ADNEXAL MASSES N PREGNANCY DR EREN AKBABA School

ADNEXAL MASSES İN PREGNANCY DR. EREN AKBABA School of Medicine, Muğla Sıtkı Koçman University

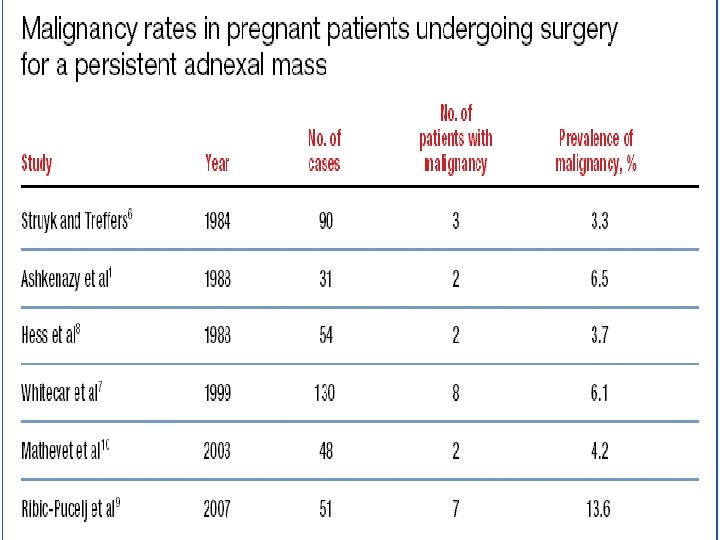
ADNEXAL MASSES İN PREGNANCY • Since the introduction of routine obstetric ultrasound examination adnexal masses are diagnosed more frequently than before. • The incidence of adnexal masses during pregnancy : 0, 2 -2% • With a 1 -6% malignancy rate, the vast majority of these masses are benign (Hoover and Jenkins, 2011; Leiserowitz, 2006; Runowicz and Brewer, 2014; Telischak et al. , 2008) • Of all malignant tumours of the ovary: %10 are metastases of other organs, mainly gastrointestinal or breast tumours. (Amant et al. , 2010).

ADNEXAL MASSES İN PREGNANCY • Malignancy is not the only risk associated with adnexal mass. Masses that persist into the second trimester are at risk for torsion, rupture, or labor obstruction. • Torsion: %1 -22 • Rupture: %0 -9 • Obstruction of labor: %2 -17 Leiserowitz G. 2006, Schmeler K. 2005

Histopathology of adnexal masses removed in pregnancy. Benign ovarian masses account for the majority of masses diagnosed in pregnancy, most of which are mature cystic teratomas, corpus luteum cysts, and cystadenomas. Clinical Obstetrics & Gynecology. , March 2015.

ADNEXAL MASSES IN PREGNANCY: BASKENT UNIVERSITY EXPERIENCE Polat DURSUN, Filiz F. YANIK, Esra CABUK, Hulusi B. ZEYNELOGLU, Berk BILDACI, Esra KUSCU, Ali AYHAN Turk Soc Obstet Gynecol 2011 Histopathologic type, % Dermoid cyst %22, 2 Serous cystadenom %14. 8 Mucinosis cyst %14. 8 Endometrioma %11. 1 Morgagni cyst %11. 1 Follicle cyst Siderophagic cyst Fibroma Thecomata %11. 1 %7. 4 %3. 7

Ovarian cancer during pregnancy Kazım Gezginç, Rengin Karataylı, Fatma Yazıcı, Ali Acar, Çetin Çelik, Metin Çapar Department of Obstetrics and Gynecology, Meram Medical School, Selçuk University, Konya, Turkey March 17 , Int J Gynaecol Obstet. 2011 • Ovarian cancer insidance : 0. 75 per 1000 deliveries. • Median age of diagnosis: 26. 5

Frequency of malignant and benign ovarian masses during pregnancy Archives of Gynecology and Obstetrics 2014(Ahmed Nazer , Canada) Ovarian mass Per 10, 000 deliveries Total malignant ovarian masses 0. 12 Malignant neoplasm of ovary 0. 11 Fallopian tube 0. 001 Uterine adnexa 0. 001 Other specified sites of uterine adnexa 0. 001 Neoplasm of uncertain behavior of ovary (LMP) 0. 11 Benign adnexal mass 25 Ovarian mass in pregnancy 25

ADNEXAL MASSES İN PREGNANCY • Ovarian cancer is the second most common gynecological malignancy complicating pregnancy after cervical cancer. • In the premenopausal population adnexal masses found on examination are often incidentally, mostly benign and of little clinical significance. • One has to make a distinction between an ovarian mass and a non-ovarian mass • An adnexal mass in pregnancy can be complicated by torsion, rupture, or bleeding/infection, or labor obstruction. Arch Gynecol Obstet Al-Halal H, Kezouh A, Abenhaim HA (2013)

Imaging • Ultrasound is the most common diagnostic tool it is safe to use. Morphology is the most important determinant in distinguishing benign masses from malignancies. • Color Doppler imaging has been shown to significantly improve the ability to distinguish benign from malignant masses. The Doppler criteria show that malignant tumors will generally have lower blood flow impedance and higher blood flow velocity; these findings can also be seen in inflammatory lesions (Usui et al. , 2000; Leiserowitz, 2006. , Telischak et al. , 2008; Hoover and Jenkins, 2011 Cohen. Herriou et al. , 2013; Levine, 2014).
 can be safely used during the second")
Imaging • MRI Magnetic resonance imaging (MRI) can be safely used during the second and third trimester, although the use of gadolinium-based contrast material should be avoided because fetal safety has not been established. • MRI is particularly useful in making 3 -dimensional images, distinguishing between different morphologic characteristics like bone of muscular tissue, e. g. leiomyomas, endometriomas and complex masses with solid compounds. (Runowicz and Brewer, 2004; Leiserowitz, 2006; Telischak et al. , 2008).

ADNEXAL MASSES İN PREGNANCY • Potential non-ovarian masses include pedunculated fibroids, hydrosalpinx or paraovarian cysts. • Fibroids appear as heterogeneous, solid masses • Hydrosalpinx present more as a tubular shaped structure. A hydrosalpinx can be difficult to distinguish from a malignant neoplasm due to the presence of nodules and thick endosalpingeal folds. • Para-ovarian cysts are a common incidental finding and do not have any clinical significance. (Chiang and Levine, 2004; Glanc et al. , 2008; Levine, 2014)

Benign adnexal masses discovered during early pregnancy sonography with their morphologic appearance on ultrasound. (Giuntoli et al. , 2006; Glanc et al. , 2008; Hoover et al. , 2011; Leiserowitz, 2006; Parsons, 2001; Telischak et al. , 2008; Whitecar et al. , 1999). Type of mass Sonographic features 1. Functional cyst – Corpus luteum – Widespread appearance; ‘Ring of fire’ with Doppler. – Follicular cyst – Mainly simple cyst < 10 cm, sometimes with debris. – Haemorrhagic cyst – Fine interdigitating lines (fishnet); solid compounds with concave outer lining. No flow with Doppler 2. Dermoid cyst – Rokitansky nodule; a hyperechoic nodule with acoustic shadowing in a background of low-level echoes. – ‘Tip of the iceberg’ phenomenon, where a highly echogenic cyst, contents of sebum and hair, causes posterior attenuation of sound. – ‘Dermoid mesh’, multiple interdigitating lines and dots which are seen when hair is floting in sebum.

Type of mass Sonographic features 3. Serous cystadenoma – Large simple cyst > 5 cm. – Thin septations or papillary formations. 4. Mucinous cystadenoma – > 5 cm in diameter. – Multiple septae. – Heterogenic aspect 5. Endometrioma – Round thick regular wall; diffuse homogenous low-level internal echoes (chocolate cyst). – Calcifications with acoustic shadowing. 6. Leiomyomas – Not attached to the ovary. – Round regular wall. – When outgrowing the blood supply central necrosis may be seen. 7. Paraovarian cyst – 1 -2 cm simple cysts. – Not attached to the ovary.

Ultrasound/diagnostic features of adnexal mass

KORPUS LUTEUM

DİSGERMİNOM
 müsinöz tm(USG), seröz kistadenokarsinom.")
Sırasıyla müsinöz kistadenom, LMP(Low malignant potantial) müsinöz tm(USG), seröz kistadenokarsinom.

ENDOMETRİOMA

Pregnancy-associated changes of ovarian masses Endometriomas can have a strongly changed appearance during pregnancy because of decidualized walls due to high levels of progesterone in pregnancy. A previous history of symptoms of endometriosis can be indicative. Glanc etal. , 2008; Patel et al. , 1999
 with characteristic homogenous echogenicity")
Benign adnexal masses. Ultrasound images of an ovarian endometrioma (A) with characteristic homogenous echogenicity in a cystic mass, and a mature cystic teratoma (B) with heterogenous echogenicity and calcifications, both diagnosed in pregnancy. Images courtesy of Dr Bryann Bromley.

Malignancy. Ultrasound image of an endometrioid ovarian adenocarcinoma with papillary projections diagnosed . during pregnancy. Image courtesy of Dr. Bryann Bromley.
")
Seröz kistadenom(USG)

MÜSİNÖZ KİSTADENOM

HEMORAJİK KİST

MULTİLOKULE THECA LUTEİN KİSTİ
 simple rules. Adjusted from Timmerman et al. , 2010.")
IOTA (International Ovarian Tumor Analysis) simple rules. Adjusted from Timmerman et al. , 2010. Ultrasonic features For predicting a malignant tumor (M features) M 1 – Irregular solid tumor M 2 – Presence of ascites M 3 – At least four papillary structures M 4 – Irregular multilocular solid tumor with largest diameter ≥ 100 mm M 5 – Very strong blood flow (colour score 4) For predicting a benign tumor (B features) B 1 – Unilocular B 2 – Presence of solid components, of which largest solid component has largest diameter < 7 mm B 3 – Presence of acoustic shadows B 4 – Smooth multilocular tumor with largest diameter < 100 mm B 5 – No blood flow (colour score 1) Rule 1: If one or more M features are present in absence of B feature, mass is classified as malignant. Rule 2: If one or more B features are present in absence of M feature, mass is classified as benign. Rule 3: If both M features and B features are present, or if no B or M features are present, result is inconclusive and second stage test is recommended.

Pregnancy-associated changes of ovarian masses • When a pregnant patient presents with a symptomatic adnexal mass early in pregnancy, an ectopic pregnancy must always be ruled out since an undiagnosed ectopic pregnancy may have a potentially lethal outcome(. Runowicz and Brewer, 2014). • Other pregnancy associated masses are benign and typically present as bilateral cysts, except for luteomas who present as unilocular solid masses . (Leiserowitz, 2006; Hoover and Jenkins, 2011; Hoffman, 2014).

Pregnancy-associated changes of ovarian masses • The most common pregnancy-associated ovarian masses are functional cysts like the corpus luteum of pregnancy and theca-lutein cysts. Most of these cysts will resolve after the first 14 -16 weeks of gestation but some, like theca lutein cysts, can persist until after delivery. Masses still present after 16 weeks of gestation are predominantly nonfunctional. (Chiang and Levine, 2004; Leiserowitz, 2006; Glanc et al. , 2008; Hoffman, 2014).

Tumour markers • The reliability of tumour markers in the diagnosis and characterization of tumours during pregnancy is often debated. During pregnancy elevations of tumour markers are mostly associated with the normal physiologic changes of pregnancy and presence of obstetric complications(miscarriage, preeclampsia, HELLP) (Han et al. , 2012)
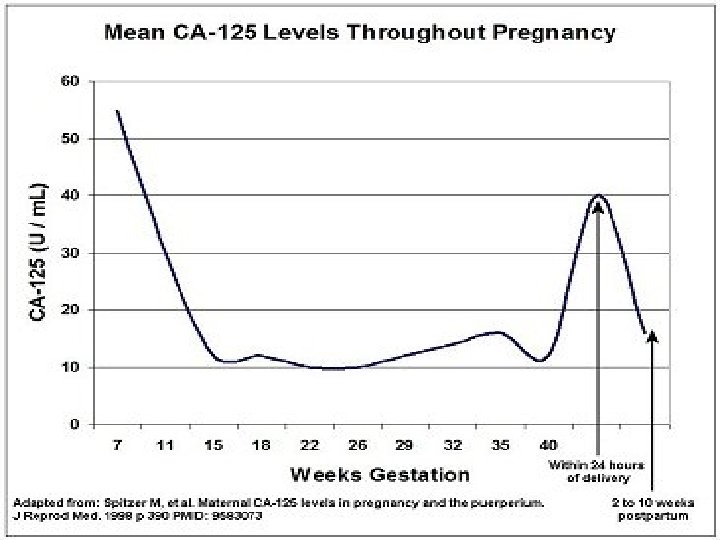

Tumour markers • When an ovarian mass is diagnosed in pregnancy, CA-125 levels may help to distinguish between a benign or malign lesion and can be used to evaluate treatment(Giuntoli et al. , 2006; Leiserowitz, 2006). • However, decidua- and amnion cells also produce CA-125 resulting in higher CA-125 levels during pregnancyespecially in the first and third trimester (respectively because of trophoblast invasion and detachment of the placenta). Tumour markers associated with germ cell tumours (e. g. AFP and b-h. CG) and granulosa cell tumours • (Inhibine B and AMH) can also be elevated in normal pregnancy and can therefore only be used as follow-up . (Leiserowitz, 2006).
 • The clinician needs to make a careful")
Surgery during pregnancy (open vs laparoscopy) • The clinician needs to make a careful decision when to operate, 1. Too early (risk of miscarriage and loss of luteal function before the fourth month of pregnancy) 2. Too late (complications as torsion, rupture or bleeding, progression in case of malignancy, premature labour) can affect the patient and fetus.

Surgery should be considered in 3 general groups 1. Acut symtomatic with signs and symptoms of ovarian torsion or hemodynamically unstable due to cyst rupture. 2. Suspicious for malignancy 3. Larger adnexal masses that are at higher risk of the above complications. AJOG 2011
 • A midline laparotomy with minimal uterine manipulation")
Surgery during pregnancy (open vs laparoscopy) • A midline laparotomy with minimal uterine manipulation is preferred in case of an open approach. • Laparoscopy : A guideline from the The Society of American Gastrointestinal and Endoscopic Surgeons, published in 2008, the following recommendations specific to performing laparoscopy during pregnancy. Yumi H. Surg Endosc 2008
 Laparoscopy is safe and feasible when specific guidelines")
Surgery during pregnancy (open vs laparoscopy) Laparoscopy is safe and feasible when specific guidelines are followed. 1. Laparoscopic management nonemergent cases should be optimally scheduled between 16 and 20 weeks of gestation, based on the time allowed for spontaneous resolution, the optimized visualisation of the mass in contrast with the enlarged uterus, and the decreased ratio of premature labour.
 2. Important to consider is the position of")
Surgery during pregnancy (open vs laparoscopy) 2. Important to consider is the position of the patient to avoid hypovolemia, hypotension and hypoxemia by the slowly change to Trendelenburg allowing only mild inclination, and from 20 weeks of gestation onwards, using the left lateral tilt position. 3. The preferred method for primary trocar insertion should be the open laparoscopy and supra-umbilical port placement to limit the possibility of uterine perforation by insertion of a Veress needle. (Hassan technique). Veress needle is not contraindicated. The surgeon may consider using the veress needle in conjunction with ultrasound guidance.
 4. Trochars should be placed at least 6")
Surgery during pregnancy (open vs laparoscopy) 4. Trochars should be placed at least 6 cm above the fundus or in the left upper quadrant. 5. Intraoperativ CO 2 monitoring by capnography should be used. 6. Intraoperative abdominal pressure should be maintained less than 15 mm/hg while in trendelenburg position to ensure adequate venous return and uteroplacental sufficiency.
 7. The CO 2 pneumo-peritoneum and CO production")
Surgery during pregnancy (open vs laparoscopy) 7. The CO 2 pneumo-peritoneum and CO production during electrocoagulation do not seem to be detrimental to the fetus when a maximum pressure of 10 -15 mm. Hg, an experienced surgeon and limited operation time is considered (Han et al. , 2014; Ko et al. , 2009). 8. At this time there is no indication for prophylactic tocolysis for antenatal surgery.
 • A guideline from the Society of American")
Surgery during pregnancy (open vs laparoscopy) • A guideline from the Society of American Gastrointestinal and Endoscopic Surgeons, published in 2011, makes the following recommendation: “Laparoscopy is safe and effective treatment in gravid patients``

. Guidelines for Diagnosis, Treatment, and Use of Laparoscopy for Surgical Problems During Pregnancy Prepared by the Society of American Gastrointestinal and Endoscopic Surgeons Guidelines Committee 2007.
 For early stage ovarian cancer, stage I")
Early stage ovarian cancer (borderline and invasive) For early stage ovarian cancer, stage I and II according to the International Federation of Gynecologyand Obstetrics (FIGO), standard surgical procedure consisting of hysterectomy, bilateral adnexectomy, omentectomy, cytology, biopsies and lymphadenectomy should be aimed for. (Prat J and FIGO Committee on Gynecologic Oncology, 2014). For early stage disease, fertility- and pregnancy preserving treatment may be considered. In these selected cases surgery includes removal of the adnex and surgical staging (cytology, peritoneal biopsies, omentectomy and appendectomy in mucinous tumours). (Prat J and FIGO Committee on Gynecologic Oncology, 2014).
 • For invasive epithelial ovarian carcinoma, grade")
Early stage ovarian cancer (borderline and invasive) • For invasive epithelial ovarian carcinoma, grade I and diagnosed at FIGO stage Ia, fertility- and pregnancy preserving management can also be performed(Prat J and FIGO Committee on Gynecologic Oncology, 2014). Restaging after delivery may be considered because of occult extra-ovarian disease, which may not be assessed adequately during pregnancy (Amant et al. , 2010; Morice et al. , 2012). • Non-epithelial tumours (germ-cell and sex-cord stromal tumours), which frequently present as bulky masses, are over 90% diagnosed at FIGO stage Ia and therefore also treated by a resection and surgical staging (Mancari et al. , 2014). • For high grade stage I and any stage II disease, standard adjuvant chemotherapy (carboplatin-paclitaxel) can be considered.
 • In unilateral borderline tumours, a laparoscopic")
Advanced stage ovarian cancer (borderline and invasive) • In unilateral borderline tumours, a laparoscopic procedure without spilling is possible • In case of higher stage disease in borderline tumours, adnexectomy/biopsy during pregnancy is aimed for, followed by completion of surgery after delivery. • Since chemotherapy is not effective for borderline disease and given the indolent nature, an otherwise conservative approach during pregnancy is advised.
 Similar, the performance of complete cytoreductive surgery")
Advanced stage ovarian cancer (borderline and invasive) Similar, the performance of complete cytoreductive surgery for advanced stage invasive (FIGO stage III) ovarian cancer is not possible during pregnancy. In most reported cases of advanced invasive disease, patients chose to terminate pregnancy when diagnosis has been made early in the first trimester of pregnancy (Mancari et al. , 2014).
 • When the patient wants to proceed")
Advanced stage ovarian cancer (borderline and invasive) • When the patient wants to proceed the pregnancy, neoadjuvant chemotherapy (carboplatin and paclitaxel) until fetal maturity and complete cytoreductive surgery after delivery is recommended from midpregnancy onwards (Amant et al. , 2014).

İncidental adnexal masses at caesarean section �İncidence 1/200 -1/400 �Mostly benign �Prefered cyst excision �Frozen section �The incidence of malignant tumors: 0, 21/1000 C/S �%15, 38(2/13)MGHOT �%23, 08(3/13)MEOT �%61, 54(8/13)BOT �All in stage I Lixiao et al , 2011 Schortz et al, 2009

İncidental adnexal masses at caesarean section.

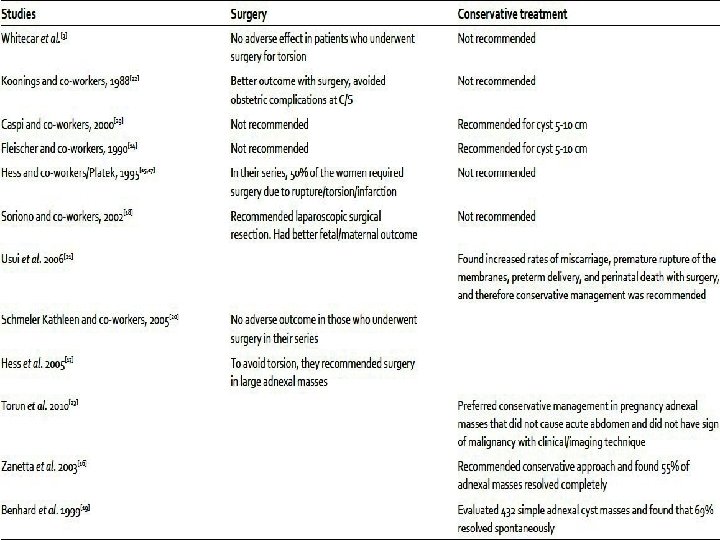
Surgical risk in pregnancy • The traditional management of an adnexal mass in pregnancy has been surgical. However , surgery includes the add risks of fetal loss, preterm contractions, and an increased risk of embolic events. AJOG 2011

Comparison of obstetrical outcomes in delivering women with benign and malignant adnexal masses. Archives of Gynecology and Obstetrics 2014 Controls Benign ovarian masses % % Adjusted ORa (95 % CI) P value Abruptio placentae 1. 09 1. 46 0. 84 (0. 75– 0. 95) 0. 004 2. 79 1. 15 (0. 46– 2. 86) 0. 76 Postpartum hemorrhage 2. 67 2. 10 0. 96 (0. 87– 1. 07) 0. 5 2. 79 0. 26 (0. 09– 0. 75) 0. 012 Infection of amniotic cavity 2. 02 2. 97 1. 02 (0. 94– 1. 11) 0. 60 3. 35 1. 06 (0. 47– 2. 41) 0. 88 Eclampsia 0. 08 0. 10 0. 75 (0. 48– 1. 16) 0. 20 0. 56 3. 10 (0. 43– 22. 31) 0. 26 Preeclampsia 3. 90 6. 38 1. 12 (1. 05– 1. 19) <0. 001 2. 79 0. 40 (0. 16– 0. 98) 0. 04 Blood transfusion 0. 90 1. 62 1. 09 (0. 97– 1. 22) 0. 17 5. 03 1. 20 (0. 51– 2. 85) 0. 67 0. 08 0. 28 1. 65 (1. 25– 2. 19) 0. 005 6. 70 60. 90 (27. 38– 135. 53) <0. 001 0. 22 0. 36 1. 27 (1. 00– 1. 61) 0. 05 2. 23 5. 52 (1. 96– 15. 53) 0. 001 DIC 0. 03 0. 06 0. 87 (0. 48– 1. 61) 0. 66 – – – Maternal death 0. 01 0. 02 1. 16 (0. 43– 3. 13) 0. 76 0. 50 6. 78 (0. 84– 54. 45) 0. 072 Cesarean section 31. 26 77. 50 7. 36 (7. 11– 7. 62) <0. 001 76. 5 5. 92 (4. 17– 8. 41) <0. 001 Forceps delivery 1. 00 0. 26 0. 77 (0. 58– 1. 01) 0. 061 – – – Outcomes Hysterect omy VTE Malignant adnexal masses

Comparison of fetal outcomes in delivering women with benign and malignant adnexal masses Controls Benign ovarian mass % % Adjusted ORa P value 95 % CI 1. 95 2. 37 0. 93 (0. 84– 1. 02) 0. 11 0. 56 0. 20 (0. 03– 1. 42) 0. 11 IUFD (intrauterine 0. 67 fetal demise) 0. 44 0. 92 (0. 75– 1. 14) 0. 50 0. 56 0. 75 (0. 10– 5. 42) 0. 78 7. 39 9. 24 0. 99 (0. 94– 1. 05) 0. 79 18. 4 2. 24 (1. 48– 3. 42) <0. 001 1. 13 1. 17 0. 95 (0. 82– 1. 09) 0. 43 2. 23 0. 83 (0. 29– 2. 38) 0. 74 Outcomes IUGR Preterm birth (<37 weeks) Preterm rupture of membrane Malignant adnexal mass

CHEMOTHERAPY İN PREGNANCY First trimester : Should be avoided secondary to tetratogenic effects on the fetus; Second and Third trimesters : Safe. Growth and functional impairment are of greater concern than fetal malformation. Doll, D. C. , Q. S. Ringenberg, and J. W. Yarbro, Antineoplastic agents and pregnancy. (Paclitaxel and cisplatin chemotherapy) Nevertheless, there should be some side effects in mind(Neutropenia and thrombocytopenia , Spontaneous abortion) � Aviles, A. , et al. , Growth and development of children of mothers treated with chemotherapy during pregnancy: . Am J Hematol, 199. 1 , Marret H et al , 2010

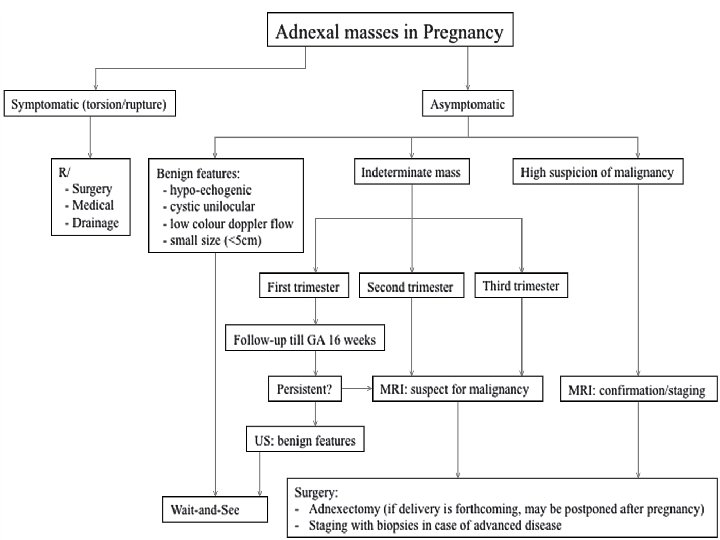
Conclusion • Ovarian cysts or masses during pregnancy should be accurately evaluated to decide the most appropriate treatment option. • Ultrasound and MRI are safe and allow distinguishing between benign and malignant lesions. • A wait-and-see strategy is advised for an ovarian cyst with benign features. • Masses with septa, solid components, papillary or nodules, or when persisting after 16 weeks of pregnancy should be further investigated.

Conclusion • Laparoscopy is safe and feasible, and both maternal and perinatal outcomes are favorable. • If corpus luteum is removed before 8 weeks, then progesterone supplement should be given.

Conclusion • When advanced stage invasive ovarian cancer is diagnosed, termination of pregnancy may be considered in early pregnancy, otherwise chemotherapy can be administered during second and third trimester. • Treatment options should be discussed for each patient individually. • When there is high suspicion of malignancy, a multidisciplinary approach is necessary, and preferably patients should be referred to centres with specialized experience.

DİNLEDİĞİNİZ İÇİN TEŞEKKÜRLER
- Slides: 59