Adult Wilms ALEJANDRA FUENTES MD PGY4 OCTOBER 27

Adult Wilms ALEJANDRA FUENTES, MD PGY-4 OCTOBER 27 TH, 2016

Case Presentation 37 yo Hispanic female who presented to UMC ED in April 2016 with recurrent R flank pain. PMH - Recent diagnosis of 11 cm “carcinosarcoma of adrenal gland” s/p nephrectomy and adrenalectomy in January 2016 back in Honduras. Treatment presumably complete. - HTN

CT a/p showed in UMC ED showed 8. 3 cm mass in R adrenal fossa with invasion in IVC and R hepatic lobe. She was discharged from ED with pain medication and follow up with surgery and oncology.

Original biopsy sample from Honduras available and evaluated by our pathologists: “Nephroblastoma with predominance of mixed blastemous, stromal, and epithelial elements, favorable histology”. Sample was also sent for expert opinion to Children’s Oncology Group (pending at that point).
 also obtained, demonstrating a “claw sign”")
Initial imaging from Honduras (prior to resection) also obtained, demonstrating a “claw sign” (arrow) – further evidence of renal and not adrenal etiology.

Treatment Planning Tumor Board, May 2016: Considered Stage III disease. Did not consider it a relapse, since she did not receive multimodal treatment for Wilms’ Tumor. Recommended repeat biopsy and further surgical consideration. Surgery concerned about extent of tumor involvement, and recommended neoadjuvant chemotherapy. Radiation Oncology deferred until surgery done. June 3 rd, 2016: Repeat biopsy by IR confirms nephroblastoma.

Treatment June 8 th to July 20 th: Six weeks of neoadjuvant DD 4 A Dactinomycin, vincristine, doxorubicin – protocol shown to have 4 -yr event-free survival and OS estimates of 75 -86% in children with advanced stage Wilms Tumor with favorable histology. stopped DD 4 A after CT scans showed progression of primary mass as well as peritoneal implants. August 5 th, 2016: Repeat biopsy unchanged, still favorable histology without anaplastic features. August 16 th, 2016: Expert pathology opinion from the original tumor sample returned: “a single markedly enlarged and hyperchromatic nucleus present in one slide” with abnormal TP 53 accumulation by IHC in the setting of refractory disease – concerning for anaplastic tumor. August 31 st, 2016: Children’s Hospital Pediatric Tumor board recommends anaplastic chemotherapy protocol followed by surgery.

September 3 rd, 2016: Started Anaplastic Wilms’ Protocol AREN 0321, consisting of 7 weeks of combination cyclophosphamide, doxorubicin, vincristine, carboplatin, and etoposide. September 21: grade 3 neuropathy with foot drop. Discontinued vincristine. September 27: symptomatic and persistent bradycardia during cyclophosphamide infusion. October 18 th: Tumor Board, recognizing limitations in chemotherapy, recommends surgery.

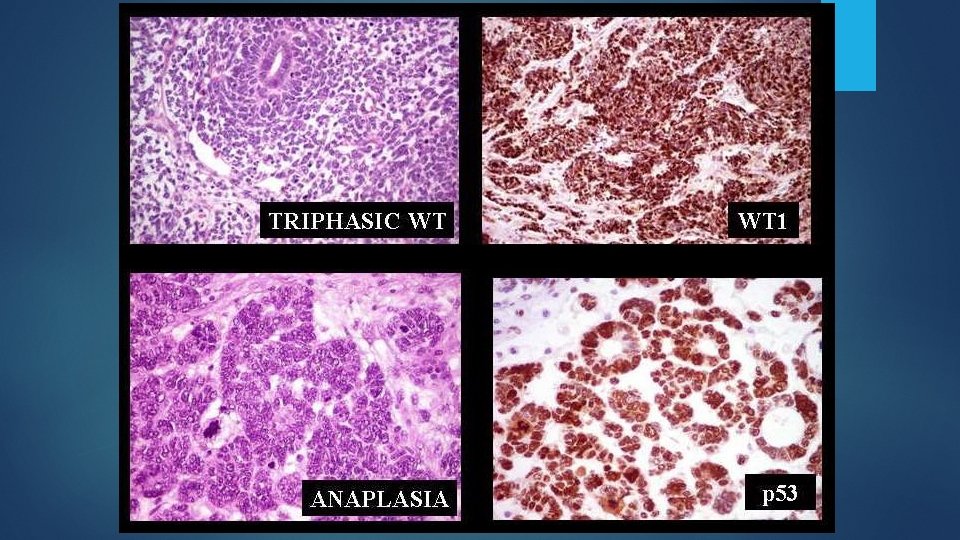
Wilms Tumor - Pathophysiology Originates from metanephric blastemal cells that are unable to complete the mesenchymal-epithelial transition, resulting in triphasic histology. Mutations in the WT 1 gene (tumor suppressor, chromosome 11 p 13) are responsible for 10% of cases. A loss of heterozygosity (LOH) and the “Two -Hit” hypothesis may explain this phenomenon. LOH can be tested for and confers worse prognosis.

Epidemiology Approximately 650 cases of Wilms Tumor in the US each year, with only 3% involving adults. 50% adults presented with advanced (Stage 3 -4) disease, vs 30% children. SEER database analysis: adults (n = 152) had statistically worse OS (69% vs. 88%, P <. 001) than did pediatric patients (n = 2, 190), despite previous studies showing comparable outcome. Adults are more likely than children to have anaplastic histology, which has worse prognosis and response to treatment. Other possible factors: incorrect diagnosis, under-treatment, lack of central review of pathology.

Clinical presentation and Diagnosis Hematuria, flank/abdominal pain, hypertension. Biopsy is controversial because it may lead to seeding. Diagnosis without tissue (via radical nephrectomy) is difficult because it can be radiologically similar to other adult renal malignancies. Histology: Triphasic – blastemic, epithelial, stromal favorable. Can do IHC for cytokeratin, vimentin, desmin, actin, and WT 1 Large, hyperchromic nuclei anaplastic. Can have TP 53 mutations
: recommends radical nephrectomy (accurate diagnosis/staging)")
Treatment Radical nephrectomy National Wilms’ Tumor Study Group (US): recommends radical nephrectomy (accurate diagnosis/staging) before chemotherapy. Society of Pediatric Oncology (Europe): Recommends chemotherapy before radical nephrectomy (better surgical results). Chemotherapy: Adults can be treated with pediatric protocols. Stage I-II: two agents > Stage III: at least 3 agents (usually dactinomycin, vincristine, doxorubicin for favorable histology) Anaplastic or proven LOH mutation: more agents, more aggressive. The most effective chemotherapeutic agents are: Dactinomycin Vincristine Doxorubicin Cyclophosphamide Ifosfamide Etoposide Carboplatin Radiation – it is radiosensitive. Recommended for more advanced tumors.

Poor Prognostic Indicators Anaplastic histology Advanced stage at diagnosis. Molecular features: 1 q gain (most powerful predictor) and LOH of 1 p and 16 q. Older age. If relapsed, < 12 months since last remission.

Summary Wilms Tumor in adults is rare, but carries a worse prognosis than in children. Multimodal approach with surgery, chemotherapy, radiation is best. Children’s protocols can be used in adults, and care is best coordinated closely with pediatric experts. Chemotherapy protocols are complex and determined by histology. QUESTIONS?

References Choi YJ, Jung WH, Shin DW, et al. Histopathological and immunohistochemical features of Wilms Tumor. Korean J Pathol. 1993; 27: 339 -48. Huszno J, Starzyczny-Slota D, Jaworska M, et al. Adult Wilms’ tumor – diagnosis and current therapy. PDQ® Pediatric Treatment Editorial Board. PDQ Wilms Tumor and Other Childhood Kidney Tumors Treatment. Bethesda, MD: National Cancer Institute. Updated <10/12/2016>. Available at: http: //www. cancer. gov/types/kidney/hp/wilms-treatment-pdq. Accessed <10/24/2016> Ali AN, Diaz R, Shu HK, et al. A Surveillance, Epidemiology and End Results (SEER) program comparison of adult and pediatric Wilms’ tumor. Cancer. 2012; 118: 2541 -51.
- Slides: 16