Aging of the Urinary Tract Kidney Lower Urinary





 • secreted by")















- Slides: 22
Aging of the Urinary Tract: Kidney Lower Urinary Tract
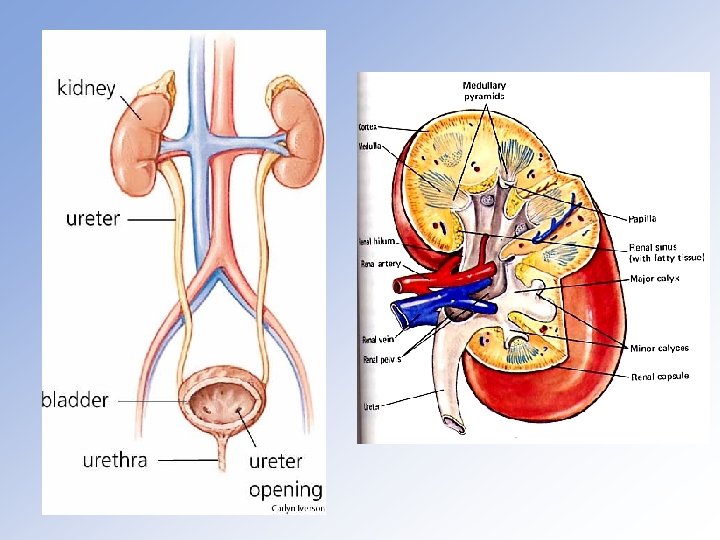
Nephron & Renal Circulation
Table 19 -1 Major Functions of the Kidney Water and electrolyte regulation Metabolic products excretion Hydrogen ion excretion and maintenance of blood p. H Endocrine functions: Renin-angiotensin secretion (blood pressure) Vitamin D activation (Ca++ metabolism) Erythropoietin secretion (hematopoiesis)
Renal Glomerulus: Tufts of capillaries between afferent and efferent renal arterioles. Filtration is through a fenestrated endothelium separated from the basal membrane by podocytes. Filtrate is the same as plasma but without proteins.
Renal Tubules divided into: • Proximal Tubule, mostly reabsorption of water & solutes • Loop of Henle, mostly reabsorption of water & salt • Distal Tubule, mostly water & salt (under influence of aldosterone) reabsorption and acidification of urine • Collecting Duct, water reabsorption under the influence of ADH (antidiuretic hormone from posterior pituitary)
Distal and Collecting Tubules function is regulated by ADH (antidiuretic hormone) • secreted by neuroendocrine hypothalamus • stored and released from the posterior pituitary Juxtaglomerular Apparatus: • located between affarent artery and distal tubule • secretes the enzyme renin • renin acts on the liver protein angiotensinogen to form angiotensin I, and angiotensin is transformed into angiotensin II in the lungs • angiotensin II is a very potent hypertensive substance; it also stimulates the release of aldosterone from the adrenal cortex
Hypothalamus, Posterior Hypophysis, and their Hormones Hypothalamus
Figure 19 -2
Table 19 -2 Common Renal Problems in the Elderly Renal Failure Impaired drug excretion Urinary tract infections Hypertension Miscellaneous disorders: Tuberculosis Nephritis Diabetes, etc.
Table 19 -3 Some Signs of Renal Failure Generalized edema Acidosis Increased circulating non-protein nitrogen (urea) Increased circulating urinary retention products (e. g. creatinine, uric acid)
Table 19 -4 Selected Causes of Acute Renal Failure PRE-RENAL: Loss of body fluids Inadequate fluid intake Surgical shock or myocardial infarction RENAL: Drug toxicity Immune reactions Infectious diseases Thrombosis POST-RENAL: Urinary tract obstruction
Table 19 -6 Drugs and the Aging Kidneys Questions: Is the drug excreted primarily by the kidney? How competent are the kidneys? What are the side-effects? What are the consequences of drug toxicity when the kidney is impaired? Etiopathology of Renal Drug Toxicity: High renal blood flow Increased drug concentration and accumulation in kidney Increased hepatic enzyme inhibition in the elderly Increased autoimmune disorders in the elderly
Functions of the bladder • Filling with urine from the kidneys • Micturition: emptying of bladder by muscle contraction and opening of sphincters. • Principle muscle: Detrusor muscle • Sphincters: Internal (involuntary; smooth muscle) and external (voluntary to some degree; skeletal muscle)
Figure 19 -5
Figure 19 -6
Table 19 -7 Physiologic Requirements for Continence Motivation to be continent Adequate mobility and dexterity Normal lower urinary tract function Adequate cognitive function
Table 19 -7 Physiologic Requirements for Continence Storage: No involuntary bladder contractions Appropriate bladder sensation Closed bladder outlet Low pressure accommodation of urine
Table 19 -7 Physiologic Requirements for Continence Emptying: Normal bladder contraction Lack of anatomic obstruction Coordinated sphincter relaxation & bladder contraction Absence of environmental/iatrogenic barriers
Table 19 -8 Age-Related Changes Contributing to Incontinence In Females Estrogen deficiency Weak pelvic floor and bladder outlet Decreased urethral muscle tone Atrophic vaginitis In Males Increased prostatic size Impaired urinary flow Urinary retention Detrusor muscle instability
• Weakness of pelvic muscles • Inability to avoiding when bladder full • overdistended, non-contractile blood • cognitive, emotional problems