Advanced Endoscopy Techniques Jayant P Talreja M D






 –")









 0.")






, particularly in esophageal CA •")


- Slides: 30
Advanced Endoscopy Techniques Jayant P. Talreja, M. D. Gastrointestinal Specialists, Inc. Bon Secours St. Mary’s Hospital
Acknowledgements Christopher Thompson, MD Marvin Ryou, MD William Brugge, MD David Forcione, MD Brigham & Women’s Hospital Massachusetts General Hospital Harvard Medical School Boston, MA
Objectives • Discuss the endoscopic management of Barrett’s Esophagus • EUS-guided placement of fiducials • Endoscopic management of bariatric surgery complications
Case Presentation #1 HPI: • 53 year old male with 8 month history of reflux symptoms • Marginal benefit with omeprazole daily • Despite lifestyle modifications – avoiding dietary triggers, late meals • No alarm symptoms – no dysphagia, weight loss • Presented for outpatient EGD
Barrett’s esophagus • In 1957 Norman Barrett, British thoracic surgeon, described the “lower esophagus lined by columnar epithelium. ” • Barrett’s esophagus is now defined as “metaplastic change from squamous to columnar-lined epithelium (including the presence of goblet cells), visible endoscopically and confirmed histologically. ” • Barrett’s esophagus results from the reflux of gastric acid and bile salts into the esophagus, and may be viewed as an adaptive response in which stratified squamous epithelium is replaced by potentially acid-resistant columnar epithelium. O’Donovan M, Fitzgerald R. Diag Histopath 2012 Noffsinger N. Atlas Nontumor Path. AFIP. 2007
Evolution of Barrett’s and Cancer Injury Acid & bile reflux nitrous oxide Genetics Gender, race, ? other factors (cox-2) Accumulate Genetic Changes Kountourakis P, et al. Gastrointest Cancer Res 2012 Ong CA, et al. World J Gastroenterol, 2010
Barrett’s Prevalence Estimates • 1. 6% of general adult population (3. 8 M) – Ronkainen J, et al. Prevalence of BE… Gastroenterology 2005; 129: 1825 -31. • 5. 6% of general US adult population (13. 1 M) – Hayeck TJ, et al. The Prevalence of BE in the US (model)…Dis Esophagus 2010; 23: 451 -7. • 6. 8% of persons over age 40 (8. 3 M) – Rex DK, et al. Screening for Barrett’s. . . Gastroenterology 2003; 125: 1670 -77.
U. S. Cancer Incidence General Population Cancer Incidence Esophageal 3. 0 per 100, 000 Adenocarcinoma (0. 003%) Colorectal Cancer HGD Cohort Cancer Incidence Multiple 6, 600 per 100, 000 (6. 6%) 2, 200 X General Population Polyp Cohort Cancer Incidence Multiple 45 per 100, 000 (0. 045%) 13 X http: //www. seer. cancer. gov/ (accessed July 2, 2013) Surveillance, Epidemiology and End Results (SEER) Wani S, et al. Am J Gastroenterol 2009 Winawer SJ, et al. N Engl J Med 1993 580 per 100, 000 (0. 58%) Risk multiple for developing cancer conferred by HGD or polyp versus risk of that cancer in the general U. S. population
U. S. Cancer Incidence General Population Cancer Incidence LGD Cohort Cancer Incidence Multiple 1, 700 per 100, 000 (1. 7%) 560 X General Population Cancer Incidence Polyp Cohort Cancer Incidence Multiple 45 per 100, 000 (0. 045%) 580 per 100, 000 (0. 58%) 13 X Esophageal 3. 0 per 100, 000 Adenocarcinoma (0. 003%) Colorectal Cancer http: //www. seer. cancer. gov/ (accessed July 2, 2013) Surveillance, Epidemiology and End Results (SEER) Wani S, et al. Am J Gastroenterol 2009 Winawer SJ, et al. N Engl J Med 1993 Risk multiple for developing cancer conferred by LGD or polyp versus risk of that cancer in the general U. S. population
U. S. Cancer Incidence General Population ND-BE Cohort Cancer Incidence Esophageal Adenocarcinoma 3. 0 per 100, 000 (0. 003%) 330 per 100, 000 (0. 33%) General Population Cancer Incidence Polyp Cohort Cancer Incidence Colorectal Cancer 45 per 100, 000 (0. 045%) http: //www. seer. cancer. gov/ (accessed July 2, 2013) Surveillance, Epidemiology and End Results (SEER) Desai TK, et al. Gut 2012 Winawer SJ, et al. N Engl J Med 1993 580 per 100, 000 (0. 58%) Multiple 110 X Multiple 13 X Risk multiple for developing cancer conferred by NDBE or polyp versus risk of that cancer in the general U. S. population
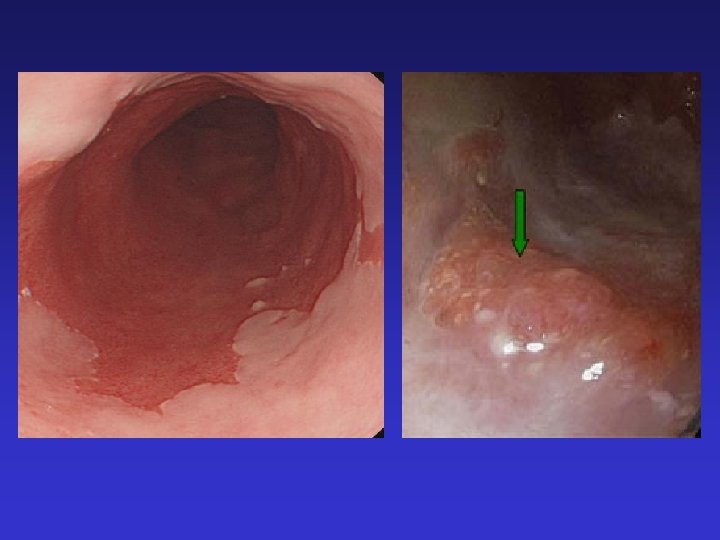
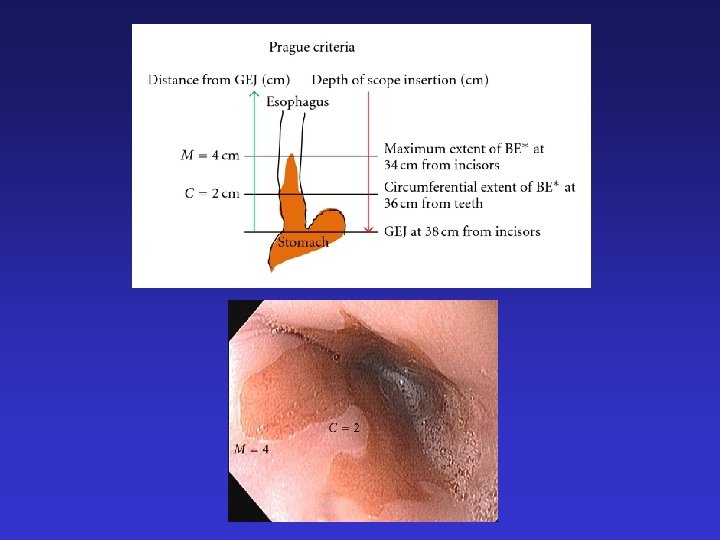
Case Presentation #1 • Diagnostic EGD – by Prague Criteria the Barrett’s appearing mucosa was measured at C 5 M 6 • Top of the gastric folds seen at 40 cm • Circumferential extent of Barrett’s terminated at 35 cm • Maximum extent of Barrett’s terminated at 34 cm • Prague Criteria – C 5 M 6 • Biopsies taken with cold forceps • Current consensus guidelines – 4 quadrant biopsies every 2 cm • Directed biopsies at abnormal appearing regions (i. e. nodules) • This patient had a total of 4 specimen jars – biopsies taken every 2 cm and directed biopsies at nodular region
Case Presentation #1 • Biopsies of nodular region show high grade dysplasia • Remaining biopsies show intestinal metaplasia consistent with Barrett’s esophagus • Follow up discussion with patient about significance of these findings and options for the next step in management • What can we offer this patient? • Endoscopic mucosal resection • Radiofrequency Ablation
Endoscopic Mucosal Resection • endoscopic technique designed to remove targeted superficial tissue • Indicated for nodular dysplasia and superficial T 1 a adenocarcinoma • Distinct advantage is availability of larger tissue specimens • EMR for HGD and EAC is successful in 91 -98% of T 1 a cancers • Complications include bleeding, perforation, and stricture formation
Endoscopic Mucosal Resection
Case Presentation #1 • EMR of nodular region completed during subsequent endoscopy • If initial biopsies had shown intramucosal carcinoma, staging radial EUS would be performed prior to EMR to ensure submucosal preservation • Post-procedure recommendations: – Clear liquid diet for 24 hours – Soft solid diet for 72 hours – PPI – Carafate – Consider liquid oxycodone – Avoid non-essential NSAID’s for 14 days – Hold Plavix for additional 5 -7 days – Restart ASA if CAD – Repeat EGD in 2 months
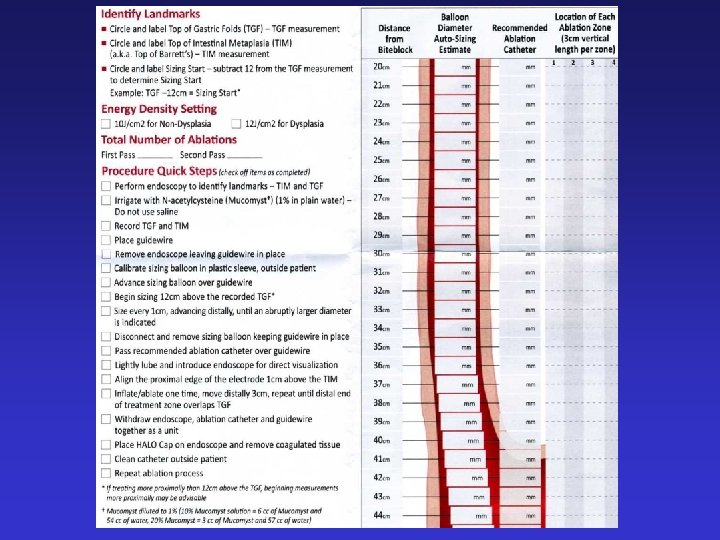
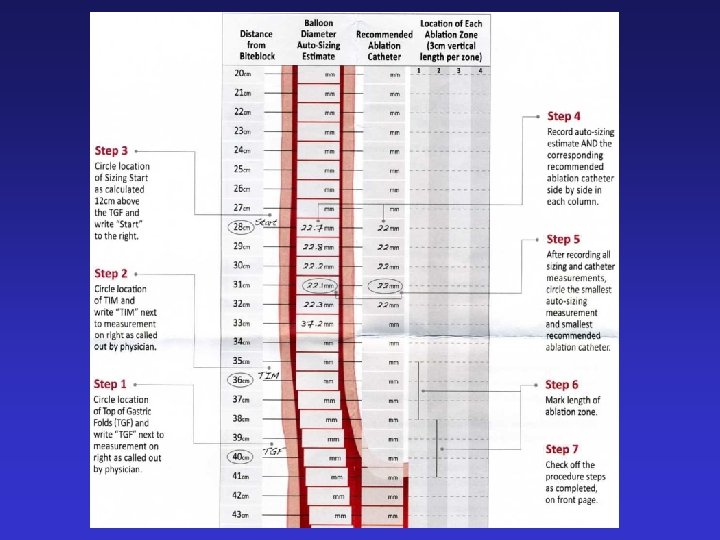
Case Presentation #1 • Repeat EGD in 2 months shows well healed EMR resection site with no residual nodularity • Next step is to proceed to radiofrequency ablation (RFA) • An electrode mounted on a balloon catheter or over the scope is used to deliver heat energy directly to the diseased lining of the esophagus. • The energy delivered results in high temperature heating (ablation) of the Barrett’s lining. • This tissue sloughs off over 48 to 72 hours following the procedure. • Over a period of six to eight weeks, this tissue is replaced by normal (squamous) lining.
Ablation Effect on Natural History NDBE LGD HGD Polyp Natural History (53 studies) 0. 6% 1. 7% 6. 6% 0. 58% After Ablation (65 studies) 0. 16% 1. 7% 0. 06% NNT=45 NNT=13 NNT= 4 NNT= 38 Progression risk expressed as “Per-patient-per-year” (%) risk of developing EAC NNT calculated on 5 -year basis (number needed to treat to avoid one cancer over 5 years) Wani S. Am J Gastro 2009 Winawer SJ. NEJM 1993
Proprietary Properties of RFA Lead to a Precise Ablation Depth Mechanisms 1. Tightly spaced electrodes (250 µm apart) 2. Proven pre-set energy & power densities 3. Generator turns off when a pre-determined resistance level in the ablated tissues is reached (mean of 0. 3 s) Ganz, Gastrointest Endosc, 2004 Dunkin, Surg Endosc 2006 Smith, Surg Endosc 2007
Case Presentation #2 HPI: • 64 year old male with 6 month history of progressive dysphagia • Unintentional weight loss of 12 pounds • Longstanding smoker • No significant reflux symptoms • Presented for outpatient EGD
Bx: adenocarcinoma
Background • Esophageal Cancer: – Worldwide 5 th most common cause of cancer related death – In US 4 th leading cause of cancer mortality • Resectability rate: 60%-90% • Neo-adjuvant chemoradiation commonly used • 5 -year overall survival rate of resectable disease: 10% - 25%
Background • Advances in XRT (IMRT, IGRT, PET-based planning), particularly in esophageal CA • However, these advances only as effective as the accuracy with which target is known • Esophagus represents cancer site affected by one of the widest ranges of inter-observer variability in tumor delineation 1 • Endoscopic clipping has improved definition of gross tumor volume during XRT sim 2 1 Njeh CF. J Med Phys. 2008 2 Pfau PR. J Clin Gastro. 2005
Clinical Need • Accuracy & Precision of Tumor Delineation – Current paradigm entails: • Baseline PET CT (FDG activity, bony landmarks, surgical hardware) • Endoscopy report (distance from incisors) – Challenges of the current paradigm: • • • Dynamic movement of viscera Respiratory variations & cardiac cycle Body habitus changes over treatment
Solution: Paint the Target Fig 1: Fiducial marking proximal mass Fig 2: PET shows optimal fiducial positioning