Adolescents and Infections How Are They Different and



. Fact Sheet on Demographics: Adolescents and Young Adults.")
. Fact Sheet on Mortality: Adolescents and Young Adults.")
 “inconsistent and unpredictable”")


 Their changing anatomy")















 Stiff neck Nausea Altered mental")




 Meningococcal capsular polysaccharide vaccine (MPSV 4) 2) Meningococcal conjugate vaccines (MCV")








 Gram")
")














 v“Where they’re")




- Slides: 66
Adolescents and Infections: How Are They Different and Why Are They At Risk Lawrence J. D’Angelo, MD, NPH Professor of Pediatrics, Medicine, Epidemiology, and Prevention and Community Health George Washington University Division Chief, Adolescent and Young Adult Medicine Children’s National Medical Center
Adolescents and Infections: How are they different and why are they at risk? Learning Objectives 1) Understand some of the basic physiologic differences in adolescents and how these differences predispose to infections; 2) Understand social and psychological issues that predispose to infections; 3) Review some of the infections unique to adolescents 4) Understand the preventive measures that can protect teens.
ADOLESCENT POPULATION OF THE UNITED STATES 1980 - 2010
National Adolescent Health Information Center. (2008). Fact Sheet on Demographics: Adolescents and Young Adults. San Francisco, CA
National Adolescent Health Information Center. (2006). Fact Sheet on Mortality: Adolescents and Young Adults. San Francisco, CA
Adolescence Is……………. “a time of storm and stress” (G. Stanley Hall) “inconsistent and unpredictable” (Anna Freud) “an abstraction limited by the boundaries of the minority group concept” (Eugene Brody) “the confluence of all the great physical and psychosocial changes” (A Really Great Adolescent Medicine specialist) “the time your tail falls off” (Kermit the Frog)
How Are Adolescents Defined? Law - “Minors” are < 18 years of age NIH - 12 to 18 years NCHS/CDC - 10 to 20 years AAP - 12 to 21 years WHO - 10 to 25 years (youth) Erikson - “Achievement of an identity” ATN - 12 to 25 years
Unfortunately, Society Perceive the Health Problems of Adolescents as: SEX DRUGS ROCK ‘N ROLL No one thinks about infections in adolescents, accept in these contexts
What puts adolescents “at risk” of inctions and infectious diseases? 1) Their changing anatomy and physiology 2) Their changing social milieu 3) Their changing behavior
What specific “anatomic and physiologic” aspects can increase infectious risk in adolescents? • An ever changing and “inexperienced” immune system • An Immature genital tract • An immature skeletal system • An immature “central nervous system”
Case Presentation #1 14 yo F with acute onset of lower and epigastric abdominal pain Nausea, 8 episodes of vomiting, occasionally bloodtinged but now bilious ROSS +fever 101. 6, decreased PO intake, +sore throat, +headache for the past 24 hours +menses for last 4 days with cramps DENIES URI sxs, cough, CP, diarrhea, dysuria or hematuria, myalgias, arthralgias, rash DENIES new foods, sexual activity, drug/alcohol use, recent insect bites
Case #1 - Continued PMHx: scoliosis Surg Hx: posterior spinal fusion Oct 07 FHx: non contributory Allergies: PCN Meds: none Social: Lives in New Mexico, here on school trip
Case #1 – Physical Exam T 39. 3 P 132 R 31 BP 69/29 GEN: uncomfortable, wretching HEENT: NC/AT, PERRL, EOMI, conjunctival injection TMs intact, MM tacky, erythematous lips Neck: supple, no LAD CV: Tachycardic with gallop cadence, II/VI SEM along LSB, cap refill 2 seconds, pulses 2+ Lungs: Clear to Auscultation Abd: Scaphoid, diffusely tender to palpation, no rebound, BS+ Skin: “flushed”, diffusely erythematous without petecchiae Ext: NL ROM, no swelling, no edema Neuro: Alert, Oriented, CNs intact, 5/5 strength, NL sensation, 2+ DTR, NL coordination, NL gait GU / bimanual: Blood in vaginal vault; + CMT + adnexal tenderness
Case #1 – Laboratory Findings CBC – Hgb 13. 9 gm/dl; Hct 39. 7%; WBC 18, 900/mm 3 Plt CT 83, 500 Sed Rate – 67 mm/hr CMP – Na 139; K 4. 2; Cl 104; CO 2 ; BUN 29; Cr 3. 4; AST 48; ALT 119; TBili 0. 8; Alk Phos 114; CA 8. 9 CPK 6426 Lipase – 67; Amylase 89
Case #1 – Question What additional “piece of the history” will you now seek? A) B) C) D) Do you have pets? Have you received the “meningitis shot”? What type of catamenial (feminine hygiene) products do you use? Have you had any tick bites?
Case #1 – My Answer What additional “piece of the history” will you now seek? A) B) C) D) Do you have pets? Have you received the “meningitis shot”? What type of catamenial (feminine hygiene) products do you use? Have you had any tick bites?
Staphylococcal Toxic Shock Syndrome: Definition 5/6 Criteria = Probable *6/6 Criteria = Definite u u u Fever >38. 9 C (102 F) Rash: Diffuse macular erythroderma **Desquamation – late (1 -2 weeks later) Hypotension - systolic <90 mm Hg adult or <5% for age or orthostasis Multi-organ system involvement- at least 3 of: -1. Mucus membrane hyperemia : conjunctival, oropharyngeal or vaginal -2. Renal: BUN, Cr >2 X nl OR >5 WBC/hpf on urinalysis -3. Hepatic: bili, AST, or ALT >2 X nl -4. Gastrointestinal: vomiting/diarrhea at onset -5. Hematologic: Platelets <100 K -6. CNS: Disorientation, altered LOC without focal neuro signs in absence of fever, hypotens 7. Muscular: severe myalgia, CPK >2 X nl u Exclusion of other causes: -Blood, throat, CSF cultures negative - blood MAY be positive for Staph aureus (only 5% of time) -Consider RMSF, Leptospirosis, Measles
TSS: Macular Erythroderm
Why Teens and Toxic Shock Syndrome? Fact: In the 1980 TSS “outbreak”, 36% of the cases occurred in individuals ages 15 -19 years Reasons? 1) While 95% of adults have antibody to TSST-1, only 50% of 13 year olds do. (Immature Immune System) 2) The endocervix of most teens ages 12 -15 years is still lined with columnar epithelial cells and these persist in many adolescents until age 20 years. (Immature Genital Tract) 3) Young adolescents are less skilled at using intravaginal catamenial products. (Less “Life Experience”) 4) Relatively lighter menstrual flow means fewer tampon changes and overnight use is often greater than 8 hours.
Other infections where stage of adolescent development is a “cofactor” Infectious Mononucleosis All STIs and Pelvic Inflammatory Disease (PID) in particular Osteomyelitis Sinusitis Lemierre’s Syndrome
Case Presentation #2 18 yo college freshman with 12 hours of fever (103. 8 F), sore throat, weakness, neck pain and headache. Seen in student health center and transferred to your emergency room ROSS; Patient noted macular papular eruption shortly before going to student health center Hx: No significant history; has a “girlfriend” but denies sexual activity; no animal contact; no history of tick bite
Case #2 – Physical Exam T 38. 7 P 118 R 31 BP 100/59 GEN: uncomfortable, aggitated HEENT: Photophobia, PERRL, EOMI, conjunctival injection; TMs intact, MM tacky, erythematous lips Neck: Moderately stiff, + Brudzinski, + Kerig CV: Tachycardic, with no murmurs or gallop Lungs: Clear to Auscultation Abd: Scaphoid, non-tender to palpation, BS+ Skin: Red papular lesions on lower extremities with surrounding petecchiae Ext: NL ROM, no swelling, no edema Neuro: Lethargic, Oriented, CNs intact, 5/5 strength, NL sensation, 2+ DTR,
Case #2 – Question Based on the history and findings to date, what test do you want to do first? A) B) C) D) CBC and platelet count Complete metabolic panel CT scan Lumbar Puncture
Case #2 –My Answer Based on the history and findings to date, what test do you want to do first? A) B) C) D) CBC and platelet count Complete metabolic panel CT scan Lumbar Puncture
Meningococcal Disease 1 Meningitis Fever and headache (flu-like symptoms) Stiff neck Nausea Altered mental status Seizures Occurs in ~30% of cases; 3% to 10% fatality rate © The Meningitis Trust. www. meningitis-trust. org. Meningococcemia Rash Vascular damage Disseminated intravascular coagulation Multi-organ failure Shock Death can occur in 24 hours Occurs in 10% to 30% of cases; up to 40% fatality rate Reference: 1. Munford RS. Meningococcal infections. In: Braunwald E, Fauci AS, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine. 15 th ed. New York, NY: Mc. Graw-Hill Professional Publishing; 2001: 927 -931.
Meningococcal Disease: Adolescents and Young Adults at Risk a b ABCs = Active Bacterial Core Surveillance System. a NETSS = National Electronic Telecommunications System for Surveillance. b Rate of invasive disease in 17 - to 20 -year-olds is twice that of US population 1 Carriage rates suggest that adolescents, young adults are most common source of transmission to the community 2 Majority of cases are potentially vaccine-preventable 3 References: 1. CDC. Meningococcal disease. In: Atkinson W, Wolfe S, Hamborsky J, Mc. Intyre L, eds. Epidemiology and Prevention of Vaccine-Preventable Diseases. (The Pink Book). 11 th ed. Washington DC: Public Health Foundation; 2009: 177 -188. 2. Pelton SI. Pediatr Infect Dis J. 2009; 28(4): 329 -332. 3. Harrison LH, et al. JAMA. 2001; 286(6): 694 -699.
Age-Specific Fatalities From Meningococcal Disease, US, 1997– 2002 CDC. National Vital Statistics Reports. 2003; 52: 30; 2004; 53: 29.
Rates of Meningococcal Disease in Young Adults, US, 9/1/98 - 6/30/99 Groups # Cases Population Rates/100, 000 Centers for Disease Control and Prevention and control of meningococcal disease and Meningococcal disease and college students: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR. 2000; 49(RR-7); 120. Updated in: Bruce MG et al [CDC]. Risk Factors for Meningococcal Disease in College Students. JAMA. 2001; 286: 688 -693
Common factors of Adolescent “Social Milieu” that are “Risk Factors” for Meningococcal Disease Risk Factor Relative Risk Dormitory living 10. 7 Cigarette smoking 7. 8 Bar patronage 16. 7 Alcohol consumption (>15 drinks*/week) 3. 8 *With one drink defined as 2 oz (60 m. L) of liquor, 5 oz of wine, or 12 oz of beer Bruyere HJ, Culver B. Pharm Times. 1998; 90; Mc. Gee ZA, Baringer R. In: Mandell GL, Douglas RG Jr, Bennett JE, eds. Principles and Practices of Infectious Diseases. 3 rd Edition. New York, NY, Churchill Livingston; Imrey PB, et al. Am J Epidemiol. 1996; 143: 624; Imrey PB, et al. J Clin Microbiol. 1995; 33: 3133
Meningococcal Vaccines 1) Meningococcal capsular polysaccharide vaccine (MPSV 4) 2) Meningococcal conjugate vaccines (MCV 4) (Menactra and Menveo) Preferred vaccine, replacing MPSV 4 for most patients Provides longer lasting immunity than MPSV 4 Provides herd immunity by reducing nasopharyngeal carriage Recent data showed breakthrough cases and titer decreases Later vaccine may cause quicker response with higher titer No conclusive data on “boostering” with vaccine not originally administered as primary
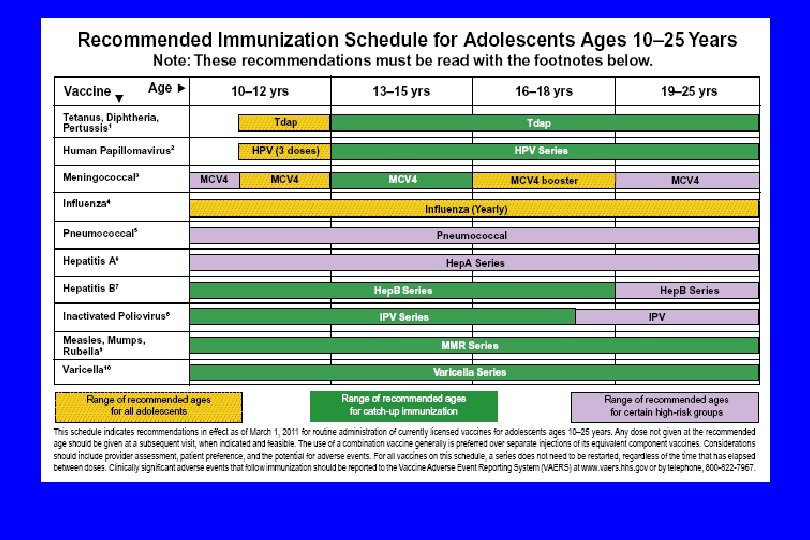
ACIP Recommendations for Use of Meningococcal Conjugate Vaccine in Adolescents at their 11 - to 12 -year health-care visit, with a booster dose at 16 years of age 1 If primary dose not given until 13 -15 years of age, then booster dose at 1618 years of age 1 Adolescents 11 -18 years of age who were not vaccinated previously 2 Previously unvaccinated college freshmen living in dormitories 3 Adolescents 11 -18 years of age with human immuno-deficiency virus (HIV) infection 1 Two-dose primary series, 2 months apart Booster doses: same as for other adolescents Reference: 1. CDC. MMWR. 2011; 60(3): 72 -76. 2. CDC. MMWR. 2007; 56(31): 794 -795. 3. CDC. MMWR. 2005; 54(RR-7): 1 -21.
ACIP: Meningococcal Vaccination of High-risk Persons 2 -55 Years of Age 1 Persons with persistent complement component deficiencies or functional or anatomic asplenia Primary series: 2 doses, 2 months apart Booster dose every 5 years (give first booster at earliest opportunity if a 1 -dose primary series was given) Persons at prolonged increased risk for exposure Microbiologists working with N meningitidis; travelers to countries where meningococcal disease is hyperendemic or epidemic If first vaccinated at 2 -6 years of age, revaccinate after 3 years If first vaccinated at 7 years of age or older, revaccinate after 5 years if the person remains at increased risk Reference: 1. CDC. MMWR. 2011; 60(3): 72 -76.
Other infections where the “Social Milieu” is a “risk factor” for adolescents Pertussis Influenza Mycoplasma pneumonia Hepatitis A Cellulitis, skin eruptions (herpes, MRSA)
Reported Cases of Pertussis Are Highest Among Adolescents and Adults 1990 -19931 1994 -19961 1997 -20002 2001 -20033 2004 -20053 2006 -20093 Average Cases Per Year 9000 8000 7000 6000 5000 4000 3000 2000 1000 0 <1 yr 1 -4 yrs 5 -9 yrs 10 -19 yrs 20+ yrs Age Group References: 1. Güris D, et al. Clin Infect Dis. 1999; 28(6): 1230 -1237. 2. CDC. MMWR. 2002; 51(4): 73 -76. 3. CDC. Pertussis Surveillance Reports, 2001 -2009.
Case Presentation #3 17 yo F with 3 days of increasing right upper quadrant pain Nausea with 2 episodes of vomiting; preceded by lower abdominal pain 5 days prior ROSS Decreased PO intake for past 24 hours; LMP concluded 1 day prior to onset of symptoms DENIES diarrhea, fatty food intolerance, dysuria or hematuria DENIES new foods, drug use, or alcohol use
Case #3 - Continued PMHx: History of “gonorrhea” 10 months ago, rxed with “pills” FHx: no history of gall bladder disease Allergies: Shellfish, nuts Meds: Oral Contraceptives Social: Sexually active (sexual debut age 14), 2 partners in past 6 months, 5 lifetime
Case #3 – Physical Exam T 36. 7 P 78 R 14 BP 110/66 BMI 31 GEN: No distress HEENT: Unremarkable Neck: Supple; no abnormalities CV: Normal rate and rhythm with no murmurs or gallop Lungs: Clear to Auscultation Abd: Scaphoid, Moderate RUQ tenderness worse with inspiration, neither liver or spleen palpated; BS+ Pelvic: No ext lesions; moderate white dc from os; minimal CMT and “ 1+” adnexal tenderness Skin: No rashes or lesions Ext: NL ROM, no swelling, no edema Neuro: Alert, Oriented
Case #3 – Laboratory Findings CBC – Hgb 13. 9 gm/dl; Hct 39. 7%; WBC 6900/mm 3 Sed Rate – 67 mm/hr CMP – Na 139; K 4. 2; Cl 104; CO 2 ; BUN 19; Cr 1. 0; AST 48; ALT 119; TBili 0. 8; Alk Phos 114; CA 8. 9 Lipase – 67; Amylase 89 Wet Prep – p. H 5. 5, + clue cells, + “wiff” test, moderate WBCs
Case #3 – Question The most likely etiology of this illness is: A) Gram negative bacteria (Gall Bladder Disease) B) Neisseria Gonorrhoea C) Chlamydia trachomatis D) Streptococcus pneumoniae
Case #3 – My Answer The most likely etiology of this illness is: A) Gram negative bacteria (Gall Bladder Disease) B) Neisseria Gonorrhoea C) Chlamydia trachomatis* D) Streptococcus pneumoniae * Causing Fitz-Hugh Curtis Syndrome
Chlamydia—Rates by State, United States and Outlying Areas, 2009 327 309 305 272 303 252 Guam 352 375 472 457 369 386 399 400 405 346 313 305 225 469 375 413 478 341 753 468 420 311 438 199 503 398 595 626 Puerto Rico 185 556 191 160 297 344 346 276 540 422 1, 107 445 478 803 435 VT NH MA RI CT NJ DE MD DC 185 411 Virgin Islands 444 398 Rate per 100, 000 population <300. 0 (n = 10) 300. 1– 400. 0 (n = 21) >400. 0 (n = 23) NOTE: The total rate of chlamydia for the United States and outlying areas (Guam, Puerto Rico, and Virgin Islands) was 406. 3 per 100, 000 population.
Chlamydia—Rates by Age and Sex, United States, 2009 Men 3, 800 Rate (per 100, 000 population) 3, 040 2, 280 1, 520 760 0 13. 8 760 Age 0 10– 14 127. 9 Women 1, 520 15– 19 735. 5 1, 234. 0 30– 34 286. 0 141. 3 81. 9 36. 0 11. 0 2. 9 219. 8 511. 7 35– 39 40– 44 205. 8 88. 4 45– 54 32. 0 55– 64 9. 1 65+ Total 3, 800 3, 273. 9 25– 29 573. 3 3, 040 3, 329. 3 20– 24 1, 120. 6 2, 280 2. 1 593. 4
Gonorrhea—Rates by State, United States and Outlying Areas, 2009 34. 9 8. 3 23. 5 29. 4 7. 2 Guam 33. 5 44. 1 92. 4 42. 8 63. 2 77. 2 12. 5 50. 0 81. 4 55. 2 139. 2 154. 7 57. 2 54. 5 89. 4 128. 3 107. 2 89. 6 109. 8 127. 5 156. 2 246. 4 160. 8 120. 4 144. 3 49. 0 87. 2 147. 0 13. 9 66. 4 VT NH MA RI CT NJ DE MD DC 10. 9 204. 0 Puerto Rico 5. 8 26. 2 100. 3 150. 4 185. 7 141. 3 113. 9 Virgin Islands 104. 7 8. 0 8. 6 30. 4 30. 6 73. 1 54. 8 111. 2 113. 5 432. 7 Rate per 100, 000 population <19. 0 (n = 8) 19. 1– 100. 0 (n = 24) >100. 0 (n = 22) NOTE: The total rate of gonorrhea for the United States and outlying areas (Guam, Puerto Rico, and Virgin Islands) was 97. 8 per 100, 000 population.
Gonorrhea—Rates by Age and Sex, United States, 2009 Men 750 Rate (per 100, 000 population) 600 450 300 150 0 5. 0 Age 10– 14 0 150 Women 300 568. 8 20– 24 407. 5 555. 3 25– 29 238. 9 229. 4 30– 34 145. 0 60. 8 40– 44 33. 6 11. 4 2. 7 92. 2 106. 2 35– 39 85. 6 47. 6 22. 9 45– 54 8. 7 55– 64 2. 1 65+ 0. 5 Total 600 25. 3 15– 19 250. 0 450 105. 7 750
Percentage of High School Students Who Ever Had Sexual Intercourse, by Sex* and Race/Ethnicity, † 2011 *M>F †B > H > W National Youth Risk Behavior Survey, 2011
Percentage of High School Students Who Ever Had Sexual Intercourse, 1991 – 2011† † Decreased 1991– 2001, no change 2001 -2011, p < 0. 05. National Youth Risk Behavior Surveys, 1991– 2011
Percentage of High School Students Who Had Sexual Intercourse for the First Time Before Age 13 Years, 1991 – 2011* * Decreased 1991– 2005, no change 2005 -2011, p < 0. 05. National Youth Risk Behavior Surveys, 1991– 2011
Percentage of High School Students Who Had Sexual Intercourse with Four or More Persons During Their Life, 1991 – 2011* * Decreased 1991– 2001, no change 2001 -2011, p < 0. 05. National Youth Risk Behavior Surveys, 1991– 2011
Range and Median Percentage of High School Students Who Had Sexual Intercourse with Four or More Persons During Their Life, Across 38 States and 21 Cities, 2011 State and Local Youth Risk Behavior Surveys, 2011
Percentage of “Currently Sexually Active” Students who have had 4 or more Sexual Partners by grade Grade 9 th 10 th 11 th 12 th % Female 18. 0 31. 8 41. 5 56. 7 % Male 22. 2 29. 4 42. 0 48. 3 Total 20. 1 30. 6 41. 8 52. 6
Percentage of High School Students Who Used a Condom During Last Sexual Intercourse, * by Sex† and Race/Ethnicity, § 2011 * Among the 33. 7% of students nationwide who were currently sexually active. †M>F § B>H National Youth Risk Behavior Survey, 2011
Percentage of High School Students Who Used a Condom During Last Sexual Intercourse, * 1991 – 2007 * Among students who had sexual intercourse with at least one person during the 3 months before the survey. 1 Increased 1991 -2003, no change 2003 -2007, p <. 05 National Youth Risk Behavior Surveys, 1991 – 2007
Percentage of High School Students Who Were Ever Taught in School about AIDS or HIV Infection, 1991 – 2007 1 Increased 1991 -1997, decreased 1997 -2007, p <. 05 National Youth Risk Behavior Surveys, 1991 – 2007
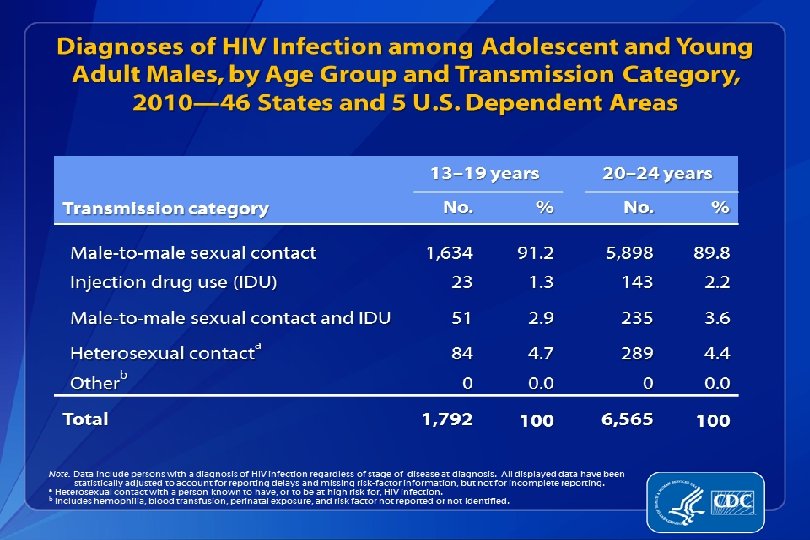
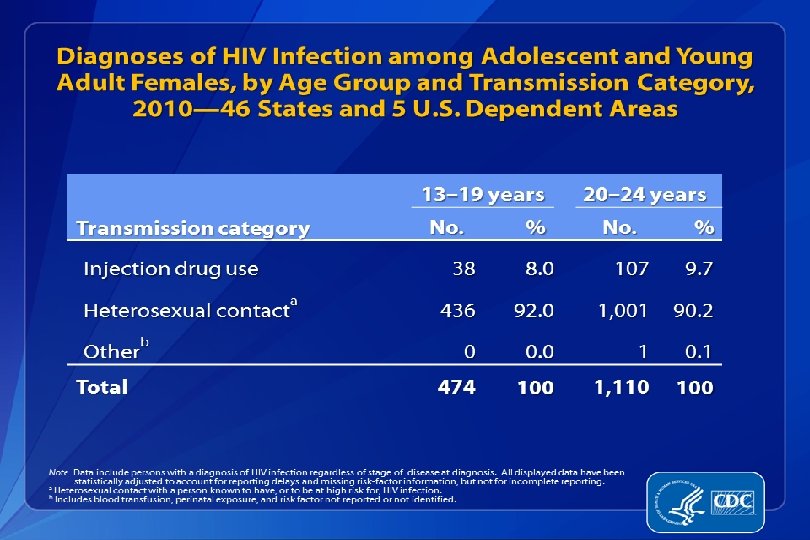
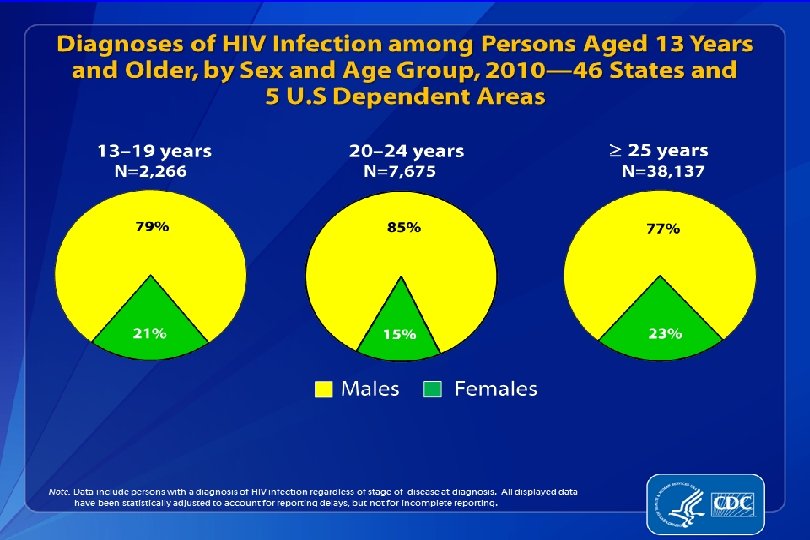
What Are Adolescents’ Risk Factors for HIV Infection and other STDs? • Traditional risk factors (Lack of Barrier Protection, MSM, Injection drugs, Other high risk sexual practices) • “Multiple” and “Older” sexual partners • Non-injection drug use • Co-existent sexually transmitted disease(s) • Resident in community with high incidence of HIV
What Puts Adolescents at Risk of Infections? v. Who they Are (Biology) v“Where they’re At” (Sociology) v. What they Do (Psychology)
What Can Health Care Providers Do to Lower the Risks for Adolescents? Biologic Risks – Anticipatory guidance; Education advocacy Social Milieu Risks – Immunization; Health advocacy Behavioral Risks – Endorse family values; Encourage “connectedness”; Encourage communication on sexual matters; Anticipatory guidance; Community advocacy
An Anticipatory Guidance Checklist For Biologic Risks üAppropriate Tampon Use üAppropriate Barrier Protection for Sexually Active Teens üAppropriate education about skeletal development
Anticipatory Guidance for Social Interaction Risks ü Provide Appropriate Immunization ü Emphasize the value of Handwashing ü Encourage Protective Hygiene ü Limit Exposure to High Risk Environments
Anticipatory Guidance for Behavioral Risks üEncourage teen-parent communication üEmphasize the importance of family and family values üEncourage barrier protection use üEmphasize the risks of STIs üEncourage HPV immunization