Acuteonchronic liver failure Objective admission and support criteria

Acute-on-chronic liver failure: Objective admission and support criteria in the intensive care unit Assistant Lecturer at Hepatology departement

N O TI D A IN F E G L O I Y M DE I P E G G N I D RA SIS PROGNO IND WH EN ICA TI FO R I ON CU TO ST OP

ACLF : A SEPARATE ENTITY … and which not equals end-stage liver disease !!!
 stated that")
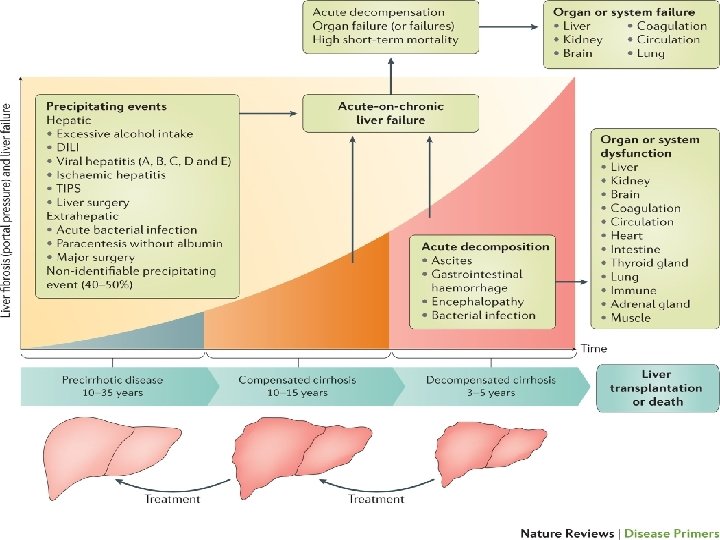
Defination The European Association for the Study of the liver disease (EASL) stated that : Acute-on-chronic liver failure (ACLF) involves any : acute precipitating event, cirrhosis, which deterioration leads to in a patient with acute rapid of hepatic function and extrahepatic Extrahepatic often include renal, cardiovascular, and organ failure. respiratory failures.

Defination World Congress of Gastroenterology: THE SAME DEFINATION + increased mortality within a period of 28 days from onset. .
 admission")
Epidemiology § ACLF is an important syndrome and necessitates intensive care unit (ICU) admission for intensive organ support. § Its prevalence is about 31% in patients presenting with acute decompensation of cirrhosis. § It even carries a greater mortality risk than decompensated cirrhosis, as demonstrated by a recent study showing a 90 -day mortality rate of 34% in patients with ACLF compared to 1. 9% in patients with decompensated cirrhosis.

Need ICU admission

High resistance to ICU admission • Constrained resources. • High resource use and cost. • Preconception of futility.

Avoiding Futility: • Age • Co morbidity • Severity of acute illness • Indication for admission • Prognostic assessment.

Avoiding Futility: prognostic assessment ?

Prognostication in patients with ACLF Different prognostication models: - MELD score. -Child-Turcotte-Pugh score.

CANONIC: Acute On-Chronic liver failure In Cirrhosis 29 Liver Units, 8 European Countries 1343 Hospitalised patients with cirrhosis Develop a definition and scoring system for ACLF.
 score.")
Prognostication in patients with ACLF -Chronic liver failure sequential organ failure assessment (CLIF-SOFA) score. (more accurate at predicting poor outcomes in all patients with ACLF than the older models -Chronic liver failure-consortium organ failure (CLIF-C-OF) score
 score")
Chronic liver failure-sequential organ failure assessment (CLIF-SOFA) score
 score")
Chronic liver failure-sequential organ failure assessment (CLIF-SOFA) score


……")
finally simplified to the CLIF-C SOFA score which defines (> 7 – max 18)……



28 -day mortality based on ACLF grade Grade 1 : 22% Grade 2: 32% Grade 3: 77%
 + 1. 71*(INR) +")
CLIF-C AD score 10 * [0. 03*Age + 0. 66*(Creatinine) + 1. 71*(INR) + 0. 88*(WBC) – 0. 05*Sodium + 8] (Age in years; Creatinine in mg/d. L; WBC (white blood count) in 109 cells/L; Sodium in mmol/L. )

Avoiding Futility: Indications for Admission Variceal Bleeding Renal failure Encephalopathy

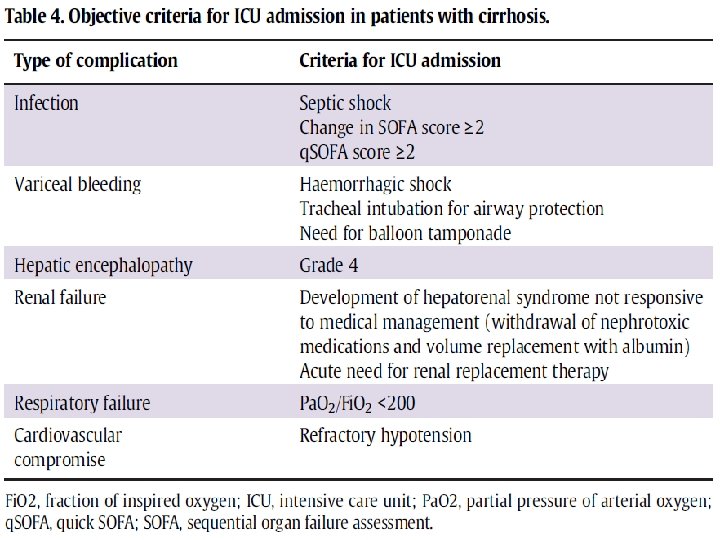
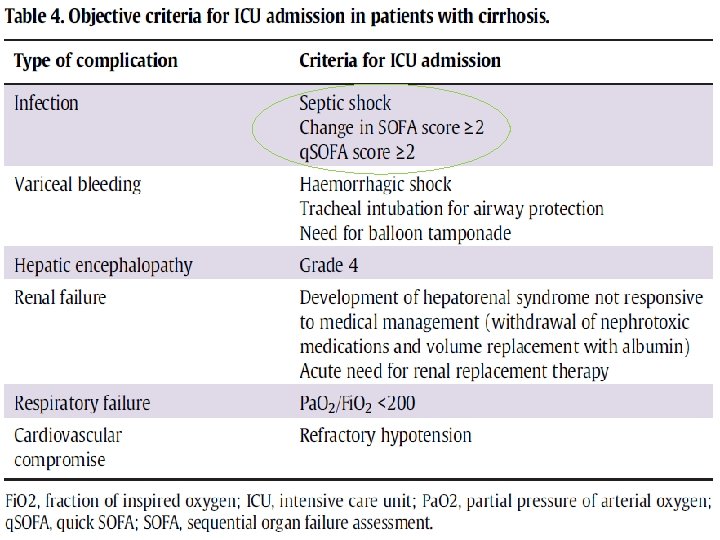
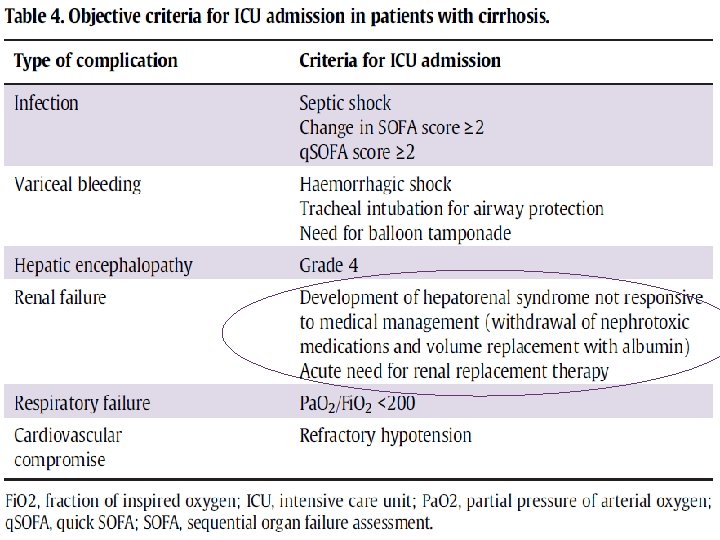
Indication of intensive care unit admission § Patients with cirrhosis require hospitalization in a non-intensive care. § Complications of decompensated liver disease (variceal bleeding, HE, infection, or HRS) are severe or when ACLF develops with extrahepatic organ failure ICU admission is required.

Infection nd u o r a n i t n se e r p e r a s n h t i Infectio w s t n e i t pa f o d r i h t e d n on a s i s o h r r i c d e t a s n e p s h t a e decom d f o % 0 5 o t p u r account fo

Relative immunodeficiency Lack of complement and protein C production by the liver. • Splenomegaly leads to sequestration of immune cells, • Altered gut microflora and translocation of intestinal bacteria also contribute to the development of infection. •
 score>= 15")
Predisposing factors malnutrition recent infection within the past 12 months, (MELD) score>= 15

when ACLF caused by infection The need for critical care and organ support, are greater than if it developed from noninfectious aetiologies was greater Increased mortality in patients with ACLF 90 -day mortality of 51% compared with 38% in patients who did not have an infectious trigger.

Why? ?

§ Cirrhotic patients have a hyperdynamic circulation with elevated cardiac output, decreased arterial pressure, and reduced systemic vascular resistance. § If infection occurs, more hyperdynamic circulation occur and become less responsive to alpha-adrenergic agonists and more liable to develop sepsis and progress to septic shock with multiorgan failure from infection, which is a strong indication for ICU admission.

The early identification • An acute change in the SOFA score of 2 or more points. • The simplified quick SOFA (q. SOFA) score of at least 2.

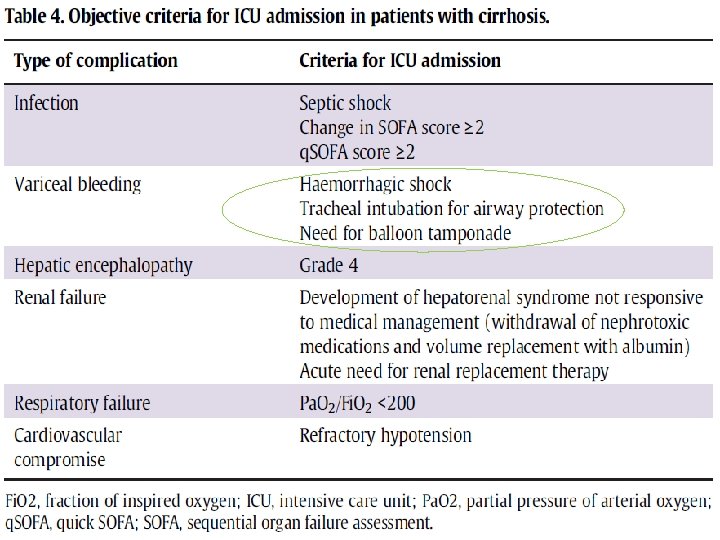
Variceal bleeding l a e c i r a v m ro % Mortality f 0 3 m o r f s e g n a r e g a h n is o i haemorr s s i m d a U C I o S. … % to 50. d e d n e m recom

• Airway protection from aspiration through tracheal intubation. • Rapid resuscitation and immediate initiation of vasoactive agents such as somatostatin, terlipressin, or octreotide. , • Use of vasopressor agents to maintain a MAP of 65 mm. Hg. (haemorrhagic shock ) • Endoscopic therapy is standard treatment within 12 hours • 20% of patients - failure of haemostasis- Balloon tamponade. Intensive care admission is mandatory when balloon tamponade is being implemented

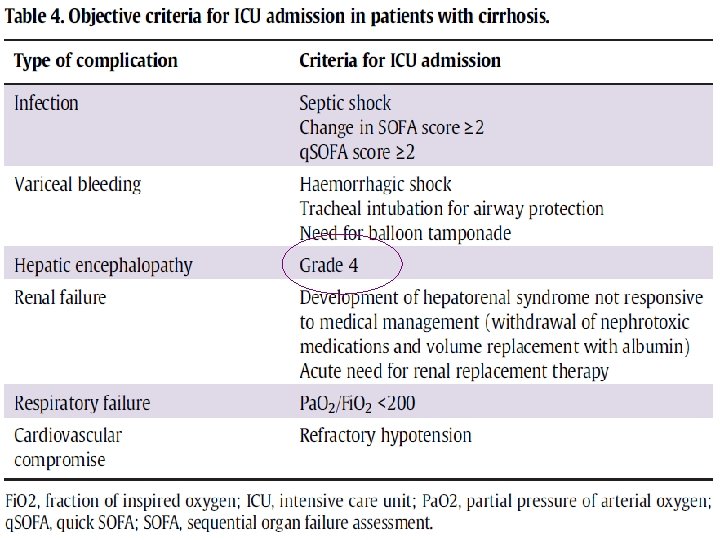
Hepatic encephalopathy y t i l a t r o m , HE f o t e s n o % 0 5 With the n a h t r e at e r g s i r a e at 1 y

• Patients who are grade 4 generally have a Glasgow coma score < 7 and tend to be comatose. . So the presence of severe HE in cirrhotic patients is an indication for management in the ICU, with patients often requiring tracheal intubation for airway protection.

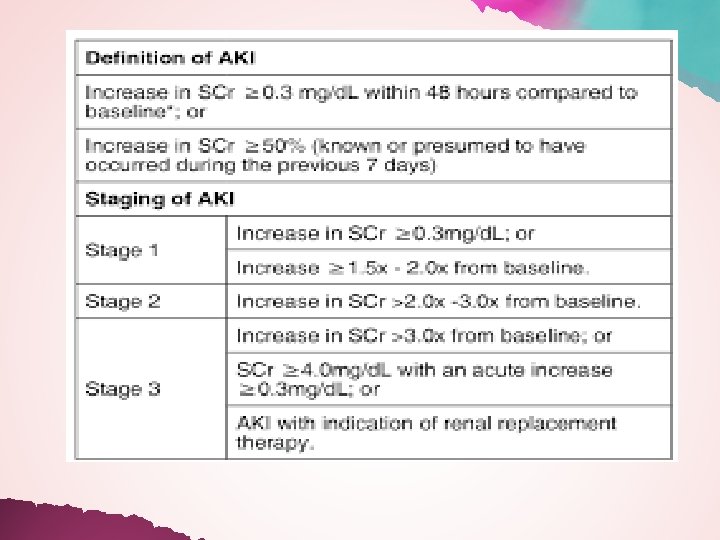
Acute kidney injury n o i t c n u f s dy l a n e r n i s d e s i l AKI result a t i p s f ho o % 0 5 o t d e s a in up e r c n i h it w , s t n e i t a 9% 1 cirrhotic p o t e s o l c f o y t i l a t r o m
 40% of patients within the first 5 years. HRS defined by")
Hepatorenal syndrome (HRS) 40% of patients within the first 5 years. HRS defined by the following criteria: i) presence of cirrhosis and ascites. ii) diagnosis of AKI in accordance with the ICA-AKI criteria. iii) absence of shock. iv) no improvement with 2 days of diuretic stoppage and plasma volume expansion with 1 g/kg body weight of albumin. v) absence of nephrotoxic drug use. vi) absence of macroscopic signs of structural renal disease.

Management of AKI in patients with ACLF -First step is to address any potential underlying cause. -withholding any nephrotoxic drugs, -treating potential infections, -reducing or withdrawing diuretics, - plasma volume expansion in the presence of hypovolemia. Mainstay of treatment of HRS albumin +terlipressin

Indication for ICU admission : • When these measures do not provide an adequate response. • HRS occurs and therapy with vasoactive agents including terlipressin or norepinephrine is indicated. • severe and refractory hypotension. • If terlipressin is unavailable, norepinephrine can also be used along with albumin for the treatment of HRS. (It has been shown to be as effective and as safe as terlipressin). Norepinephrine can only be used in an ICU setting

Other indications for ICU admission in cirrhotics with renal failure Metabolic derangements such as refractory hyperkalemia, metabolic acidosis, severe uraemia, and fluid overload. .

Respiratory failure e h t o t y r a d on c e s s r u c F c L O C A f o e a el u q e s y r o t n. o i t inflamma c e f n i g un l f o e s u a c or be
 to fraction of inspired")
Respiratory failure Partial pressure of arterial oxygen (Pa. O 2) to fraction of inspired oxygen (Fi. O 2) ratio (P/F ratio) of < 200. mm. Hg Which need for ICU admission.

Cardiovascular failure ry o t a m m a l f in o r p f o e s a c i Rele m e t s y s o t s d a e l s e n i al r cytok e h p i r e p d n a n o i t a f o g n inflamm e s or w , n o i t a l i od s a v r e a r l u u s c s s e r va p d loo b l a i r e t r a mean + y h t a p o y m o di r a c c i t o Cirrh

Require for ICU admission for management with vasoactive agents for haemodynamic support
. • Fluid Therapy")
Management • Ensuring adequate venous access for fluids (central venous access). • Fluid Therapy by colloids, crystalloids, BUT not starch • Echocardiography as a first line option for initial evaluation of circulatory failure. • Use of norepinephrine as the first line vasopressor agent • In patients with increasing vasopressor requirements, (refractory shock) hydrocortisone 200– 300 mg/day in divided doses should be administered.
 In patients with cirrhosis and septic shock, the prevalence of AI")
Adrenal insuffeciency (AI) In patients with cirrhosis and septic shock, the prevalence of AI ranges between 51% and 76% ? ? ? s i s Diagno

p o t s o t When w a r d h t i or w ? ? ? e r ca

All patients with a CLIF-C ACLF score of >70 at 48 hours post-ICU admission died within 28 days…… So if no improvement within 48 to 72 hours post-ICU admission. Withdrawal of care should be considered

• At day 3 to 7 ACLF grade is 3. • If the CLIF-C ACLF score is> 64 at 3 to 7 days post diagnosis.

- Slides: 59