Adrenal disease Dr bandar ghazal Each Adrenal gland

Adrenal disease Dr. bandar ghazal

• Each Adrenal gland lie superior to each kidney. • Pyramidal in shape. • 3 - 5 cm in height , 3 cm in width , less than 1 cm thick • Mass 3. 5 - 5 g • Gland differentiate in two distinct regions large ( 80 % ) cortex ( mesoderm ) Small ( 20 % )medulla (ectoderm ) Capsule covering the gland Highly vascularized structure.
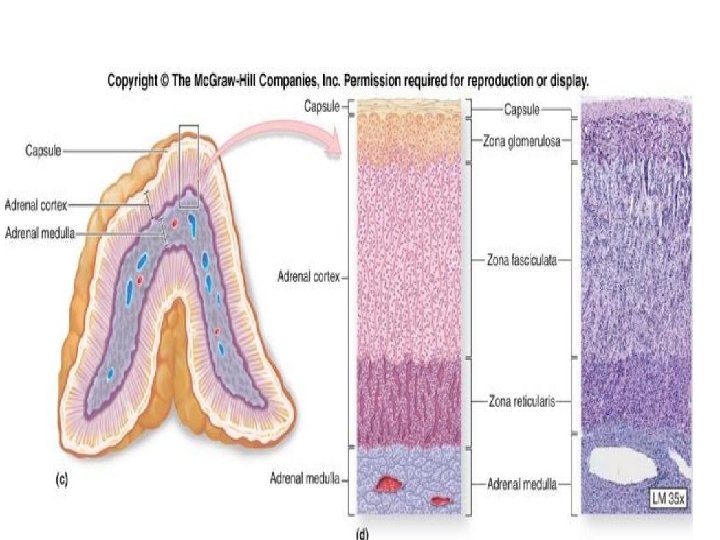

Adrenal hormones • Zona Glomerulosa : mineralocorticoids Major : ALDOSTERONE Regulate blood volume , pressure , NA and K. Also promote H excretion in urine. Aldosterone secretion stimulated by reninangiotensin- aldosterone pathway. And to lesser extent by ACTH.
 account for 95 % Cortisone ,")
• Zona Fasciculata: glucocorticoids Cortisol (hydrocortisone ) account for 95 % Cortisone , Corticosterone CRH corticotropin releasing hormone promote secretion of ACTH (adrenocorticotropic hormone) • Function of corticosteroids : Protein breakdown : increase amino acid in blood Glucose formation : gluconeogenesis Lipolysis : breakdown triglycerides Resistance of stress Makes blood vessel sensitive to other hormone causing vasoconstriction such increase BP Anti inflammatory , alteration of wound healing Depression of immune system.

• Glucocorticoid: -cortisol level are highest in the morning and lowest in the middle of the night ( diurnal rhythm ) cortisol rises dramatically during stress (e. x: illness, starvation) • Most of cortisol circulates in blood attached to cortisol binding protein , with small amount circulate as biologically active free hormone. • Zona reticularis : produce small amount of androgen. DHEA ( dehydroepiandrosterone ) Weak androgen with peripheral conversion to testosterone.
 regardless the cause.")
Cushings syndrome • Excessive activation of glucocorticoid receptors. ( syndrome ) regardless the cause. 1. Exogenous- Prolonged administration of Prednisolone. 2. Endogenous. Cushing disease : endogenous high cortisol due to high ACTH from pituitary tumor
 • Ectopic ACTH")
• ACTH-dependent : • Pituitary adenoma secreting ACTH (Cushing's disease) • Ectopic ACTH syndrome (bronchial carcinoid, small-cell lung carcinoma, other neuro-endocrine tumor) Non-ACTH-dependent : • Adrenal adenoma • Adrenal carcinoma • ACTH-independent macronodular hyperplasia; primary pigmented nodular adrenal disease.

Signs and symptoms

• • Striae : especially reddish > 1 cm width Easy bruising Facial plethora Dorsocervical and supraclavicular fat pads.


Urine free cortisol: 24 -hr timed collection, elevated if above reference")
Initial testing • 1)Urine free cortisol: 24 -hr timed collection, elevated if above reference range for assay • 2)late night salivary cortisol 11 pm – 12 pm at least 2 different nights Loss of diurnal rhythm. • 3)overnight dexamethasone suppression test: 1 mg orally at 11 pm, measure plasma cortisol at 8: 00 am (<50 nmol/l ) exclude cushing syndrome. >138 nmol/l considered positive • When suspicion of cushing is low , single test if negative makes cushing syndrome is unlikely. • • When suspicion of cushing is high ? ? ? Two different test are recommended

• Pseudo cushings : Occur with major depression , anxiety , psychosis , poorly controlled DM and sever visceral obesity
Low dose dexamethason suppression test: Serum cortisol is measured following administration")
Confirmatory test • 1)Low dose dexamethason suppression test: Serum cortisol is measured following administration of 0. 5 mg 6 -hourly for 48 hour (<50 nmol/l ) exclude Cushing syndrome • 2)High dose dexamethasone suppression test: Serum cortisol is measured following administration of 2 mg 6 -hourly for 48 hour • 3)Measuring plasma ACTH: <1. 1 pmol/L ACTH-independent cause > 3. 3 pmolL ACTH-dependant cause

• Adrenal CT scan or MRI • Pituitary MRI In case of ACTH dependent If no tumor , or if tumor is less than 6 mm High dose dexamethasone suppression test to evaluate for ectopic ACTH

Management • • Most patients are treated surgically, but medical therapy may be given in severe cases for a few weeks prior to operation to improve the clinical state. A number of drugs are used to inhibit corticosteroid biosynthesis, including metyrapone and ketoconazole. • • If the patient have cushing disease --transphenoidal surgery

hyperaldosteronism

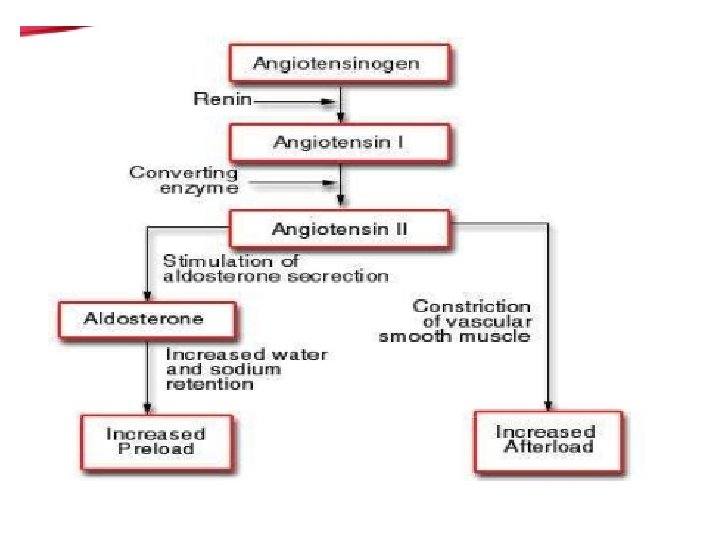
PATHOPHYSIOLOGY • Stimuli of aldosterone secretion : • • 1 - angiotensin II ( the principal stimulus ). 2 - increased K+. 3. decreased volume. 4. lesser extent by ACTH. • suppressors of aldosterone secretion : • 1 - hypervolemia 2 - hypokalemia
 • Renin : a proteolytic enzyme , released")
RAAS ( RENIN ANGIOTENSIN ALDOSTERONE SYSTEM) • Renin : a proteolytic enzyme , released by the kidneys , in which the primary site of it’s storage and release is the JGA. • • It’s release is stimulated by : 1 - sympathetic activation. 2 - renal artery hypo perfusion 3 - decreased Na delivery to the distal tubules

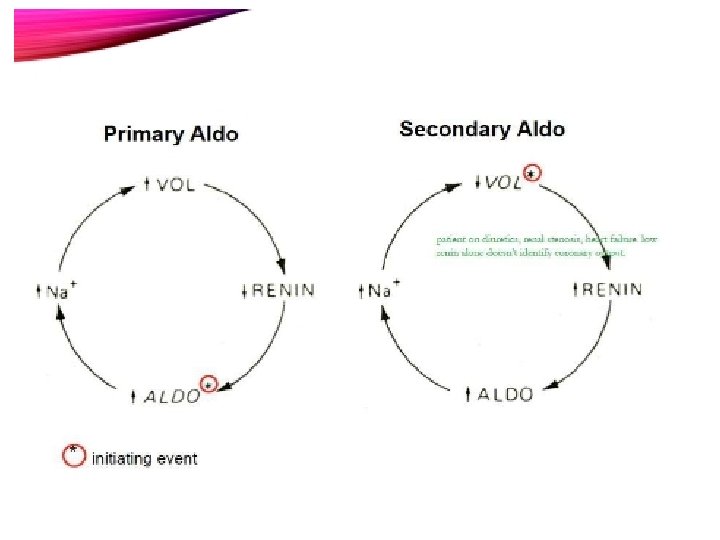
PRIMARY HYPERALDOSTERONISM • -Increased mineralocorticoid secretion from the adrenal cortex. • -Low renin levels but high aldosterone levels

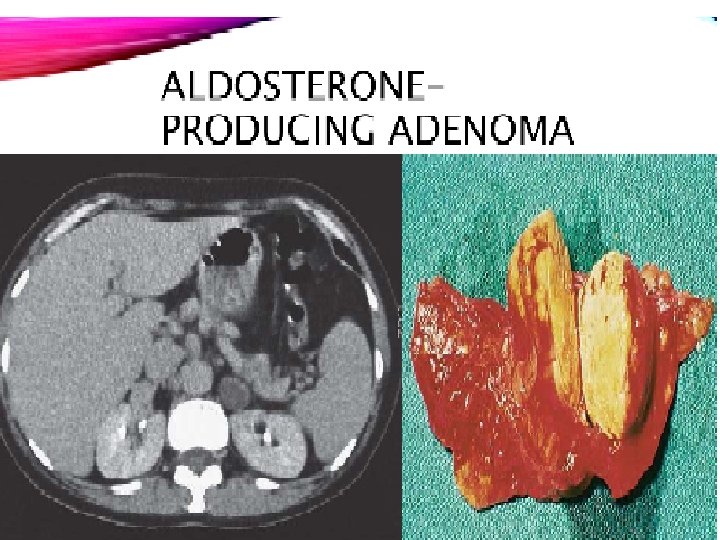
Etiology • Idiopathic bilateral adrenal hyperplasia. Tow third of cases • - Adrenal adenoma secreting aldosterone (Conn’s syndrome). One third of cases
")
- hypertension. - hypokalemia , muscle weakness or even paralysis. ( 40 % ) - Hypernatremia. - Excess thirst , polyuria due low K level - Higher cardiovascular mortality and morbidity noted in primary hyperaldosteronism compared to PT with essential HTN with similar BP.

PA ? ? ? • HTN > 140 /90 on three drug therapy • HTN with spontaneous hypokalemia or diuretic induce hypokalemia. • Untreated HTN with sustained BP >150 /100 • HTN with incidental adrenal mass • HTN in setting of first degree relative with PA. • HTN in setting of family history of HTN onset age < 40.

Investigations • Biochemical – • Routine blood tests • - Aldosterone: renin ratio ( ARR ) Mid morning seated sample If pt taking ACEI , ARBS , spironolactone ? ? An ARR greater than 20 with plasma aldosterone concentration of at least 15 ng / dl is considered a positive test • confirmatory test : suppression tests ( normal saline , fludrocortisone , Na. Cl tabs ) Infuse 2 liter 0. 9% over 4 hours or 10 -12 g daily of NACL tab for 3 days Blood level : plasma aldosterone >5 ng /dl confirm diagnosis 24 Hr urine collection for aldosterone , creatinine and NA Aldosterone in urine >10 microg/24 hr confirm diagnosis

• Adrenal CT : Result : NL Hyperplasia Unilateral or bilateral adenoma Incidental adrenal mass may or may not related to primary aldosteronism • Adrenal vein sampling to measure aldosterone.
 for hypertension and")
Management • - Mineralocorticoid receptor antagonist ( spironolactone , eplerenone ) for hypertension and hypokalemia other anti HTN medications. • For unilateral disease : Laparoscopic adrenalectomy 40 % of PT cured after surgery others BP significantly improve. Persistent HTN after surgery may occur due to primary HTN or due to vascular changes caused by HTN.

SECONDARY HYPERALDOSTERONISM • • high renin and aldosterone levels. • Etiology : • 1 - Inadequate renal perfusion ( HF , RA stenosis , diuretic therapy ) • 2 - renin-secreting renal tumor ( very rare)

Adrenal insufficiency

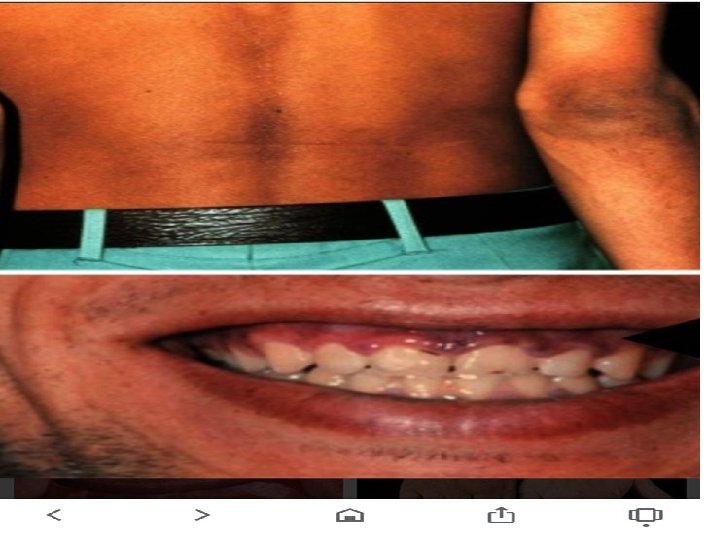
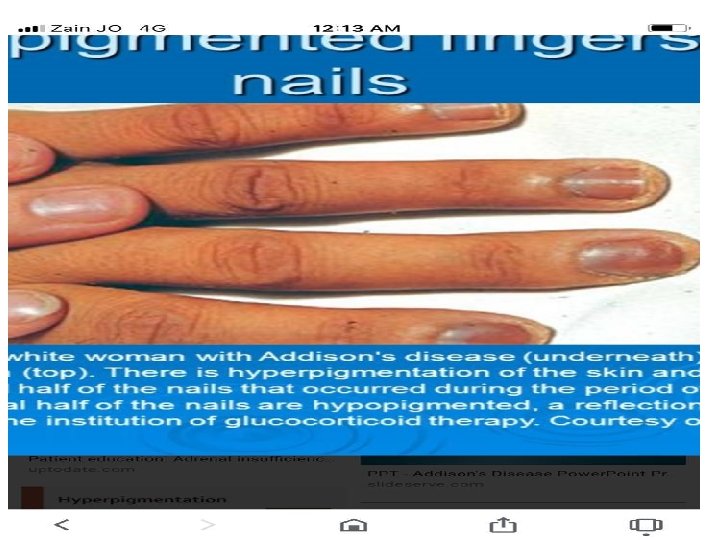
• -It results from inadequate secretion of cortisol and/or aldosterone. • PRIMARY Endogenous Failure of adrenal gland to secret hormones Presence of hyperpigmentation due to stimulation of melanocytes by high ACTH. • SECONDARY most common cause and its due to ACTH deficiency usually due to inappropriate steroids withdrawal , or pituitary tumor ADRENAL CRISIS Potentially fatal and variable in its presentation , usually precipitated by acute illness or replacement of thyroid hormone in un recognized chronic adrenal insufficiency •
 1 -Addison’s disease •")
Causes of adrenal insufficiency • Primary adrenal insufficiency (High ACTH) 1 -Addison’s disease • Autoimmune. ( most common ) destruction of all 3 layers , most pt have positive 21 – hydroxylase antibodies. 50 % of these pt may develop autoimmune endocrine disorder (primary hypothyrodism , celiac disease type 1 DM , hypoparathyrodism ) 2 -Other causes : • TB , fungal infection • HIV/AIDS • Sarcoidosis , hemochromatosis • Metastatic carcinoma ( lung cancer , renal cell cancer ) lymphoma • Bilateral adrenal hemorrhage, sepsis and DIC , anticoagulation protein C deficiency.

2 - Corticosteroid biosynthetic enzyme defects – - Congenital adrenal hyperplasia's. 21 hydroxylase deficiency
: • -sudden Withdrawal of glucocorticoids therapy. •")
• Secondary adrenal insufficiency (Low ACTH): • -sudden Withdrawal of glucocorticoids therapy. • -Hypothalamic or pituitary disease.

CLINICAL ASSESSMENT • In addison’s disease, either glucocorticoid or mineralocorticoid deficiency might come first, but eventually all patients fail to secrete both. • Patients may present with chronic features (weakness, fatigue and hyperpigmentation) and/or in acute circulatory shock. • These symptoms are often misdiagnosed as chronic fatigue syndrome or depression. • Adrenocortical insufficiency should be considered in patients with hyponatremia even in the absence of symptoms.
 • Weight loss •")
CLINICAL FEATURES in primary disease (SYMPTOMS CAUSED BY GLUCOCORTICOID INSUFFICIENCY) • Weight loss • Anorexia • fatigue • Nausea and vomiting • Diarrhoea or constipation • Postural hypotension • Shock. • Hyponatremia. • hypoglycemia
 • Hypotension. • Shock. • Hyponatremia.")
ADDISON’S DISEASE CLINICAL FEATURES (CAUSED BY MINERALOCORTICOID INSUFFICIENCY) • Hypotension. • Shock. • Hyponatremia. • Hyperkalemia.
 • Decreased body hair • Loss of")
SYMPTOMS ARE DUE TO ADRENAL ANDROGEN INSUFFICIENCY) • Decreased body hair • Loss of libido especially in female

Secondary disease • All symptoms mentioned above. • Pt don’t develop hyperpigmentation. • no hyperkalemia.

ADRENAL CRISIS -Primary acute hypoadrenalism. sever fatally symptoms -Causes: stress, rapid withdrawal of steroids, adrenal hemorrhage, surgery and infection. -Circulatory shock with severe hypotension, hyponatremia, hyperkalemia. In some instances hypoglycemia.

Treatment should not be delayed to wait for results in patients with suspected acute adrenal crisis. If the patient’s condition permits, it may be appropriate to perform a short ACTH stimulation test before administering hydrocortisone. Investigations should be performed before treatment is given if the patient’s symptoms suggest chronic adrenal insufficiency

MANAGEMENT OF ADRENAL CRISIS 1 -correct volume depletion with IV saline to normalise BP 2 -replace glucocorticoids 3 -correct other metabolic abnormalities 4 -Identify and treat the underlying cause

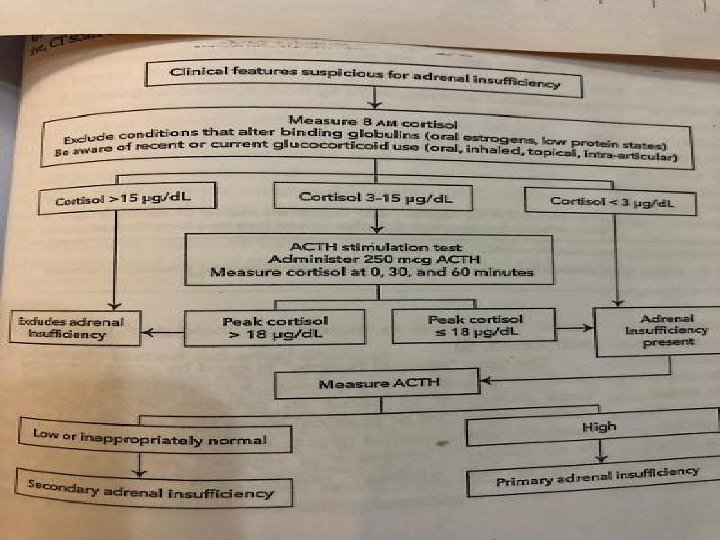
• Random plasma cortisol is usually low in patients with adrenal insufficiency but it may be within normal range, yet inappropriately low, for a seriously ill patient. • ACTH stimulation test is more useful: Cortisol levels fail to increase in response to exogenous ACTH in primary adrenal insufficiency.
: • oral hydrocortisone 15 -20 mg daily in divided")
MANAGEMENT • -Glucocorticoid replacement (always): • oral hydrocortisone 15 -20 mg daily in divided doses. • -Mineralocorticoid replacement (usually): Fludrocortisone 0. 05 -0. 15 mg daily. • -Androgen replacement (beneficial in women): DHEA (De. Hydro Epi. Androsterone)50 mg/day During stress or illness corticosteroids should be in increase 2 to 3 times.

• Adrenal ct scan in case of primary disease • Brain MRI in case of secondary disease in absence of steroids intake • If pt on steroids therapy for 3 weeks or more , dose should be tapered off gradually
- Slides: 51