Adrenergic Antiadrenergic Drugs By Prof Alhaider Anatomy of

Adrenergic & Antiadrenergic Drugs By Prof. Alhaider

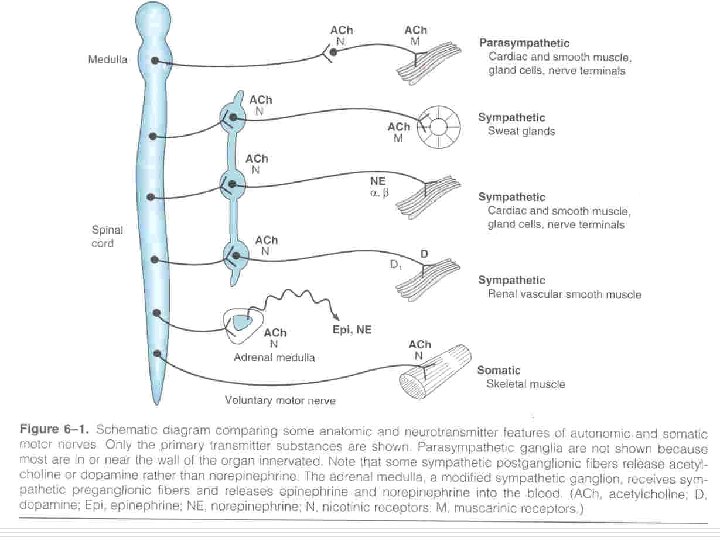
Anatomy of the sympathetic nervous system o The origin is from thoracolumbar segments “all thoracic + lumbers L 1, L 2, L 3 and L 4 ” o They have short preganglionic fibers, and it relays in sympathetic chain ganglia & release Ach in these ganglia o They have long postganglionic fibers that innervate their body organs & release Norepinephrine as a neurotransmitter there
 n Storage of dopamine (DA)")
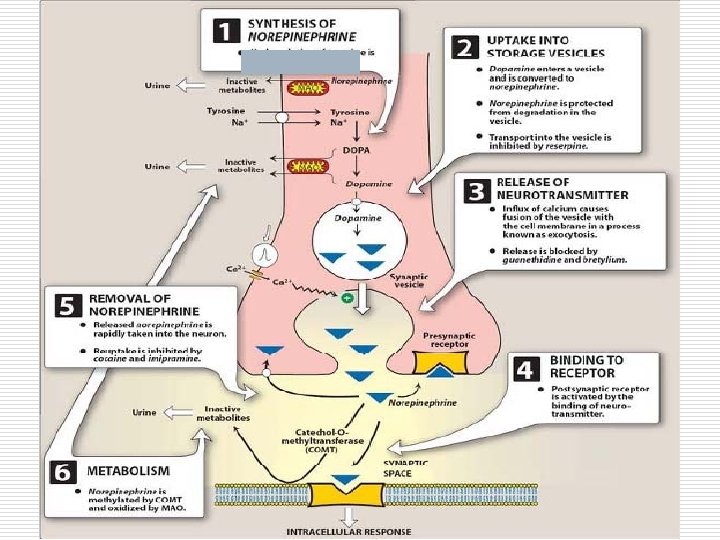
Neurotransmission at adrenergic neurons n Synthesis of norepinephrine (NE) n Storage of dopamine (DA) and NE in vesicles n Release of NE n Metabolism (COMT 20% + MAO 80%) n Binding to receptors n Uptake mechanism

We ask the doctor about the drugs are they included in the exam he said “it’s up to you”

Adrenoceptors o The adrenergic receptors are classified into n n n α 1 α 2 β 1 β 2 β 3 o There are some subtypes

α 1– Adrenoceptors
 Site of α 1– adrenoceptors & the effects of their")
α 1– adrenoceptors (continue) Site of α 1– adrenoceptors & the effects of their stimulation o In vascular smooth muscle. n α 1 stimulation cause vasoconstriction (VC) : o Vasoconstriction in the skin & viscera cause increase total vascular resistance (TVR) causing increase blood pressure (BP) n α 1 – adrenoceptors the most determine of arteriolar tone. When their stimulated no others receptors have an affects on BP. So, hypertension may be treated by blocking α 1 o Vasoconstriction in the nasal blood vessels cause relief of congestion o In the radial muscle of iris. n α 1 stimulation causes contraction of the radial muscle causing mydriasis (dilation of the pupil)

Cont…. o In the smooth muscle of the sphincters of GIT. n α 1 stimulation cause contraction of all sphincters n In the smooth muscle of internal sphincter of urinary bladder (Very important). α 1 a subtypes stimulation cause contraction and closure of the sphincters (precipitate urinary retention) o In the seminal vesicles. (with α 2) n α stimulation cause ejaculation. Thus, all α blockers inhibit ejaculation o In the liver. n α 1 stimulation causes increase glycogenolysis & gluconeogenesis o In the fat cells. n α 1 stimulation causes increased lipolysis

Adrenoceptors α 1 – adrenoceptors Drugs effects : o α 1 selective agonist n E. g. o Phenyl ephrine o α 1 selective antagonists n E. g. o o Prazosin Terazosin Doxazosin Tamsolusin ( α 1 a) (has a different clinical use)

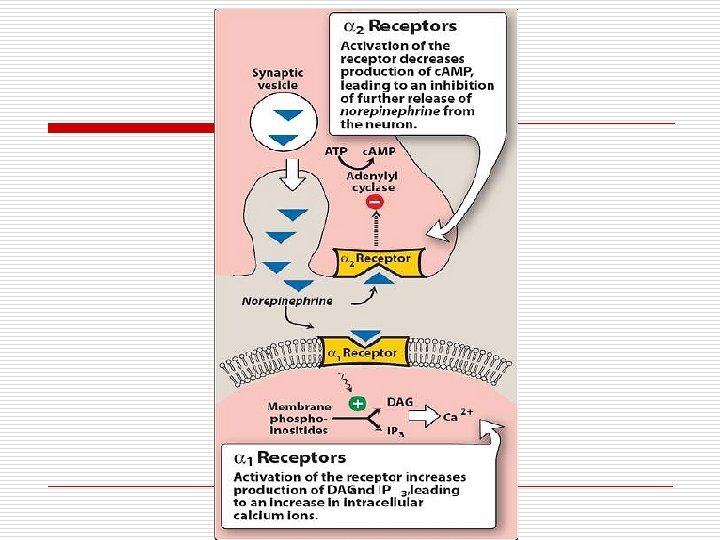
α 2– adrenoceptors Mechanism of action o α 2 stimulation leads to either n Decreased adenylyl cyclase activity(mediated by the inhibitory regulatory Gi protein) o Lead to decrease c. AMP causing decrease NE release causing n relaxation of smooth muscle & n decreased glandular secretion n Increase K+ channel activity hyperpolarization So α 1 receptors are stimulatory while α 2 receptors are inhibitory

α 2–adrenoceptors Site of α 2– adrenoceptors & the effects of their stimulation o In adrenergic nerve terminals (presynaptic). n o In n stimulation cause decreased Norepinephrine release (autoregulatory mechanism). It opposes the action of sympathetic stimulation. pancreas. causes decreased insulin release platelets. Increase platelets aggregation via c-AMP α 2 o In liver (same as α 1– adrenoceptors) o Fat cells (same as α 1– adrenoceptors).

Cont… o In ciliary epithelium. n Increase the out flow of aqueous humor. (good for glaucoma) n In the smooth muscle of GIT wall. (with β 2) α 2 stimulation cause relaxation of the wall causing decreased peristalsis (indirectly by reducing the release of ACH)
 Drugs effects : o α 2 selective agonists n E.")
α 2– adrenoceptors (Continue) Drugs effects : o α 2 selective agonists n E. g. o Clonidine o Methyldopa (Antihypertensive) o Apraclonidine (topical for eye) o α 2 selective antagonists n E. g. o Yohimbine; Mertazapine (Antidepressant)

β 1 – adrenoceptors o In the heart. n β 1 stimulation causes o In S. A node : increase heart rate (HR) (+ve chronotropic) o In Myocardium tissue : increase contractility (+ve inotropic) o In Conducting system : increase conduction velocity (+ve dromotropic) o Increase ectopic beats o In the Juxtaglomerular Apparatus of the kidney. o In fat cells (with α 1, α 2 & β 3) n β 1 stimulation cause increased renin release. Then causes increase in BP n β 1 stimulation causes increased Lipolysis

Adrenoceptors β 1 – adrenoceptor Drugs affecting them o β 1 selective agonists n E. g. o Dobutamine o β 1 selective antagonists n E. g. o Atenolol o Esmolol o Metoprolol

β 2 – adrenoceptors o In the bronchial smooth muscle n β 2 stimulation causes relaxation of smooth muscle (bronchodilatation) o In the smooth muscle of blood vessels supplying the skeletal muscle. n β 2 stimulation causes relaxation of smooth muscle Vasodilatation(VD) o This VD effects is usually masked by the potent VC effect of α 1 – receptors

Cont…. o In the smooth muscle of GIT wall. n β 2 stimulation cause relaxation of the wall leading to decreased peristalsis o In the smooth muscle of the wall of urinary bladder. n β 2 stimulation causes relaxation of the wall n Note: Adrenergic stimulation is opposite to the cholinergic in the wall and sphincters in GIT and genitourinary tract.

Cont…. o In the smooth muscle of the uterus n β 2 stimulation causes relaxation of the uterus (Ritodrine delay the labor) o In the liver. n β 2 stimulation causes increased Glycogenolysis & Gluconeogenesis o In the pancreas. n β 2 stimulation causes slight increase in insulin secretion (hypoglycemia), but the effect on the liver is predominant. o Effect on potassium. n β 2 stimulation increase potassium influx.

Cont…. o In ciliary muscle. n β 2 stimulation causes relaxation of the ciliary muscle leading to o Accommodation for far vision Decrease outflow of aqueous humor via the canal of Schlemm In the ciliary epithelium n β 2 stimulation causes increased production of aqueous humor

Adrenoceptors β 2 – adrenoceptors Drugs affecting them o β 2 selective agonists n E. g. o o o Salbutamol (asthma + ref heperkalemia) Salmetrol Terbutaline Ritodrine Formetrol o β 2 selective antagonists n E. g. o ICI 118551 (still under investigation)

b 1 and b 2 – adrenoceptor agonists Mechanism of action o β stimulation causes increase adneylyl cyclase activity leading to increase c. AMP leading to cellular effect. E. g. n β 1 in the heart cause increase intracellular Ca++ release leading to increased contractility n β 2 in smooth muscle cause inhibition of myosin kinase enzyme causing relaxation n β 2 in the liver cause increase Glycogen phosphorylase enzyme activity causing increased glycogenolysis

β 3 – adrenoceptors o In brown adipose tissue n β 3 stimulation causes increased Lipolysis o β 3 selective agonist n E. g. o BRL 37344 o β 3 selective antagonist n E. g. o CGP 20712 A

Adrenergic Drugs o Adrenoreceptor Agonists n Non selective n Selective o Adrenoreceptor Antagonists n α– blockers n β– blockers
 Catecholamine Drugs")
Adrenoceptor Agonists I. Non selective drugs o These drugs include o 1) Catecholamine Drugs 2) n n catecholamines A. endogenous: High potency o Norepinephrine o Epinephrine Short t 1/2 o Dopamine Given parenterally b) Synthetic (exogenous) o Isoprenaline polar Non-catecholamine Drugs Inactivated by Amphetamine COMT Ephedrine Pseudo ephedrine Phenylpropranolamine noncatecolamine s Low potency Long t 1/2 Can be Given orally Non polar Not inactivated by COMT
(Noradrenaline) o NE is a neurotransmitter released from the postganglionic sympathetic fiber in")
Norepinephrine (NE)(Noradrenaline) o NE is a neurotransmitter released from the postganglionic sympathetic fiber in most organs o It also released from the adrenal medulla (20% of medulla secretion) o It is a direct non–selective adrenergic agonist which acts on all adrenoceptors, Except β 2
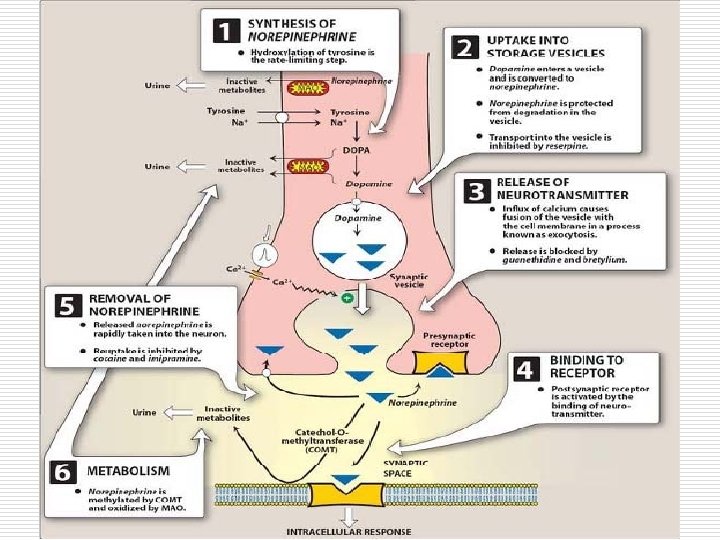

Cont…. o Sites of metabolism n In adrenergic nerves o 80% by MAO in presynaptic nerve terminals after reuptake (This is very important clinically) n If MAO is inhibited, NE will be reuptake but not metabolized, leads to release of NE again o 15% by COMT in postsynaptic membrane (This is not important clinically) o 5% reach the blood and metabolized In the Liver

Norepinephrine Pharmacokinetics o T 1/2 of NE = 2 – 3 min n Very short because it has rapid metabolism o NE causes increased systolic blood pressure (SBP) & diastolic blood pressure (DBP) n So, in shock, it will increase BP o Not given orally because it will be inactivated by intestinal enzymes

o Clinical Uses: o Note: NE is not commonly used in clinical practice like Epinephrine, However it can be used in: n Cardiac Arrest n Shock
(Adrenaline) o EP is released from adrenal medulla (80%) and in certain areas")
Epinephrine (EP)(Adrenaline) o EP is released from adrenal medulla (80%) and in certain areas of the brain o EP is a direct acting non-selective adrenergic agonist in all receptors including β 2 receptor. o T 1/2 = 2 – 5 min o Like NE, It is given parenterally (SC, I. V and I. M) not orally o Has the same pharmacokinetics as NE

Epinephrine Therapeutic use b o Epinephrine is commonly used in practice as compared to NE. o In bronchial asthma o In cardiogenic shock o In anaphylactic shock n It is given SC to act on β 2 receptors to cause bronchodilation n Now it is not commonly used because of its side effects (tachycardia and arrhythmia) n It is given I. V to increase SBP, HR and cardiac output (CO) n It is given SC to act on o α 1 cause VC, lead to increase BP & relief of congestion o β 1 cause increase HR leading to increase CO, so, increase BP o β 2 cause bronchodilation so, relieve bronchospasm
 n It is given I. V. if")
Cont… o In cardiac arrest (for Bradycardia) n It is given I. V. if there is no response, EP given directly into the lung, and if there is no response, it given intracardially, and if there is no response, direct current is applied for 3 times at most o During surgery n EP is added to the local anesthetic to cause VC in the surgery area in order to o Decrease bleeding o Decrease the amount of local anesthetic which will reach the systemic circulation. Therefore, it will decrease the cardiodepressant effect of the local anesthetic
 o It is directly acting synthetic adrenoreceptor agonist acting only on β–")
Isoprenaline (isoproterenol) o It is directly acting synthetic adrenoreceptor agonist acting only on β– receptors, with no effects on a adrenoceptos. o T 1/2 = 5 – 7 min o Like all catecholamines, It is given parenterally (not orally) n The I. V must be given carefully because the overdoses cause cardiac arrest

Iso pre naline Action o Isoprenaline will stimulate n β 1 in the heart to cause o Increased HR & cause arrhythmia & may lead to cardiac arrest n β 2 in the blood vessels to cause o VD leads to decreased BP (mainly DBP)

Isoprenaline Therapeutic uses: o It is no longer used to treat the bronchial asthma because of it’s side effects on the heart o It’s only used now to reverse the heart block which is produced by overdoses of β – blockers N. B. cardiac arrest means : complete cessation of heart’s activity. While heart block means : partial or complete inhibition of the spread of conduction of the electrical impulse from the atria to the ventricles

Effects of I. V. infusion of Epinephrine, Norepinephrine & Isoprenaline in Humans Epinepherine and isoprenaline decrease DBP because they act on β 2 Reflex bradycardia Isoprenaline decrease resistance because it acts on β only without α

Dopamine o DA is a non–selective adrenergic agonist, which acts either directly on DA – receptors in addition to b 1 - adrenergic receptors or indirectly by releasing NE o Like all catecholamines, It is given parenterally only (not orally) o It doesn’t cause tolerance o T 1/2 = 3 – 5 min o Metabolized by either n Converted to NE in adrenergic neurons or n By MAO in the Liver
 o Clinical Uses : n In small dose of DA (=< 5")
Dopamine (Cont…) o Clinical Uses : n In small dose of DA (=< 5 ug / Kg / min by I. V infusion) Renal dose: o It will stimulate DA–receptors only n It will cause vasodilatation (VD) in: § Renal vascular bed § Cerebral vascular bed § Coronary vascular bed § Mesenteric vascular bed Therefore, it is useful in treatment of shock to save these vital organs from hypoxia (also see Dobutamine) N. B : At higher doses, VD effect of DA – receptors is masked by the VC effect of α 1–receptors(see next slide)
 Cardiac")
Cont…. n In medium dose : (5 -15 ug/Kg/min by I. V infusion) Cardiac dose o It will stimulate β 1 – receptors to cause increase HR, CO and BP n In high dose of DA (> 15 ug / Kg / min by I. V infusion) o It will stimulate α 1 receptors (direct + Via release of NE) to cause VC leading to increase BP and decrease organ perfusion So, the high dose of DA is not recommended in shock.

o What is the effect of Dopamine on Bronchioles? It has no effect on the bronchioles because it doesn’t stimulate β 2 receptors (even indirectly , because NE does not stimulate β 2 receptors ).

Centrally Acting Sympathomimetic Agents: e. g: 1. Amphetamine o It is non-selective adrenergic agonist, noncatecholamine n Acts mainly indirectly via, enhancing NE release and DA. n Since it is non-catecholamine, it can be given orally n It is lipid–soluble enough to be absorbed from intestines and goes to all parts including CNS (This leads to CNS stimulation like Restlessness ﻗﻠﻖ and Insomnia )ﺍﻻﺭﻕ. n t 1/2 = 45 – 60 min (long duration of action) n It is metabolized in the Liver.

Clinical use of Amphetamine-like drugs o To suppress appetite n In very obese persons Amphetamine can act centrally on the hunger center in the hypothalamus to suppress appetite o In narcolepsy n Narcolepsy is irresistible attacks of sleep during the day in spite of enough sleep at night n Amphetamine stimulates the CNS & makes the patient awake o In ADHD “Attention Deficit Hyperactivity Disease”
 o Note: Amphetamine is a drug of")
Clinical use of Amphetamine-like drugs (controlled Drugs) o Note: Amphetamine is a drug of abuse, that should not be prescribed. However, amphetamine-like drugs can be prescribed for the following conditions: o In ADHD (Methylphenidate, Dexamfetamine) o In narcolepsy n (Dexamfetamine and Modafinil) o To suppress appetite

Amphetamines Side effects o The side effects are due to chronic use o These include : Tolerance Dependence Addiction Paranoia (thought process heavily influenced by anxiety or fear) n Psychosis (loss of contact with reality) n n

2. Ephedrine o It is non selective adrenergic agonist o It n Directly acts on the receptors (a, b 1, and b 2) It is Like an oral form of Epinephrine. n Indirectly by releasing NE n PK almost similar to amphetamine n It causes tolerance but no addiction n Like amphetamine, it is CNS and respiratory stimulant. n It does not suppress the appetite
 o Decongestant o It")
Ephedrine Clinical uses: o Pressor agent (used to increase BP) o Decongestant o It is no longer used to treated bronchial asthma. (because it’s less potent + slow onset of action)

3. Pseudoephedrine: o Has similar pharmacological activities to ephedrine o It is not controlled : OTC (over the counter) ﻳﺒﺎﻉ ﺑﺪﻭﻥ ﻭﺻﻔﺔ ﻃﺒﻴﺔ o It is commonly used as a decongestant.

4. Phenylpropranolamine: o Again it is similar to pseudoephedrine, and was used as decongestant, but it was stopped because it may cause cerebral hemorrhage 5. Oxymetazoline: Has a 1 and a 2 agonistic activity. Used as a decongestant.

Side – effects of centrally acting sympathomimetics: o o o Sympathomimetic means : n These drugs can produce sympathatic actions similar to EP and NE They include: n Amphetamine n Ephedrine n Pseudo ephedrine n Phenyl Pro Pranolamine They are lipid – soluble and can pass BBB to cause n Insomnia n Restlessness n Confusion n Irritability n Anxiety n Hypertension Remember that amphetamine has additional side effects

Adrenoreceptor Agonists Selective drugs o These drugs include : n n n Phenyl Ephrine (relatively α 1) Clonidine (α 2) Dobutamine (β 1) Salbutamol (β 2) Ritodrine (β 2)
 o It is relatively")
Adrenoreceptor Agonists 1. Phenyl Ephrine (others: methoxamine, metaraminol, mephentermine ) o It is relatively selective α 1–agonist o It is directly acting o PK: not-catecholamine and thus not metabolized by COMT o It has longer duration of action than other catecholamines

Phenylephrine Clinical uses: o As a mydriatic agent to examine the fundus of the eye n It acts on α 1 – receptors in the radial dilator pupillary muscle o As a decongestant n Used as nasal drops to cause VC in the nasal blood vessels & relief congestion o As a vasopressor agent in case of hypotension n α 1 stimulation causes VC leading to increase BP o In case of paroxysmal tachycardia n It cause VC & elevate BP. This stimulate the baroreceptors resulting in increased reflex vagal discharge which brings the heart into the normal sinus rhythm (not in use nowadays)

Clonidine: o It is a selective α 2 – agonist o Mechanism of action : (Acts centrally as a central sympatholytic drug. ) n Clonidine is Lipid – soluble, so, it freely passes BBB & reaches CNS to stimulate α 2 – receptors in medulla and pons causing decreased sympathetic tone and finally decrease BP o It act by it self not like Methyldopa o Clinical use include: n n n Treatment of mild to moderate hypertension Treatment of morphine withdrawal symptoms As analgesic during labour o The dose = 1. 25 ug/day o It can be given I. M o It can be used in patients with renal failure because it dose not affect renal blood flow or GFR & CO

Cont…. o Adverse affects of Clonidine n n n n Depression Dizziness, insomnia, & nightmares Impotence Alopecia ﺗﺴﺎﻗﻂ ﺍﻟﺸﻌﺮ Urticaria Weight gain Fluid retention Sudden withdrawal leads to rebound hypertension Methyldopa and the comparison between it and clonidine are in the lecture (adrenergic antagonists)

3. Apraclonidine o Like clonidine it is selective α 2 adrenoceptor agonist, however, main uses as adjuvant therapy for glaucoma via decrease of aqueous humour formation.
 4. Dobutamine: o It is direct acting β 1")
Adrenoreceptor Agonists (Cont. . ) 4. Dobutamine: o It is direct acting β 1 – selective agonist o T 1/2 = 10 – 15 min o It is metabolized in the liver by oxidative deamination o There is tolerance to its action o Given only parenterally (not orally) o It causes increases in CO with minimal effect on HR. (because of the baroreceptor reflex) o It has less arrhythmogenic effects than dopamine o Uses: Inotropic agent for Heart Failure; in septic and cardiogenic shock.

Adrenoreceptor Agonists 5. Salbutamol: o It is β 2 – selective agonist o Can be used orally, IV and by inhalation o Formulations: (Tablets; Syrup; Injection; solution and Inhalation) o Clinical Uses n bronchial asthma by β 2 stimulation, which leads to relaxation of bronchial smooth muscle and bronchodilation. n Treatment of refractory hyperkalemia (I. V)

6. Salmetrol and Formoterol: n These selective beta agonists, have longer duration of action as compared to Salbutamole. n Uses: As inhalors for bronchial Asthma

7. Ritodrine: o It is another β 2 – selective agonist but o It is used to delay premature labour n β 2 stimulation leads to relaxation of uterine smooth muscle leading to delay of labour o This is done to ensure adequate maturation of fetus

Clinical applications of Sympathomimetic drugs o In shock n Type of shock include o Hypovolamic shock o Septic shock o Anaphylactic shock n n Symptoms include § Congestion in the Lung, Heart & Kidney due to VD & V. Per? ? § Bronchoconstriction § Hypotension We use EP with steroid antihistamine to cause § Bronchodilation § Increase BP § Decongestant o Neurogenic shock o Cardiogenic shock n n We use DA & Dobutamine together All type lead to increases in BP? ? ? (I think shock is associated with increased BP)
- Slides: 63