Affective Disorders Depression found throughout history unipolar bipolar

Affective Disorders

Depression � found throughout history � unipolar � bipolar or major depression or manic depression

Symptoms of depression � must be evident daily or almost every day for at least 2 weeks � often comorbid with anxiety
 suffering from a")
Depression � Depression ◦ over 10% with ~ 5% (11, 000) suffering from a depressive episode in any given year ◦ untreated - 25 - 30% will attempt or commit suicide ◦ 2 X greater prevalence in women than men ◦ estimated only ~ 50% receive specific treatment ◦ increased rate of and suicide attempts

How do we treat depression? � Pharmacologically ◦ drugs have been available for ~ 40+ years

Pharmacological Txt for Depression � antidepressants typically require 10 – 30 days to start working – full effect may take 6 weeks and in many cases – improvement can continue over several months � what takes so long? ◦ 2 lines of thought ◦ role of upregulation and downregulation of receptors ◦ effects on intracellular processes such as 2 nd messengers and their functions in the neuron

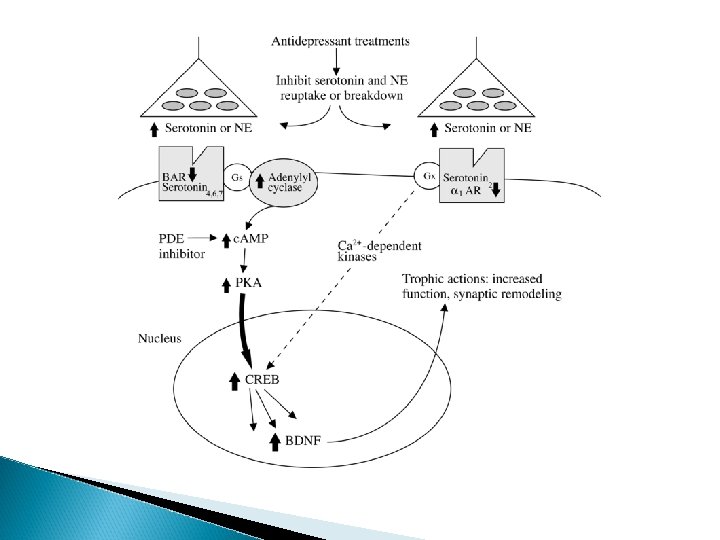
one result of activation of 2 nd messenger system � an intracellular target of 2 nd messenger system is called c. AMP response element binding protein (or c. REB) ◦ CREB increases in the hippocampus with chronic antidepressant medication

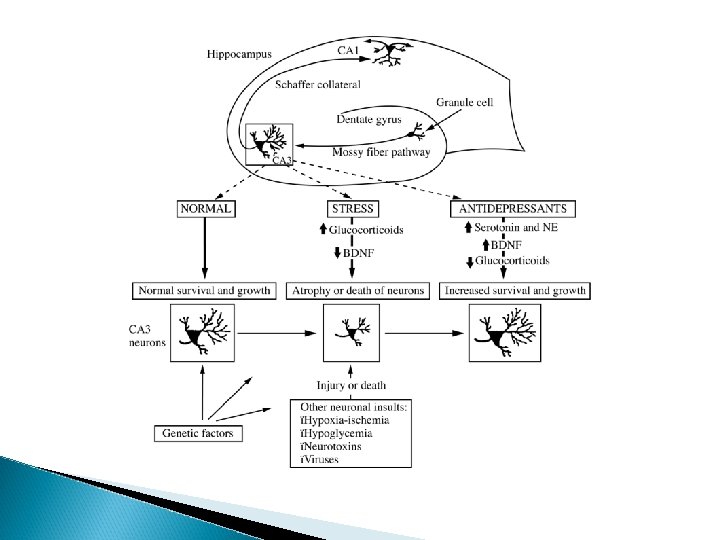
What does CREB do? � c. REB activates genes that control the production of BDNF – a neurotrophin � neurotrophins etc promote neural health, growth,

neurogenic theory of depression �two of the functions of 2 nd messengers is ◦ 1)protect neurons from damage due to injury or damage; ◦ 2) promote and maintain health and stability of newly formed neurons

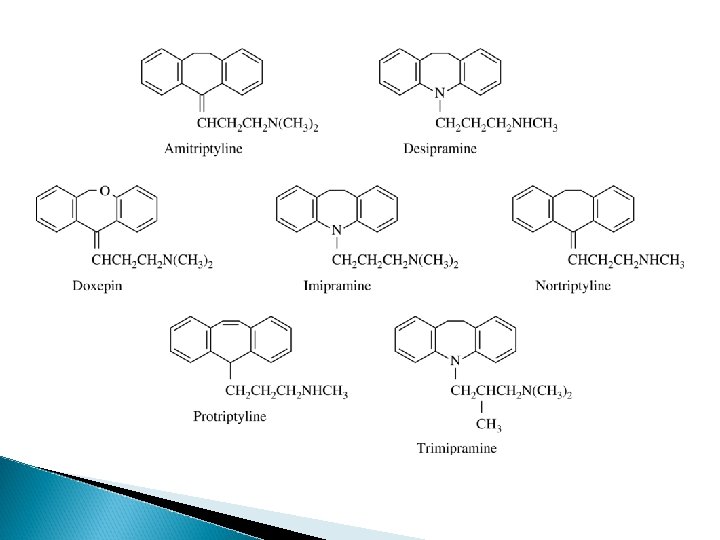
So how do we treat depression? � Pharmacologically ◦ drugs have been available for ~ 40+ years Traditional Antidepressants 1. tricyclic antidepressants

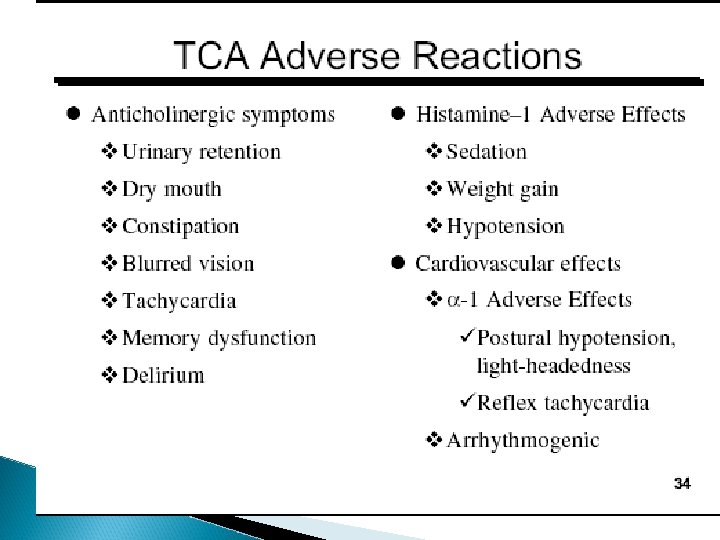
Tricyclic antidepressants � Blocks reuptake of NE and 5 HT � blocks histamine receptors � block ACh receptors � widely used � fairly significant side effects ◦ mainly because they block ACh receptors �blurred vision, dry mouth, urinary retention, irregular heart rate, constipation, sexual dysfunction, ◦ effects on other NT �sedation, weight gain

� tricyclics estimated to be effective in ~ 60 - 70% of moderately to severely depressed individuals


So how do we treat depression? � Pharmacologically ◦ drugs have been available for ~ 40+ years Traditional Antidepressants 1. tricyclic antidepressants 2. MAO inhibitors- MAO - enzyme that breaks down excess DA, NE, 5 HT
 � phenelzine (Nardil) � Isocarboxazid (Marplan) � tranylcypromine (Parnate) � 2003")
MAO inhibitors (irreversible) � phenelzine (Nardil) � Isocarboxazid (Marplan) � tranylcypromine (Parnate) � 2003 – nonselective MAOI selegiline (Eldapril) ◦ transdermal skin patch

MAO inhibitors � mechanism of action: � reversible inhibitors of MAO A – NE/5 HT ◦ moclobemide (Aurorix) – not in U. S. – not particularly effective � MAO B inhibitors - DA ◦ selegiline (Deprenyl- used at low doses for PD)
 than traditional tricyclics or SSRIs particuarly")
◦ proved as effective (if not more so) than traditional tricyclics or SSRIs particuarly for unresponsive depression ◦ not used as first level txt due to risk (or perceived risk) of adverse side effects

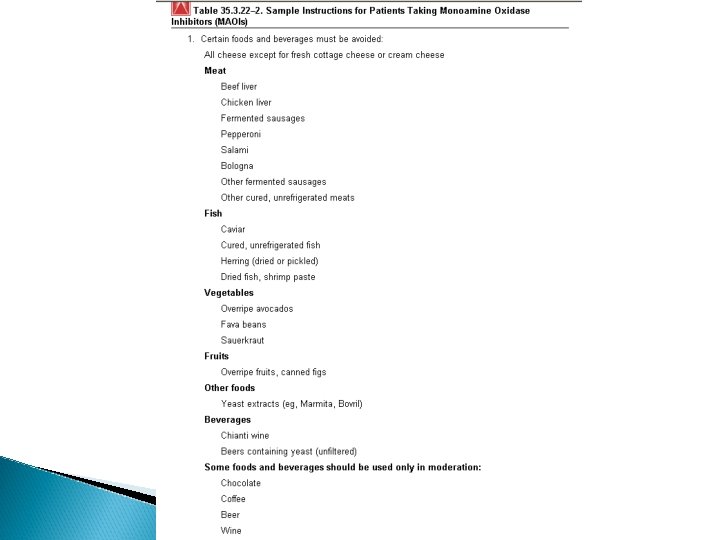
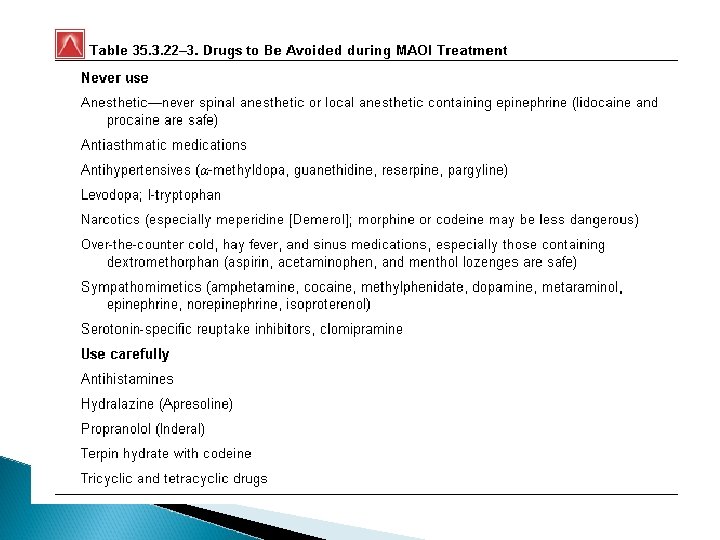
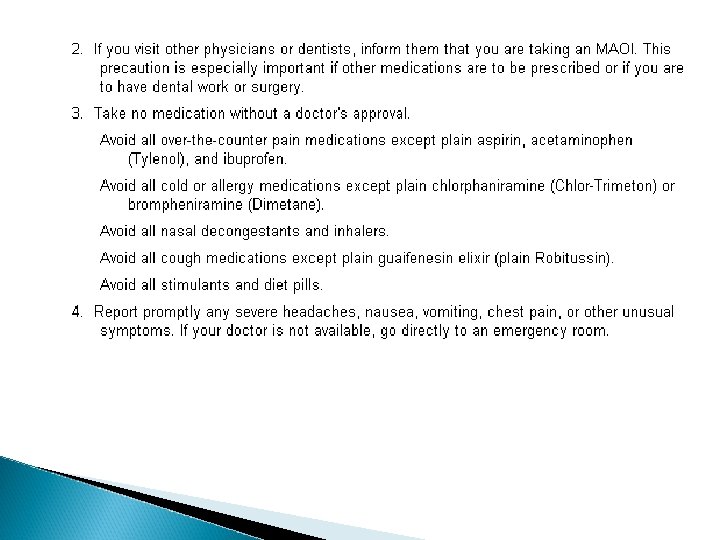
Limitations of MAO inhibitors � Alters the metabolism of amino acid tyramine

Limitations of MAO inhibitors � Alters the metabolism of amino acid tyramine ◦ foods high in tyramine include: aged cheeses, wine, smoked fish, yeast products

Limitations of MAO inhibitors � Alters the metabolism of amino acid tyramine ◦ foods high in tyramine include: aged cheeses, wine, smoked fish, yeast products ◦ consumption of these can result in a hypertensive crisis: �severe headaches, heart palpitations. Flushing, nausea, vomiting, stroke

Limitations of MAO inhibitors � Alters the metabolism of amino acid tyramine ◦ foods high in tyramine include: aged cheeses, wine, smoked fish, yeast products ◦ consumption of these can result in a hypertensive crisis: �severe headaches, heart palpitations. Flushing, nausea, vomiting, stroke ◦ very long 1/2 life (2 weeks)

2 nd generation antidepressants � from late 1970’s - mid 1980’s- looked for agents that could overcome some of the – of TCA ◦ slow onset, limited efficacy, side effect profile, etc � amoxapine (Asendin) � Trazodone (Desyrel) ◦ primarily SNRI (but also blocks DA) ◦ doesn’t block NE or 5 HT �less anti ACh; quicker action? � 5 HT agonist… (5 HT 2)
 ◦ antidepressant, anticraving (for nicotine dependence) ◦ antidepressant effect much")
� Buproprion (Wellbutrin, Zyban) ◦ antidepressant, anticraving (for nicotine dependence) ◦ antidepressant effect much like the SSRIs but with less nausea, diarrhea, somnolence and sexual dysfunction ◦ selectively inhibits DA, NE reuptake
 - first introduced in US in 1988 � SSRIs have")
SSRIs � Fluoxetine (Prozac) - first introduced in US in 1988 � SSRIs have a more favorable side effect profile than earlier antidepressants � relatively safe (esp in OD situations) � some controversy…. . .
 paroxetine (Paxil) sertraline (Zoloft) fluvoxamine")
SSRIs � 6 ◦ ◦ ◦ SSRIs fluoxetine (Prozac) paroxetine (Paxil) sertraline (Zoloft) fluvoxamine (Luvox) citalopram (Celexa) escitalopram (Lexapro)

How do SSRIs work? � Block reuptake of 5 HT ◦ selective serotonin reuptake inhibitor � single action antidepressant

5 HT withdrawal syndrome � occurs in ~ 60% of people who discontinue experience withdrawal � onset usually within a few days and persists for 3 – 4 weeks (fluoxetine even longer due to its ½ life)
 distress � Flulike symptoms")
Symptoms of withdrawal � disequilibriam � GI (dizziness, vertigo, ataxia) distress � Flulike symptoms (fatigue, lethargy, chills) � sensory disturbances � sleep disturbances

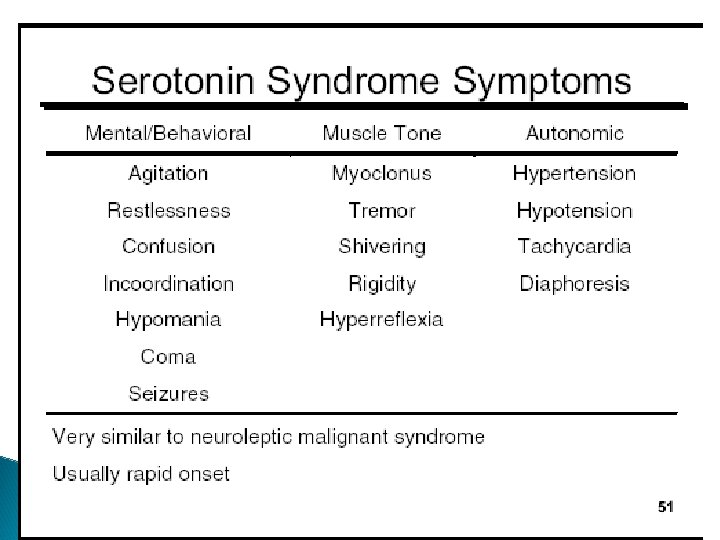
5 HT syndrome � most often seen when individual takes 2 or more drugs that increase 5 HT activity ◦ ex. SSRIs, MAOIs, TCA � incidence – rare � more than 80% resolve � no specific criterion for diagnosis � can be mild or potentially lethal

dual action antidepressants � may be more effective at treating somatic symptoms associated with depression �ex. pain � older � new tca with dual actions antidepressants with dual actions
 – ◦ strongest pharmacological action is 5")
Examples of dual-action antidepressants � Nefazodone (Serzone) – ◦ strongest pharmacological action is 5 HT 2 blockade ◦ also inhibits reuptake of NE and 5 HT ◦ black box warning – liver failure

Star*D study � sequenced depression treatment alternatives to relieve

Current problems that still exist with pharmacotherapy of depression � Some patients do not respond well to first treatment � most take 3 - 4 weeks to exert significant therapeutic effects

Some current issues

Bipolar disorder � Incidence ~ 1% ◦ population-based epidemiologic studies found agecorrected lifetime risks ranging from 0. 3 percent to 1. 5 percent, with = risks to men and women in 10 countries as divergent as Lebanon and Korea. � Less favorable profile than for depressive disorders � Most come to the attention of docs � Age of onset – ◦ Wide range with average ~ 30

�Bipolar disorder patients have a relatively high rate of nonadherence to pharmacotherapy, estimated at 32– 45% of treated patients (Rothbaum & Astin, 2000). �Approximately 25 -50% of individuals with bipolar attempt suicide, and 11% actually commit suicide.

Heritability of Bipolar I �~ 50 percent bipolar I disorder patients have at least one parent with a mood disorder, most often major depressive disorder. ◦ mode of inheritance - complex and likely involves multiple interacting genes. � If one parent has bipolar I disorder, 25 percent chance that a mood disorder; � if both parents have bipolar I disorder, there is a 50 to 75 percent chance that their child has a mood disorder.

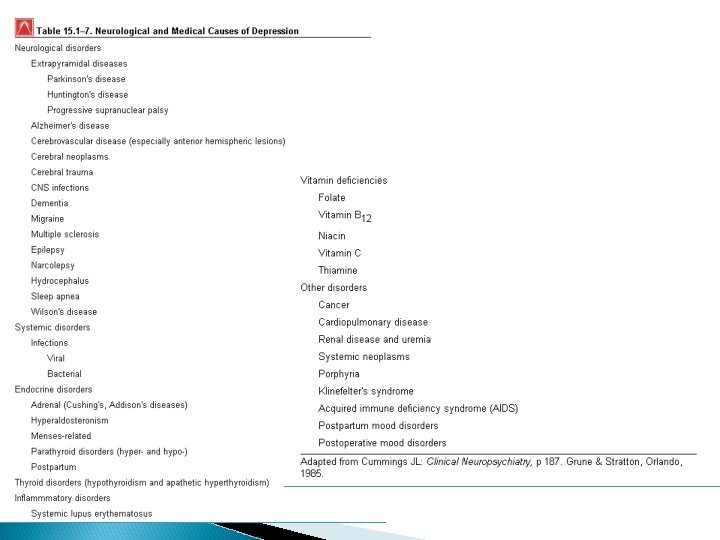
Encephalitis lethargica

drugs that can produce manic states � amphetamine � cocaine � corticosteroids � hallucinogens � l-dopa � pcp � methylphenidate

What is the aim for drugs for treating bipolar � stabilize acute mania, mixed and depressive symptoms � don’t induce mood alterations � prevent future relapses

Pharmacotherapy for Bipolar � Until the last 10 – 15 years – lithium only approved drug for treating bipolar � now number of drugs referred to as “Mood stabilizers”

Treatments for Bipolar � Lithium � Anticonvulsants � Atypical antipsychotics
 ◦ Metal isolated in 1818 ◦ Introduced")
Lithium History � Lithium (Duralith, Eskalith, Lithobid) ◦ Metal isolated in 1818 ◦ Introduced into medicine in 1840 for txt of bladder stones and gout ◦ lithium bromide - 1873 - used to treat manic episodes althought was that bromide was active ingredient ◦ 1886 - prophylactic and short term effects of lithium for txt depression ◦ Late 1880's - early 1900's - general public so enthusiastic endorsing taking of waters

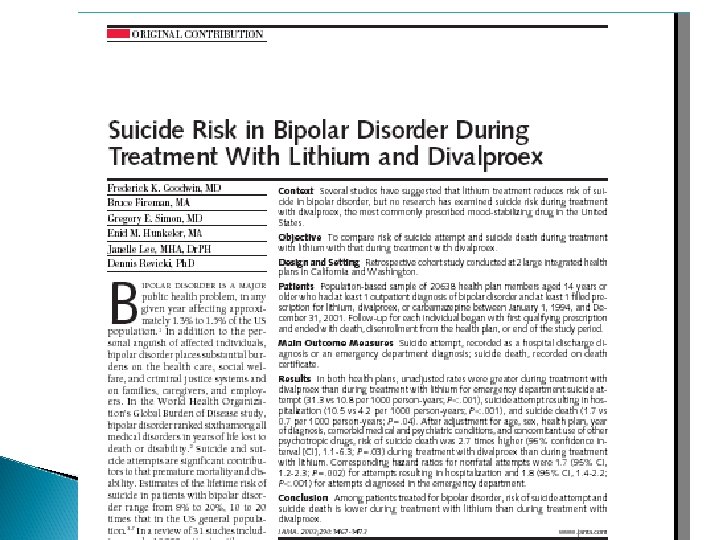
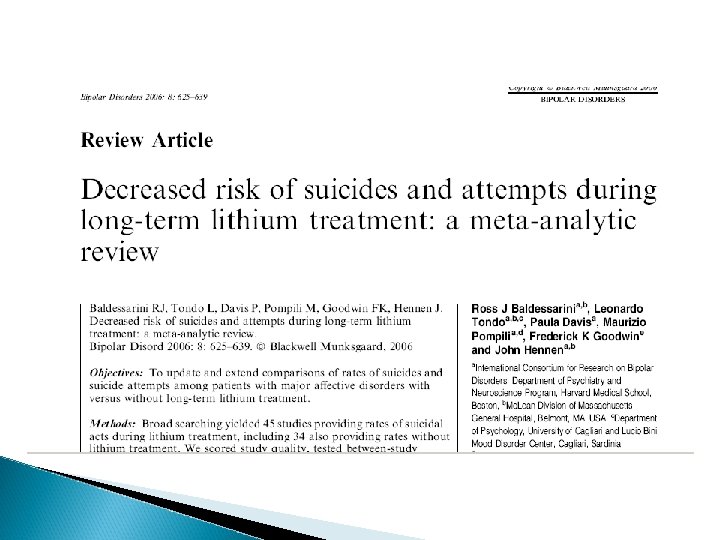
1940's - lithium chloride used as replacement for Na. Cl ◦ 1949 - lithium caused lethargy when injected in animals ◦ 1950's - 1960's - did FDA trials demonstrating short-term prophylactic efficacy of lithium for bipolar 1 disorder ◦ 1970's - reintroduced to treat mania ◦ ◦ 2003 - Evidence suggests that lithium, unlike any other mood stabilizer, may have a specific antisuicide effect

Lithium �pharmacokinetics ◦ kidneys excrete 95% ◦ sweat – 4 -5% �pharmacodynamics: ◦ good question!!!!! ◦ modulation of the levels of several genes maybe?

� ethnic differences – ◦ AA with similar plasma levels as Caucasians had on average 60% higher intracellular levels �many AA respond better with lower plasma Li levels and lower side effects � does not produce dependence or withdrawal � Frequency of bipolar relapses in 2 years ◦ In 20 – 40% of patients on lithium ◦ In 65 – 90% of patients without lithium � Suicidal attempts rose 22 -fold, and fatalities increased 14 -fold, within the first year after discontinuing the lithium.

Side effect profile for Li � Side Effects: ◦ Gastric distress: nausea, decreased appetite, vomiting, diarrhea ◦ Weight gain - poorly understood effect of lithium on carbohydrate metabolism �(in long-term therapy ~ 30% become obese); ◦ tremor - recognized in 4 th edition of DSM IV usually noticed in hands and fingers ◦ cognitive effects , - dysphoria, lack of spontaneity, slowed reaction times, impaired memory ◦ potential teratogenicity

◦ renal: polyuria with 2 ndary polydipsia - urinary output can be up to 3 liters/day (for most of us it is 1 - 2) due to antagonism of ADH; Most serious renal adverse effects - renal failure ◦ thyroid effects - causes generally benign and often transient dimunition in concentrations of circulating thyroid hormones ◦ cardiac - can result in sinus dysrhythmias ◦ dermatological effects - various kinds of acne, possible worsening of psoriasis ; risk of tetracycline; alopecia◦ lithium toxicity and overdose �antipsychotics – TI ~ 100; TCAs/MAOI TI ~ 10 Lithium ~ 3

What are the signs of lithium toxicity? � Doses are adjusted to achieve plasma concentrations of 0. 6 to 1. 2 m. M Li (lower end of the range for maintenance therapy and elderly patients) on samples taken 12 hours after the preceding dose. � Overdosage - usually with plasma concentrations over 1. 5 to 1. 8 m. M Li – ◦ keep in mind individual differences � Symptoms: Shaking and trembling, confusion, slurred speech, nausea and vomiting, diarrhea, abdominal pain, unsteadiness on the feet, coma, seizures

� At plasma levels of 1. 5 to 2. 0 m. Eq/l - most reactions involve GI tract with nausea, vomiting, diarrhea and abdominal pain ◦ Neurological side effects commonly seen at this dose include slight tremor, lethargy, impaired concentration, dizziness, slurred speech, ataxia, muscle weakness and nystagmus � once get above 2. 0 m. Eq/l - more severe side effects; � above 2. 5 m. Eq/l - can cause stupor, coma, renal failure, cardiac arrythmias and death

Treatment for Li toxicity � no antidote to lithium; usually add sodium containing fluids immediately; if toxic signs are severe, may use hemodialysis, gastric lavage, diuretic, antiepileptic, etc

maintainance therapy �- although li prevents manic and depressive episodes < 50% achieve complete relief � Recommendations: ◦ maintain bipolar patient on Li for 9 – 12 months after manic episode

anticonvulsants � introduced in 1990’s to treat bipolar � possible mechanism? � Kindling - electrophysiological process in which repeated sub-threshold stimulation of a neuron eventually generates an action potential �kindling in temporal lobes? ◦ carbamazepine reduces kindling (in animal models)

anticonvulsants that have been used or are being considered to treat bipolar � carbamazepine (Tegretol), divalproex (Depakote), gabapentin (Neurontin) and lamotrigine (Lamictal), valproic acid (Depakene)
 – approved in 1995 ◦ also reduces kindling, has anticonvulsant effects and")
�valproate (Depakote®) – approved in 1995 ◦ also reduces kindling, has anticonvulsant effects and GABAergic effects �Most serious side - liver toxicity and failure ◦ Persons taking more than one type of anticonvulsant seem to be at higher risk. �Most common side effects with valproic acid therapy are nausea, vomiting and indigestion; abdominal pain, constipation or diarrhea �Both loss of appetite with weight loss and appetite stimulation with weight gain have been reported.
 ◦ altered effectiveness of birth control pills ◦ rarer side")
carbemazepine � carbamazepine (Tegretol®) ◦ altered effectiveness of birth control pills ◦ rarer side effects - clumsiness, double vision, edema (excess of fluid in tissue or body cavity), skin rash, and cardiovascular complications.

carbemazepine’s onset of action ◦ < 1 day: seizures ◦ 6 – 12 days; mania ◦ > 30 days aggression not caused by mania � full effect ◦ within hours for epilepsy ◦ 2 weeks for mania ◦ 2 – 3 weeks for depression
, cimetidine (heartburn), erythromycin")
Potential interactions for carbemazepine grapefruit juice, influenza vaccine, isoniazid (treats tb), cimetidine (heartburn), erythromycin (antibiotics), and phenelzine (MAOI) increase plasma levels Phenytoin (anticonvulsant), alprazolam, clonazepam, primidone (anticonvulsant), and phenobarbital decrease both CBZ level and levels of interacting agents; fluoxetine increases levels decreases levels of imipramine, phenothiazines, haloperidol, theophylline, thyroid hormones, ritonavir, saquinavir, contraceptives, risperidone, thiothixene, cyclosporine, corticosteroids, doxycycline, trazodone, doxepin, and amitriptyline can reduce its own level by "autoinduction; " coadministration with lithium increases toxicity of both CBZ and the interacting agents; coadministration with clozapine further increases bone marrow toxicity and resulting agranulocytosis
 – more antidepressant than antimanic � clozapine – may")
Atypical antipsychotics � risperidone (Risperdal) – more antidepressant than antimanic � clozapine – may be more antimanic than antidepressant � olanzapine (Zyprexa) – useful for both acute mania and (now available in combination with fluoxetine) as Symbyax � quetiapine (Seroquel) � ziprasidone (Geodon) � aripiprazole (Abilify)
- Slides: 71