ADRENAL GLAND Dr Bushra AlTarawneh Weight of normal

ADRENAL GLAND Dr. Bushra Al-Tarawneh

� Weight of normal gland is 4 gm. Adrenal Cortex - Derived from mesoderm , composed of : 1 - Zona glomerulosa mineralocorticoids( aldosteron). 2 - Zona fasciculata glucocorticoids ( cortisol ). 3 - Zona reticularis estrogens & androgens. Diseases are those of hyperfunction & hypofunction. Adrenal Medulla - Derived from neural crest & is part of sympathetic system. Composed of Chromaffin cells secreting catecholamines. Diseases are mainly tumors 2

3

Medulla ZR ZF ZG 4

5

6

7

CUSHING’ Syndrome Elevation of cortisol level , which occurs in : A- Endogenous causes : i-Hypothalamic/ pituitary hypersecretion ACTH. ii- Paraneoplastic syndrome ( lung CA ). iii-Adrenal tumor or hyperplasia. B- Exogenous cause : Steroid Therapy. Cushing’s diseases is a primary pituitary lesion ACTH 8
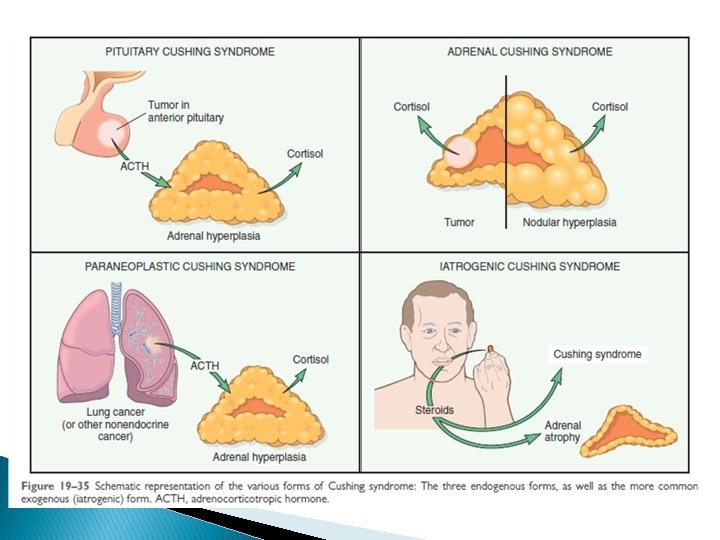

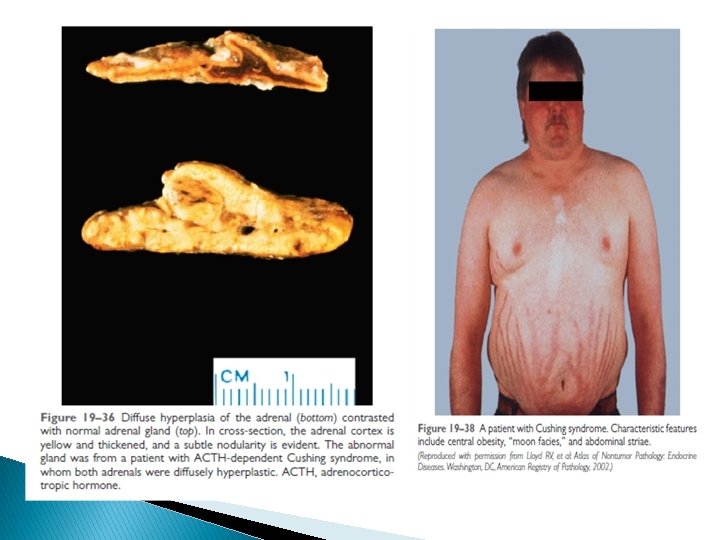
Morphology of adrenals in Cushing’s Syndrome : � This depends on the cause : 1 - Exogenous increase glucocorticoids ACTH Bilateral atrophy of adrenals. 2 -Endogenous hypercorticolism: a- Presence of adrenal adenoma or carcinoma, with atrophy of adjacent & contralateral adrenal. b- Secondary to ACTH secreting pituitary adenoma bilateral diffuse or nodular hyperplasia **Main clinical symptoms of Cushing’s include : Central obesity, Hirsutism , Hypertension, Diabetes Osteoporosis. 10

11

HYPERALDOSTERONISM : A-The potential causes of primary hyperaldosteronism are: • Bilateral idiopathic hyperaldosteronism, characterized by bilateral nodular hyperplasia of the adrenal glands. This mechanism is the most common underlying cause of primary hyperaldosteronism, accounting for about 60% of cases. The pathogenesis is unclear. • Adrenocortical neoplasm, either an aldosterone-producing adenoma (the most common cause) or, rarely, an adrenocortical carcinoma. In approximately 35% of cases, primary hyperaldosteronism is caused by a solitary aldosterone-secreting adenoma, a condition referred to as Conn syndrome. • Rarely, familial hyperaldosteronism may result from a genetic defect that leads to overactivity of the aldosterone synthase gene, CYP 11 B 2. aldosteron Na retention & K excretion BP , Hypokalemia , RENIN. B- Secondary causes : Due to decreased renal perfusion ( heart failur ), activation of the renin - angiotensin system aldosteron. Differentiate from primary by RENIN. 14
: Result from adrenogenital syndrom result from abnormal production of adrenal androgens.")
VIRILIZING Syndromes (hyperandrogen): Result from adrenogenital syndrom result from abnormal production of adrenal androgens. Typically associated with either androgen excess or deficiency. Could be caused by : 1 - Primary gonadal disorders(increase gonadal androgen). 2 -Acquired : Adrenocortical Neoplasms. can occur at any age, frequently malignant. 3 - Congenital adrenal hyperplasia: is caused by an enzyme defect in cortisol biosynthesis (21 hydroxylase) NO CORTISOL ACTH androgenic steroids (virilizing activity ). � Virilization in female or precocious puberty in male. � Patients have risk for acute adrenocortical insufficiency. � Note : Adrenal androgen formation is regulated by ACTH , thus increase androgen can occur as apure syndrome or as a component of cushing syndrome. 15
")
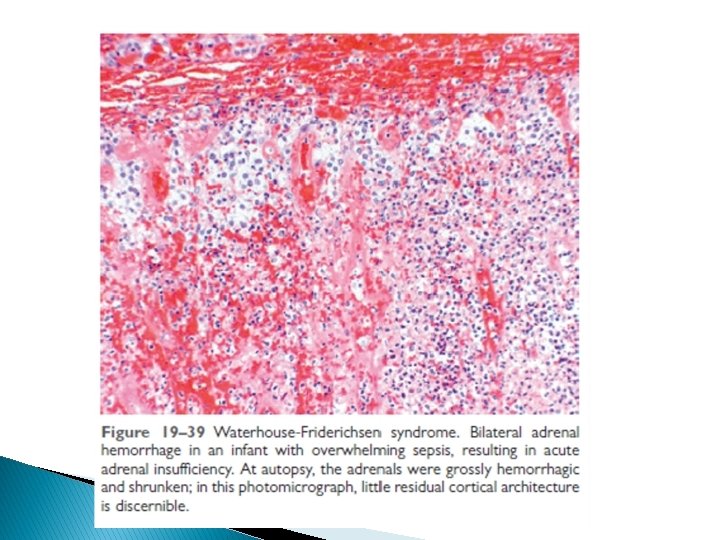
ADRENOCORTICAL INSUFFICIENCY : � May be primary adrenal( disease affecting the adrenal gland ) or secondary to destruction of the pituitary as in SHEEHAN’s syndrome or non functional pituitary adenoma : loss of ACTH. � Primary adrenal may be : A- Acute : 1 - Sepsis e. g. Waterhouse- Friderichson syndrome. 2 - Sudden withdrawal of steroid therapy ( RA ). 3 - Stress in a pt. with underlying chronic insufficiency. Adrenals may show massive hemorrhage 16
 B- Chronic : ( Addison’s disease ) -Chronic adrenal cortical")
Adrenal insufficiency (continued ) B- Chronic : ( Addison’s disease ) -Chronic adrenal cortical insufficiency , required immediate therapy. -Progressive destruction of the adrenal. Causes include: 1 - Autoimmune - 60 -70 % , may be sporadic or familial, linked to HLA-B 8 or DR 3 Often multisystem involvement. 2 - Infections e. g. Tuberculosis , fungi. 3 - Metastatic tumors destroying adrenal e. g. lung , breast , …others 4 - AIDS. 18

� � APS 1 is characterized by chronic mucocutaneous candidiasis and abnormalities of skin, dental enamel, and nails (ectodermal dystrophy) occurringin association with a combination of organ-specific autoimmune disorders (autoimmune adrenalitis, autoimmune hypoparathyroidism, idiopathic hypogonadism, pernicious anemia) that result in destruction of target organs. APS 2 manifests as a combination of adrenal insufficiency and autoimmune thyroiditis or type 1 diabetes.

Morphology & Clinical features in Chronic Adrenal Insufficiency : � Morphology depends on cause : Autoimmune shows irregular small glands, with cortex heavily infiltrated by lymphocytes, medulla normal. In T. B. Caseating Granuloma In metastatic CA Type of primary tumor In secondary to pituitary cause, the adrenal is shrunken Ø In general, clinical manifestations of adrenocortical insufficiency do not appear until at least 90% of the adrenal 20

� The initial manifestations often include progressive weakness. � In patients with primary adrenal disease, increased levels of ACTH precursor hormone stimulate melanocytes, with resultant hyperpigmentation of the skin and mucosal surfaces. However The hyperpigmentation is not seen in patients with secondary causes. Decreased mineralocorticoid (aldosterone) activity in patients with primary adrenal insufficiency results in potassium retention and sodium loss, with consequent hyperkalemia, hyponatremia, volume depletion, and hypotension, whereas secondary hypoadrenalism is characterized by deficient cortisol androgen output but normal or near-normal aldosterone synthesis. Ø Ø Hypoglycemia occasionally may occur as a result of glucocorticoid deficiency and impaired gluconeogenesis. Ø Stresses such as infections, trauma, or surgical procedures in affected patients may precipitate an acute adrenal crisis, manifested by intractable vomiting, abdominal pain, hypotension, coma, and vascular collapse. Ø Death follows rapidly unless corticosteroids are replaced immediately.

Adrenal tumor ADRENALCORTICAL TUMORS or THE ADRENAL MEDULLA TUMOR

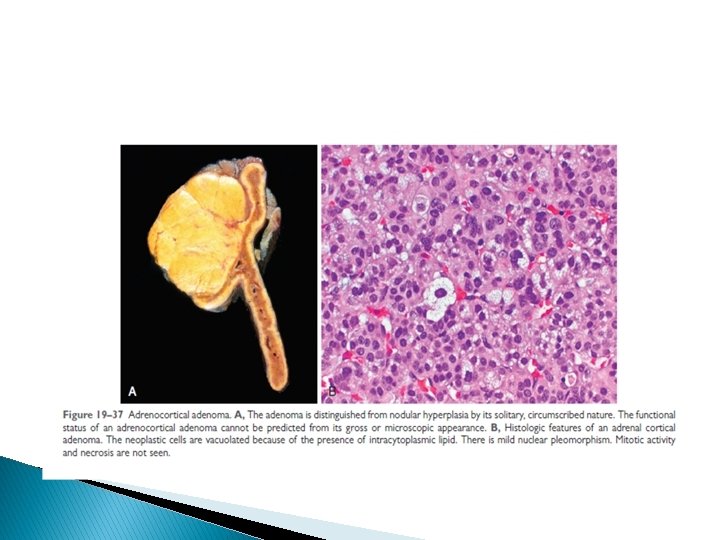
MORPHOLOGY in ADRENALCORTICAL TUMORS: � Encapsulated , usually yellow color: single or multiple. � Size variable 1 -2 cm. Up to large tumors � Malignant tumors may show necrosis, hemorrhage, and are usually larger. � Functioning or nonfunctioning tumors (hormones). � Both may show same appearance of uniform or slightly pleomorphic cells , which may be eosinophilic or clear � In many cases, the presence of metastases is the only way to differentiate benign from malignant tumors. 23

Tumor of the adrenal medulla 1 -PHEOCHROMOCYTOMA : � Sometimes described as Ruleof 10% Tumor because : * 10% bilateral. , 10 %multiple, 10% non functional * 10% familial, may be part of MEN syndrome. * 10% Malignant. * 10% extraadrenal site. *25% associated with genetic mutation. � 90% associated with catecholamine secretion. � VMA excreted in 24 hr. urine helpful in diagnosis. � Usually well circumscribed, small to large in size. � By morphology: Nests of cells (Zellballen) with abundant cytoplasm filled with granules containing catecholamine. � Malignancy confirmed by METASTASES � Clinically sustained or paroxysmal attacks of BP. � Hypertension resistant to standard antihypertensive therapy. 24

25

2 -NEUROBLASTOMA : � Malignant tumor composed of primitive nerve cells precursors derived from the neural crest. � Commonest extracranial solid tumor of childhood � Usually adrenal but maybe extra-adrenal � Familial or sporadic � Associated with deletion of short arm of chromosome 1. � Morphologically it is composed of small round blue cells which may differentiate to ganglion cells. � Spread to adjacent organs, lymph nodes, renal vein. � Haematogenous metastasis occure early to liver &bone. � Prognosis : STAGE , N myc amplification � Mostly respond well to chemotherapy. 26

27
- Slides: 27