ADULT ECHOCARDIOGRAPHY Lesson Six The Pulmonic Valve Harry

 – Rheumatic (rare) – Carcinoid –")
 –")




")




- Slides: 14
ADULT ECHOCARDIOGRAPHY Lesson Six The Pulmonic Valve Harry H. Holdorf Ph. D, MPA, RDMS, RVT, LRT, N. P.
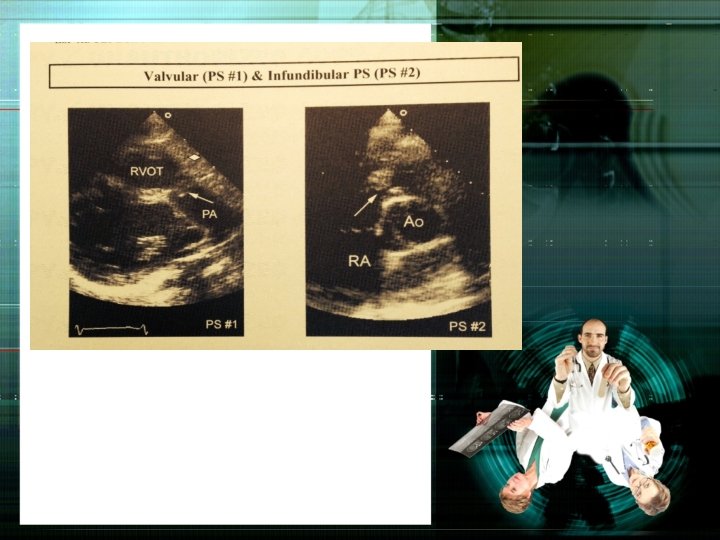
Pulmonic Stenosis • Etiology – Congenital (most common) – Rheumatic (rare) – Carcinoid – Peripheral (PPS-Junction of the R & L Pas) – Infundibular (subvalvular) – Prosthetic valve dysfunction
• Pathophysiology – Systolic pressure overload leads to right ventricular hypertrophy (RVH) – Regional hypertrophy may lead to infundibular stenosis – Commonly associated with other congenital malformations (VSDs, ASDs, tetralogy of Fallot) – RV chamber size usually normal, right atrium will enlarge – Increased risk for endocarditis
• Physical Signs – Dyspnea on exertion – Systolic ejection murmur left upper sternal border (LUSB) – Pulmonary ejection sound, decreased/delayed P 2 – Increased A wave or jugular venous pulsation (JVP) – Sustained RV impulse at midlower left sternal border (LSB)
• ECHO – M-mode may show an increase in the pulmonic “a” dip of more than 7 mm (useful for severe PS only) – Valvular thickening and systolic doming (2 -D) – Right ventricular hypertrophy – Post-stenotic dilatation of the pulmonary artery (PA) – Narrowing of RVOT in infundibular PS (subvalvular in RVOT)
NOTE: – Noonan Syndrome • Classified as a cardiofacial syndrome with PS, HCM and ASD (30%) NOTE: Know that PS dose NOT cause pulmonary hypertension
M-mode of Valvular Pulmonic Stenosis
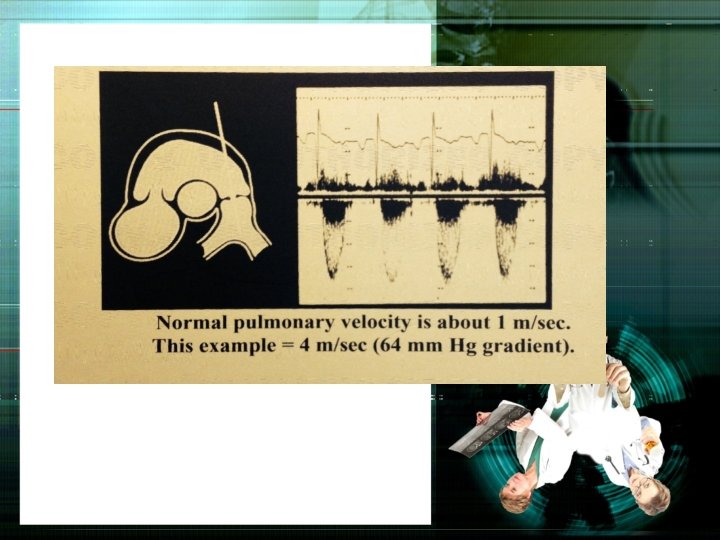
Doppler • Increased velocity and turbulence at level of obstruction (valvular, subvalvular, or supravalvular) • Used pulsed/color flow Doppler to locate level of obstruction • Check for coexisting pulmonic regurgitation • Measure peak and mean gradients (parasternal short-axis Ao. V level and RVOT long-axis are best)
NOTE: If unable to obtain PS gradient from the parasternal window, where else can you go? Subcostal short-axis
• AHA/ACC Guidelines for Pulmonary Stenosis Severity: Mild Moderate Severe Peak Velocity m/s <3. 0 -4. 0 >4. 0 Peak Gradient mm/Hg <36 36 -64 >64
PS Gradients vary with Respiration
End Lesson Six NEXT: THE MITRAL VALVE