSES
HEMORRHAGIC STROKE – SIGNS AND SYMPTOMS Hemorrhagic �Subarachnoid hemorrhage Sudden severe HA Transient LOC Nausea/Vomiting Neck pain Intolerance of noise/light Stiffneck positive �Intracerebral hemorrhage LOC , N/V , Coma Sudden severe HA Transient LOC Nausea/Vomiting Neck pain Intolerance of noise/light Stiffneck positive
COMMON SITE FOR HYPERTENSIVE HEMORRHAGE
COMMON SITE FOR HYPERTENSIVE HEMORRHAGE A=Lobar hemorrhage B= Basal ganglia hemorrhage(Putam en) C=Thalamus hemorrhage D=Brainstem hemorrhage(pons)
COMPONENT OF BRAIN CSF (10%) เลอด Brain )12%( เนอสมอง )78%(
INCREASES IN BLOOD Focal brain damage • hematoma Herniation = Coma, death • vasodilation Decrease cerebral perfusion • hypoventilation • hypercarbia / hypoxia • venous outflow
HYPERTENSION Increase brain edema Increase hematoma size Increase intracranial pressure
ROLE OF TREATMENT �Decrease �Prevent �Control hematoma growth brain herniation Risk and specific treatment for prevent recurrent events Blood pressure control
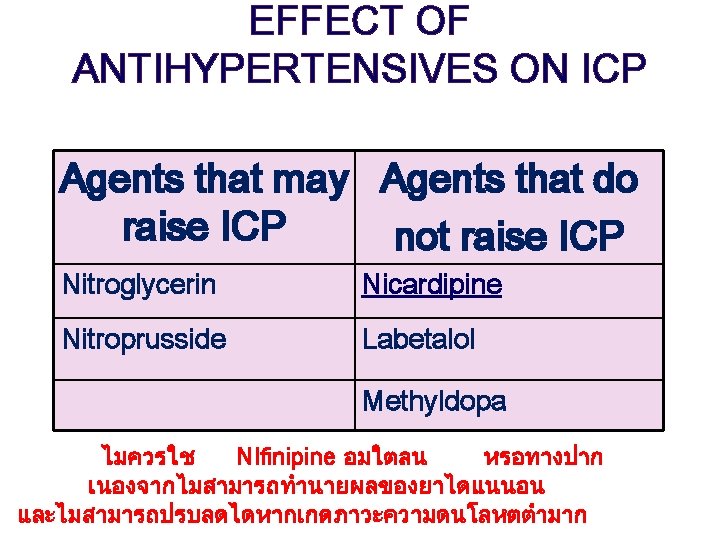
INTERVENTIONS 2. Blood pressure �A goal reduction of 30% of initial presenting MAP to avoid hypotension and potential ischemia is usually recommended BP goal 160/90, 160/100 mm. Hg �Hypertensive hemorrhage keep BP < 180/105 mm. Hg or MAP< 130 �Ischemic stroke keep BP < 220/120
INTERVENTIONS 3. Temperature BT >38. 5°C - Medicine: Acetaminophen - Tepid Sponge - cooling blanket
INTERVENTIONS 4. Fluid&Electrolyte - Avoid dehydration & Overhydration ปรมาณสารนำทควรไดร บ = urine out +500 ml (insensible loss) +300 ml/1°C ทเพมขนจาก อณภมกายปกต (37°C( - control electrolyte balance
NURSING INTERVENTIONS 8. Temperatureในรายทมการตดเช ออาจตองให ATB 9. antihypertensives, osmotic diuretic 10. IV fluid ประเมน intake & output ความตงตวของผวหนงและเยอบ ตางๆ ตดตามคา serum & urine osmolality 11. ประเมน bowel sounds
IICP Normal 4 -15 mmhg • Decrease CPP cerebral ischemia (CPP =MAP –ICP) • Brain herniation • brain injury (brian stem) • ischemic • death
- Supratentorial herniation 1. Uncal (transtentorial) 2. Central 3. Cingulate (subfalcine) 4. Transcalvarial - Infratentorial herniation 5. Upward (upward cerebellar or upward transtentorial) 6. Tonsillar (downward cerebellar)
BRAIN HERNIATION cardiovascular center, respiratory center ทกานสมอง (brain stem) ถกกด หผปวยเสยชวตไดในเวลาอนรวดเรว
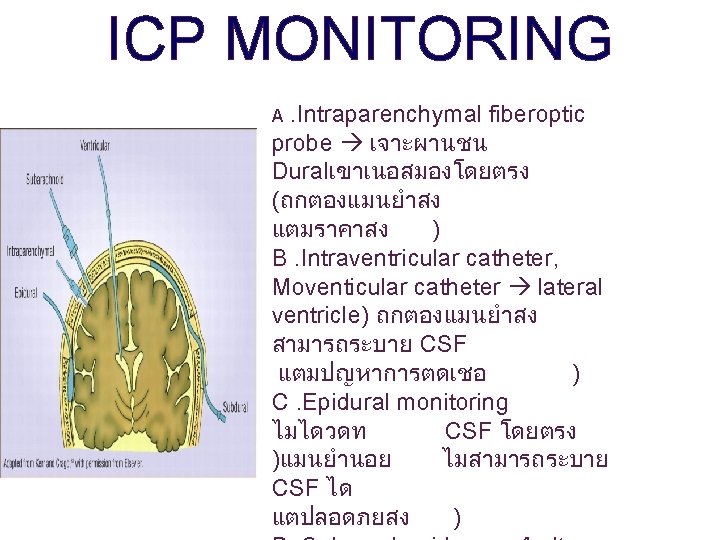
ICP MONITORING
CLINICAL MANIFESTATIONS IICP Cheyne-Stokes respirations
CLINICAL MANIFESTATIONS IICP
INTERVENTIONS 1. ตดตามคา ICP, CPP, V/S & arterial pressure 2. การรกษาดวยการผาตด – ventriculostomy ระบาย CSF – craniotomy or craniectomy decompression
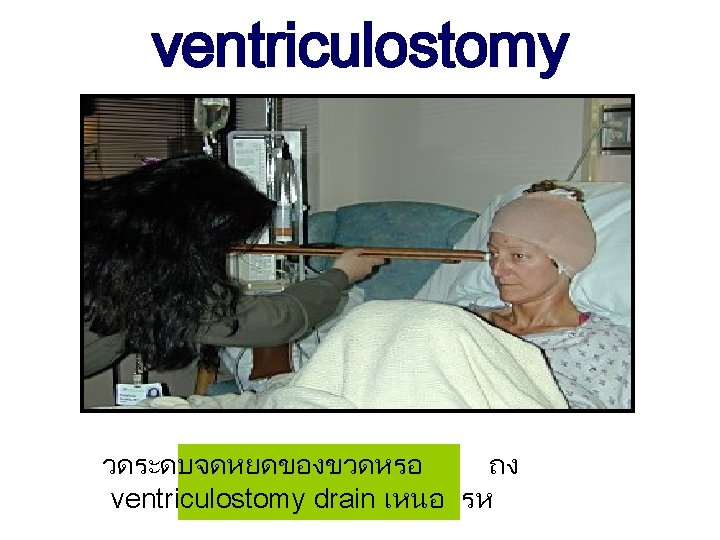
ventriculostomy
VENTRICULOSTOMY The laser level in position to ensure the panel is positioned at the "zero"
INTERVENTIONS 3. การรกษาดวยยา ไดแก �barbiturate; pentobarbital, thiopental barbiturate coma ลด brain metabolism, cerebral oxygen consumption & cerebral blood flow ลด ICP **ระวงภาวะ hypotention �เพม CPP ลด ICP ; Dopamine, Phynylephrine �osmotic diuretic ; mannitol serum osmolality เพมขน ดง free water จากเนอสมอง �steroid ; decadron ลด brain edema,
ASSESSMENT GCS < 8 คะแนน coma GCS = 3 คะแนน deep coma
ASSESSMENT �pupil reaction to light normal �pupil sluggish to light จาก N 3 ถกกด (oculomotor nerve) สาเหตจาก brain herniation, brain edema �pupil dilate > 6 ml. & non reaction to light coma พบรวมกบ N 3 ถกกด �ผดปกตขางใด
NURSING COMPLICATION PRECAUTION � VAP � SSI � UTI � Pressure sore � joint stiffness/DVT (Erly rehabilitation)
HOME PROGRAM