Advanced Lipid Testing Case Based Approach Tara Dall

Advanced Lipid Testing Case Based Approach Tara Dall, MD Advanced Lipidology Delafield, Wisconsin Diplomate, American Board of Clinical Lipidology www. advlip. com

Disclosures F Speakers bureau Abbott, Liposcience, GSK Off label: discussion of off label use of approved pharmacologic therapy may be discussed

What has been your use of NMR Lipoprofile? 1. 2. 3. 4. Have ordered a few <10 Routinely use as part of my practice Use other Advanced testing labs Never ordered NMR
 are the causal agents in")
LDL Particles Cause Atherosclerosis Low Density Lipoprotein particles (LDL) are the causal agents in atherosclerosis. 1 The more lipoprotein particles a person has, the higher the risk for plaque buildup that causes heart attacks, regardless of how much cholesterol those particles carry. 1 Fredrickson et al. NEJM 1967; 276: 148

So Why Is LDL So Important in CVD? Gradient driven process…LDL Particles invade the arterial wall ÌOxidative Ì Foam Modification Cell Formation Ì Atherosclerosis The higher the number of LDL particles (LDL-P), the greater the risk for CHD. 2 Fredrickson et al. NEJM 1967; 276: 148
 This")
LDL Cholesterol Is Not LDL!! Apo B This is an LDL particle (LDL-P) This is LDL Cholesterol (LDL-C) POLAR SURFACE COAT Phospholipid Free cholesterol NONPOLAR LIPID CORE Cholesterol Ester Triglyceride A convenient analytic surrogate of LDL since 1972
 0. 95 IDL 1. 006 1. 02 1. 06 1.")
Lipoprotein Subclasses Density (g/ml) 0. 95 IDL 1. 006 1. 02 1. 06 1. 10 Chylomicrons VLDL Chylomicron Remnants LDL HDL 2 Lp(a) HDL 3 Apo B = non HDL-C 1. 20 5 10 20 40 60 Diameter (nm) 80 1000

Small LDL Particles Contain Less Cholesterol Than Large LDL Particles Up to 70% More Particles 100 mg/d. L Large LDL Small LDL Cholesterol Balance

Even LDL Particles of the Same Size can Differ in Cholesterol Content Up to 40% More Particles 100 mg/d. L Normal Cholesterol Per Particle Less Cholesterol Per Particle Cholesterol Balance

Weight of Evidence Over 180 NMR related papers published to Date

Disease States where LDL-Particle and LDL-Cholesterol are most likely to Differ and NMR testing should be considered F Known Coronary Heart Disease F Metabolic Syndrome F Diabetes F Family history premature heart disease F High Triglyceride and low HDL

Relations of LDL Particles and LDL Cholesterol to Levels of HDL Cholesterol and Triglycerides Otvos et al. , Amer J Cardiol 2002; 90: 22 i-29 i.

LDL Cholesterol and LDL Particle Numbers in Type 2 Diabetes Patients with LDL-C < 100 mg/d. L (n=2, 355) 5 th 37% (n=870) 20 th 50 th 80 th percentile 63% (n=1485) LDL-C Percent of Subjects 70 7% (n=162) 100 31% (n=741) 130 38% (n=891) Percent 160 (mg/d. L) 16% (n=383) 8% (n=178) 24% of LDL-P Subjects 700 1000 1300 1600 (nmol/L) Am J Cardiol. 2006; 98: 1599 -1602
 20 th 24%")
LDL Particle Number Distribution in Diabetes Subjects 5 th 1% (n=19) 20 th 24% (n=364) 50 th 43% (n=631) 80 th 21% (n=307) percentile 11% (n=163) 32% Percent LDL-C 71 -99 mg/d. L of Subjects (n=1, 484) 700 16% (n=147) 1000 1300 43% (n=377) 30% (n=260) 1600 (nmol/L) 9% (n=76) 2% (n=15) 41% Percent of LDL-C < 70 mg/d. L Subjects (n=871) 700 1000 1300 1600 (nmol/L) Am J Cardiol. 2006; 98: 1599 -1602

Framingham Heart Study Offspring Cohort 1. 00 0. 98 0. 96 Low LDL-C n=1249 Probability of Event Free Survival 0. 94 Event-free survival among participants with low-density lipoprotein cholesterol (LDL-C)above or below the median. 0. 92 0. 90 0. 88 0. 86 Median values were 131 mg/d. L for LDL-C High LDL-C n=1251 0. 84 0. 82 How predictive is LDLC with respect to event -free survival? 0. 80 0. 78 0. 76 0. 74 0 2 4 6 8 10 12 14 16 Years of Follow-up Cromwell W et al. J Clin. Lipidol 2007; 1: 583 -592

Framingham Heart Study Offspring Cohort 1. 00 0. 98 0. 96 Event-free survival among participants with low-density lipoprotein cholesterol (LDLC)above or below the median. Probability of Event Free Survival 0. 94 0. 92 High LDL-C n=284 0. 90 0. 88 Median values were 131 mg/d. L for LDL-C 0. 86 0. 84 0. 82 Low LDL-C n=282 0. 80 Additional Data 0. 78 0. 76 0. 74 0 2 4 6 8 10 12 14 16 Years of Follow-up Cromwell W et al. J Clin. Lipidol 2007; 1: 583 -592

Framingham Heart Study Offspring Cohort 1. 00 0. 98 Low LDL-P 0. 96 Low LDL-C n=1249 0. 94 Probability of Event Free Survival Event-free survival among participants with low-density lipoprotein cholesterol (LDL-C) and LDL particle number (LDL-P) above or below the median. Low LDL-P 0. 92 Median values were 131 mg/d. L for LDL-C and 1414 nmol/L for LDL-P. High LDL-C n=284 0. 90 0. 88 0. 86 Significant # of LDL-C / CV-risk disconnects High LDL-P was strongly associated with increased CVD risk in both men and women (p<0. 0001) High LDL-C n=1251 0. 84 High LDL-P 0. 82 Low LDL-C n=282 When data for men and women were combined, ? Explanation Particle number (LDL-P) 0. 80 0. 78 0. 76 LDL-P was approximately twice as strongly related to CVD incidence as LDL-C is the key risk factor 0. 74 0 2 4 6 8 10 12 14 16 Years of Follow-up Cromwell W et al. J Clin. Lipidol 2007; 1: 583 -592

Cumulative Incidence of CVD Events in MESA in Subgroups with Low LDL-C, Low LDL-P, or Both From proportional hazards regression analyses adjusted for age, sex, race, SBP, smoking, hypertension rx, BMI, and diabetes. J Clin Lipidology 2011

Small, Dense LDL Published studies confirm there is no association of LDL size with CHD events independent of LDL-P: VA-HITCirculation 2006; 113: 1556 -63 EPIC-Norfolk. JACC 2007; 49: 547 -53

Small LDL-P Conclusions • NMR data confirm that patients with predominantly small LDL particles have higher CHD risk. • These patients also have LDL-P > LDL-C discordance. • Independent of LDL-P, there is no excess risk associated with small LDL size.
")
Carotid Atherosclerosis in MESA (adjusted for age, sex, race, smoking, diabetes, TG, and HDLc) Carotid IMT (microns) Quartile 1: LDLc <100 mg/d. L (n=1, 425) n=32 Ptrend = 0. 006 n=352 n=153 n=888 Q 1 Q 2 Q 3 Q 4 LDL Particle Number Mora et al, AHA/ADA Metabolic Syndrome meeting, May 2006

ADA and ACC Consensus Statement on Lipoprotein Management in Patients with Cardiometabolic Risk TREATMENT GOALS Highest-risk patients, including those with 1) known CVD or 2) Diabetes plus one or more additional CVD risk factor LDL-C Non-HDL-C Apo. B (mg/d. L) < 70 High-risk patients, including those with 1) no diabetes or < 100 known clinical CVD but 2 or more additional major CVD risk factors or 2) Diabetes but no other CVD risk factors < 100 < 130 < 80 < 90 Brunzell JD, Davidson M, Furberg CD et al. Diabetes Care 2008; 31: 811 -822

Clinical Cutpoints for LDL Percentile: 20 th 50 th 80 th Optimal High LDL Cholesterol Framingham Offspring 70 MESA 100 130 160 190 220 250 mg/d. L LDL Particle Number 700 1000 1300 1600 1900 Percent of Subjects 2200 2500 nmol/L

Recommendations from AACC Lipoproteins and Vascular Diseases Division Working Group on Best Practices Suggested Treatment Goals Apo. B LDL-C Non-HDL-C mg/d. L < 70 < 80 < 100 < 80 < 120 < 100 < 130 < 150 LDL-P nmol/L < 1100 < 1400 Contois. JH, et al. Clinical Chemistry 2009; 55: 407 -419
")
Population Equivalent Cutpoints for Alternate LDL Measures (LDL-C, Measured Apo B and NMR LDL-P) Biomarker Population LDL-C (mg/d. L) Measured Apo B (mg/d. L) Percentile Equivalent Concentration < 5 th 20 th 50 th 80 th Framingham 1 < 70 100 130 160 Framingham 1 < 60 80 100 120 Framingham 1 < 850 1100 1400 1800 MESA 2 < 700 1000 1300 1600 NMR LDL-P (nmol/L) 1 2 Contois, et al. Clinical Chemistry 2009; 55: 407 -419 Cromwell WC. Clinical Challenges in Lipid Disorders. Oxford: Clinical Publishing, 2008: 249 -259.

Treatments that Alter the Cholesterol Content of LDL Change LDLc and LDLp Differentially Cholesterol per particle decreases with: Cholesterol per particle increases with: • statins • fibrates • statin + ezetimibe • niacin • estrogen replacement therapy • glitazones • low fat, high carb diet • omega 3 FAs • exercise • low carb diet LDLc More LDLp More
![Treatment Considerations Combination therapy (statin + other agent[s]) may be necessary to achieve both](http://slidetodoc.com/presentation_image_h2/a59cbfaf1756c4b4e55d408f5b36a282/image-27.jpg "Treatment Considerations Combination therapy (statin + other agent[s]) may be necessary to achieve both")
Treatment Considerations Combination therapy (statin + other agent[s]) may be necessary to achieve both goals. Combination agents which increase LDL size (niacin or fibrates) generally lower LDL-P more than LDL-C.

Beyond LDL: Combination Therapy Statin 0 WOSCOPS 4 S vs CARE Statin/Niacin HPS FATS 10 YR HATS -10 -24 Percent -30 -40 -31 -25 -34 -50 -60 -70 -80 -95 -100 Reduction in CV Events Brown BG, et al. N Engl J Med. 2001; 345: 1583 -1592. -90

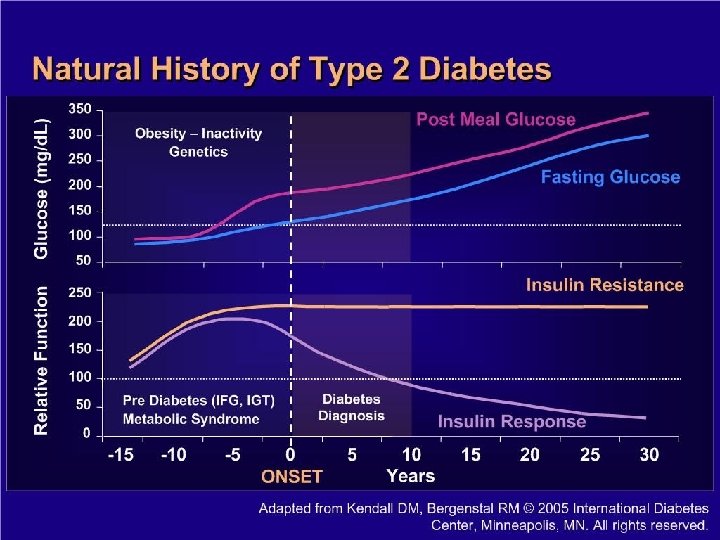
New NMR Report provides Information Regarding Insulin Resistance Possibly years before Diabetes diagnosis Presents with abnormal Glucose

Case Studies

Particle Size may not provide independent prediction of CV risk however…. . Size is helpful however in determining treatment approach
 freq associated with Insulin")
Particle size F Small Dense LDL particles (Pattern B ) freq associated with Insulin resistance, diabetes, metabolic syndrome F Large Bouyant LDL particles (Pattern A) associated with Familial Hypercholesterolemia F Bottom line: too many LDL particles puts patient at risk regardless of whether they are large or small

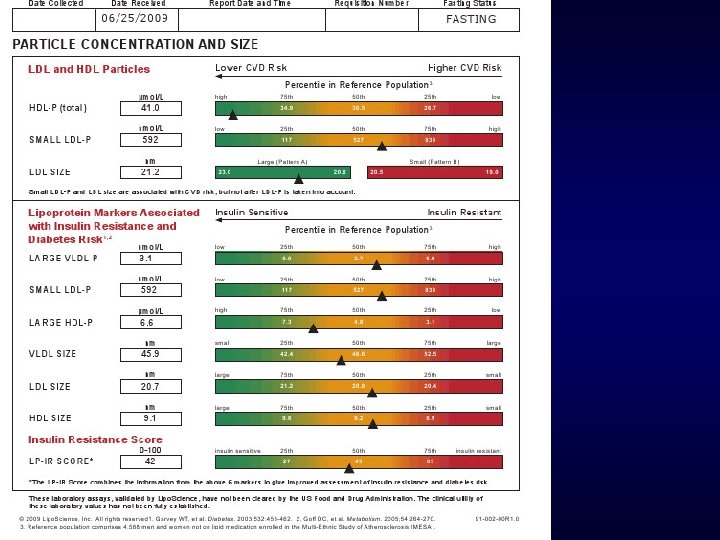
ML 38 yr Obesity, Fam History Premature CAD

ML 38 yr old Male initial visit F Vitals: 3/18/2009 F Wt 396. 6 lb, Ht 73 in, BMI 52 F WC 64 inches F BP 146/88 pulse 84 reg F Hg. AIC 5. 8 F Glucose 119 fasting

ML 38 yr Male F PMH: hypertension untreated, IFG F Medications: none F Fam. Hx: Premature Heart Disease mgma age 64 deceased, M grandfather age 54 MI, Paternal granmother age 60 MI, Mom, Maternal grandfather, Paternal Grandmother diabetes F SH: married nonsmoker (quit 2001), no alcohol, no regular exercise, American diet
 LDL –C 112 Non HDL-C 137 Low HDL 34")
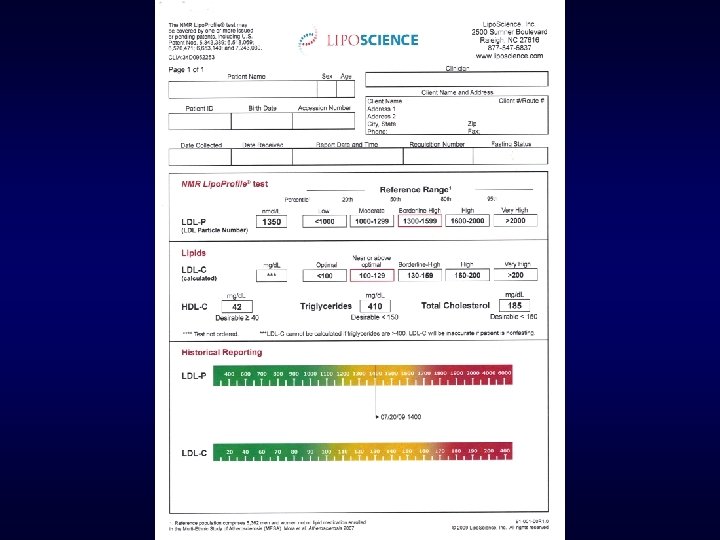
LDL -P 1906 (optimal <1000) LDL –C 112 Non HDL-C 137 Low HDL 34 Triglyceride 124
 Also")
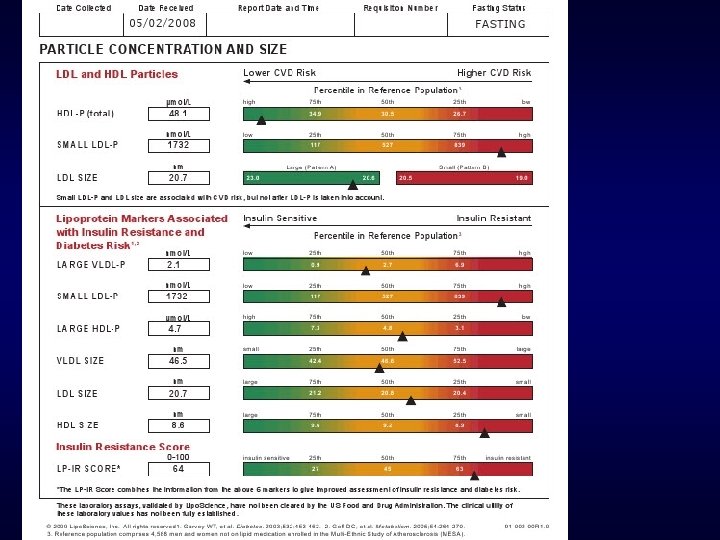
Total LDL P 1906 Small LDL P 1444 IR score 79 (abnormal >45) Also 4/5 metabolic syndrome criteria met

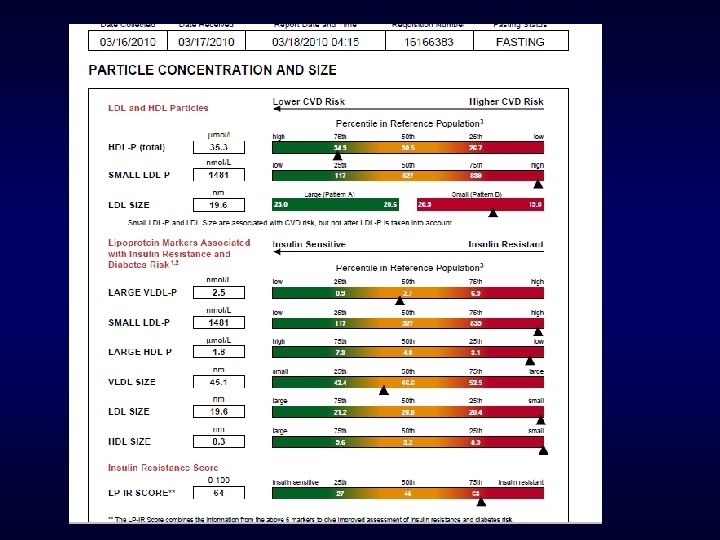
What therapy? LDL P dropped 750 points Non HDL C dropped to 90 from 137

BP 120/80, Hg. AIC 5. 2 Glucose 68 IR SCORE dropped From 79 to 38


5 months later 133 lb weight loss

March 2010 Weight loss maintained. March 2009

45 yr Female Dyslipidemia Excellent Diet and Exercises Daily

45 yr Female Dyslipidemia F Excellent diet and exercises daily F Maximized TLC and dyslipidemia persists

45 yr Female Dyslipidemia F Lipids • Total Cholesterol • LDL-C • HDL-C • Triglycerides Fasting Glucose F BP F BMI F Treatment options? F 250 150 56 220 120/82 25

AHA Guidelines for CVD Prevention in Women Clinical Recommendations Major Risk Factor Interventions F Lipids - Lipoproteins: • Optimal levels of lipids and lipoproteins in women: • LDL-C < 100 mg/d. L • Triglycerides < 150 mg/d. L • HDL-C > 50 mg/d. L • Non HDL-C < 130 mg/d. L Mosca, L. et al. Circulation 2004; 109: 672 -693

AHA Women’s Guidelines for Lipid Management n Initiate TLC for all women, regardless of risk level – – – Intermediate Risk Initiate statin if LDL-C ≥ 130 mg/d. L on TLC Initiate niacin or fibrate for low HDL-C, after LDL-C goal is reached Initiate niacin or fibrate for high non–HDL-C, after LDL-C goal is reached – – – High Risk Initiate statin if LDL-C ≥ 100 mg/d. L concomitant with TLC Initiate niacin or fibrate for low HDL-C Initiate niacin or fibrate for high non–HDL-C Mosca L, et al. Circulation. 2004; 109: 672 -693.

LDL-P 2552 Small LDL-P 1882 Treatment options: Lifestyle Statin Niaspan Fibrate Combination Metformin TZD Others
 brought LDL-P down 1068 points?")
2 Months later What treatment (s) brought LDL-P down 1068 points?
 brought LDL-P down 1068 points? 1. Statin monotherapy 2. Combo therapy")
What treatment (s) brought LDL-P down 1068 points? 1. Statin monotherapy 2. Combo therapy with statin plus 3. Niacin 4. Fibrate 5. Metformin
 brought LDL-P down 1068 points? 5 pound weight")
2 Months later What treatment (s) brought LDL-P down 1068 points? 5 pound weight loss & Metformin ER 1000 mg/day

H. L 68 yr WM prior Stroke F BP: 130/85 F PMH: CVA (Stroke = cardiac risk equivalent) • No lipid meds • LDL cholesterol at goal 70

H. L. NMR lipoprofile no meds F F F F F LDL particle 1879 (optimal <700 -1000) Small LDL p 1870 LDL cholesterol 70 HDL 36 Triglyceride 273 Total chol 161 LDL particle size Pattern B Large HDL p 4. 1 intermediate risk Large VLDL p 10. 4 High risk TSH, CMP normal

Follow up NMR 1 month later Simvastatin 40 mg Omega 3 fish oil 4 grams LDL particle was 1879 now 1115 LDL cholesterol was 70 now 53 Hg. AIC 5. 9

What treatment do you advise now along with Diet and Exercise? F 1. no further treatment F 2. Increase Simvastatin to 80 F 3. Add Metformin F 4. Add Fibrate F 5. Add Niacin

2 New Patient referrals Secondary Prevention 3/16/2010 F Both patients recent Myocardial Infarction referred for lipid treatment and work up genetic etiology F Both patients on Moderate dose stain at time NMR drawn

Consult #1 Secondary Prevention on statin LDL cholesterol 57 At NCEP goal LDL Particle very High risk 1835 (Optimal <700) Discordance Additional Therapy needed

Consult #2 Secondary Prevention on statin LDL cholesterol 60 at NCEP Goal LDL Particle Concentration 1006 Also at Goal No further treatment needed

Same Day 2 Consults Completely different decision making based on NMR results

Comparison of 2 43 year old white females Both high HDL, no Family History Heart Disease

What does the lipid panel tell us about these women’s risk for heart disease? F C. H. 43 yrs F D. L. 43 yrs F Lipid panel F Lipid Panel F Total chol 251 F Total chol 232 • LDL 130 • HDL 88 • HDL 82 • Trig 166 • Trig 101 • Tchol/HDL 2. 9 • Tchol/HDL 2. 8 • Non HDL 163 • Non HDL 150 • Framingham 2. 2% • Framingham 2. 1%

2 very different LDL particle concentrations F C. H. NMR High Risk F D. L NMR Low Risk

LDL C goal <100, LDL P goal <1000 LDL C goal <100 Requires 22% reduction Alternative measure of LDL : LDL Particle goal <1000 requires 64% Reduction of LDL P to get to goal

Office visits two women same day Primary prevention Lets assess their cardiovascular risk

2 women One Day in May F BK F 45 yr old BMI 29, 120/72 Total chol 154 F LDL c 71 F HDL c 70 F Triglyceride 64 F LDL particle size B F LDL particle # F • LDL p 1042 F JS F 41 yr old BMI 29, BP 122/78 Total chol 165 F LDL c 74 F HDL c 71 F Triglyceride 98 F LDL particle size B F LDL particle # F • LDL p 2102

BK 45 yr WF JS 41 yr WF

JS age 41 Does not meet criteria for Metabolic syndrome Normal Triglyceride, normal HDL Normal BP 122/78 Has increased waist circumference 36 inches 1/5 clinical criteria NMR shows markers of metabolic syndrome 2007 Hg. AIC 5. 4 2008 fasting glucose 107

Conclusions: LDL Particle/Apo B for Risk Assessment Primary Prevention: risk stratify more accurately, target therapy appropriately Avoid overtreatment of high LDL –C when LDL P optimal Pediatric patients : better assess who should be treated more aggressively with statins

Risk Management Patient Compliance with therapy: Bigger numbers instill more fear Identify Metabolic syndrome/Insulin resistance before traditional tests become abnormal Its our “window into Diabetes” Target therapy based on whether Metabolic markers present or not

Risk Management Clinical Pearl Combination drug therapy fixes LDL Particle elevations more then high dose statinmonotherapy

Questions F www. advlip. com F Taradall@advlip. com
- Slides: 78