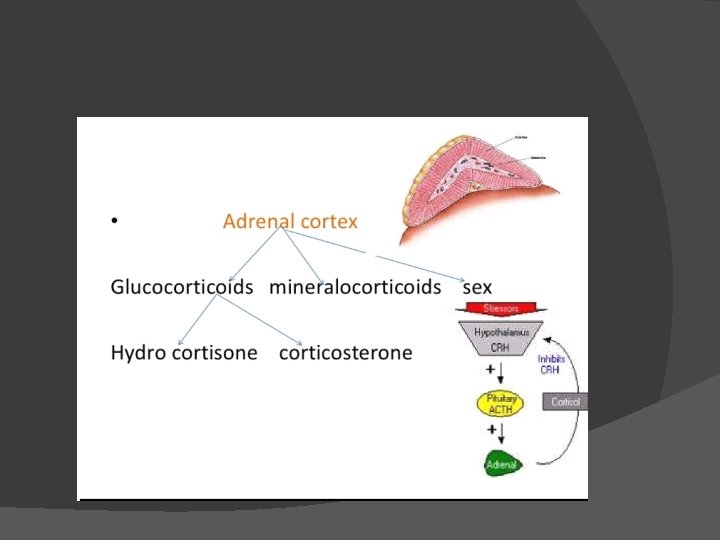
ADRENAL GLANDS DR Zaeem dahla Consultant General surgeon





SYNDROME � Hypertension , hypokalemia , hyper secretion of aldosterone. � Hypertensive")
 � Pathology: � Most unilateral adrenocortical adenoma(conns syndrome) � 20 -40%")



- Slides: 40
ADRENAL GLANDS DR. Zaeem dahla Consultant General surgeon
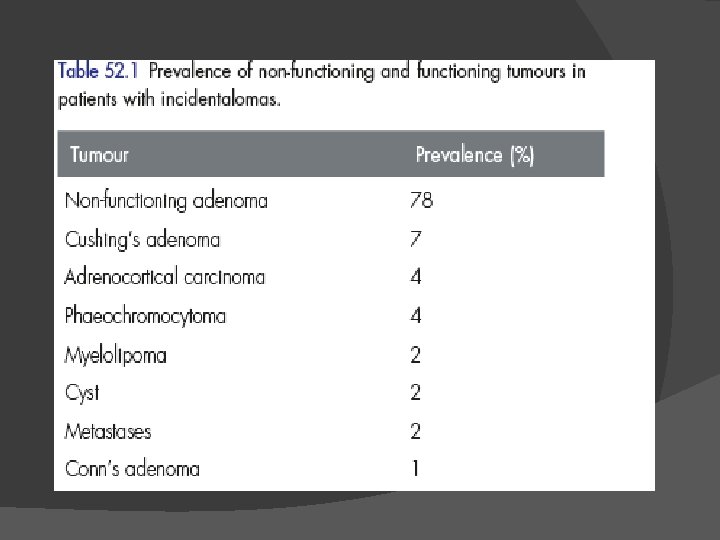
INCIDENTALOMA � DEFINITION ; a clinically unapparent mass � � � � � detected incidentally by imaging studies conducted for other reasons. Incidence; 1. 4%--8. 7% increase with age. DIAGNOSIS; Hormone evaluation; morning and mid night plasma cortisol measurements. 1 mg dexamethasone suppression test. 24 h urinary cortisol level. 24 hs urine cortisol metabolite. S k , aldosterone , renin activity. CT, MRI. Adrenal gland biopsy.
INVESTIGATION � When incident Loma identified , good informative history and physical examination , should be done. � Occult endocrine disease my be detected. � Biochmemical work up should be done. � Hormonal evaluation should be done.
Hormonal evaluation Morning and mid night cortisol level. � 1 mg dexamethasone suppression test. � 24 h urinary cortisol excretion. � 12 -24 h metanephrines & plasma metanephrines level. � Serum plasma aldosterone , plasma Renin. � DHEAS , testosterone , or 17 hydroxyestradiol (virilizing or feminizing tumors). � Imaging technique CT, MRI. �
TREATMENT mass >4 cm , smaller tumor that increase in size---resection. � Non-functioning tumor less than 4 cm , followed up for 6, 12, 24 months. � Non-functioning
PRIMARY HYPERALDOSTERONISM(CONN”S )SYNDROME � Hypertension , hypokalemia , hyper secretion of aldosterone. � Hypertensive patient with hypokalemia 2%. � Hypertensive patient with normal potassium 12%.
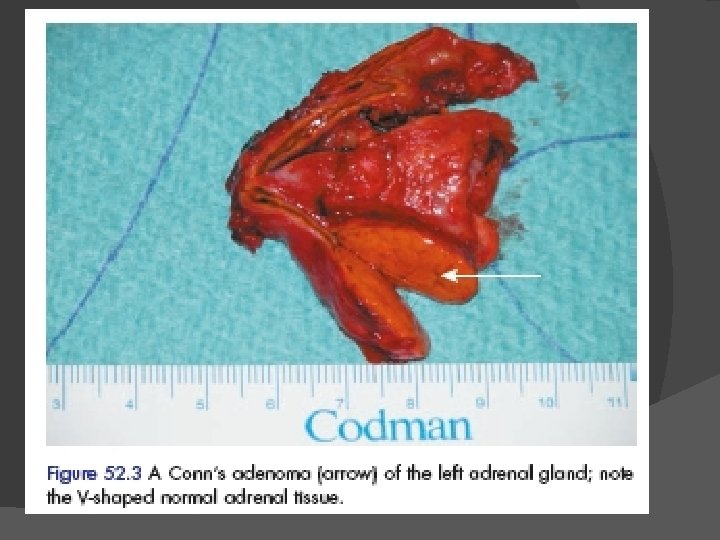
Primary hyper aldosteronsim(PHA) � Pathology: � Most unilateral adrenocortical adenoma(conns syndrome) � 20 -40% bilateral adrenal hyperplasia. � Rare; carcinma
Clinical features Age; 30 -50 ys with female predominance. � Hypertension. � Headache. � Muscles weakness. � Cramps � Intermittent paralysis � Polyuria � Polydipsia � Nocturia �
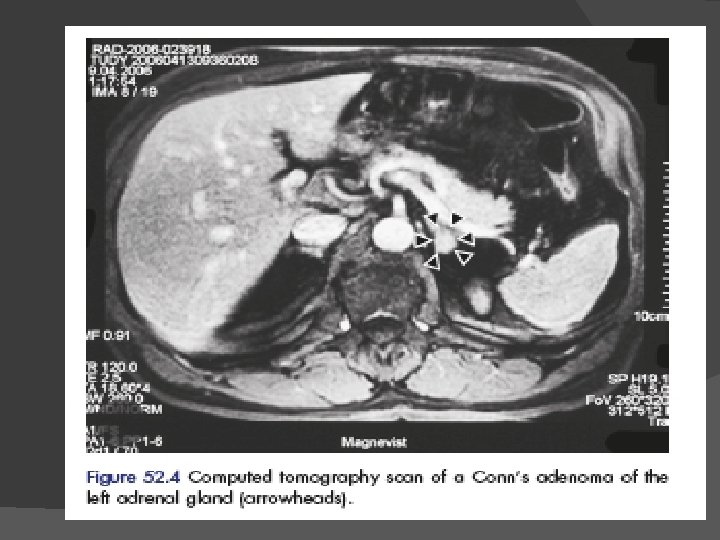
DIAGNOSIS Biochemical test ; Asses potassium , aldosterone, level to plasma renin activity. � MRI, CT, to distinguish unilateral from bilateral. � Conns adenoma usually measure 1 -2 cm. � Selective adrenal vein catheterization , for sample taken, Aldosterone & cortisol ratio. differentiate unilateral from bilateral active gland. �
TREATMENT � Frist line of treatment with bilateral hyperplasia is medical= spironolactone. � Antihypertensive medication. � Lap. surgical resection for disease gland.