Acute Vascular Disorders Acute Lower Limb Ischemia Def

Acute Vascular Disorders

Acute Lower Limb Ischemia • Def: sudden occlusion of a previously patent artery supplying the lower limbs which posses a potential threat to the viability of the limbs. • Causes: Causes The most common cause is embolization. • The heart is the source of embolus in 80 -90% of episodes. • 5 -10% of emboli of unknown origin called cryptogenic emboli.

• if adequate collateral circulation not present, irreversible changes may appear as early as 4 -6 hs after onset. So, priority must be given to restore the blood flow within this period. • Once the occlusive process has begun, vasospasm & propagation of thrombus distal to the site of initial occlusion can contribute to further ischemia.

*The Characteristic S&S are the 6 Ps: 1. Pain. 2. Pallor. 3. Pulselessness. 4. Poikilothermia. 5. Paresthesia. 6. Paralysis.

• Paresthesia: Paresthesia is an essential finding. The earliest sign of tissue loss: • is the loss of: • light touch, 2 point discrimination, vibratory perception, & propreoception esp. in the 1 st web space of the foot ( not pain, pressure or temperature BCZ: - the larger fibers serving these functions are relatively less susceptible to hypoxia).

• Paralysis: Paralysis the onset of motor paralysis is an indication of advanced limb threatening ischemia & impending gangrene If changes persist beyond 12 hs. Tense swelling with acute tenderness of a muscle belly occur. ( common in gastrocnemious muscle after superficial femoral artery occlusion). The extent of paralysis must be determined. • Skin & subcutaneous tissue have greater resistance to hypxia than nerves & muscles. • Peripheral pulses: pulses in earlier stages the pulse at site of occlusion can be palpable but absent distally, because the fresh clot, is soft, semilquid consistency & allow the pulse transmission to the site of occlusion, when becomes organized & densely compacted the pulse lost at site of occlusion.

Arteriography * the gold standard for diagnosis. * it should not be performed if doing so would keep a critically ischemic limb from receiving prompt surgical therapy. * should be reserved for patients with viable limbs who can tolerate the additional delay before revascularization.

Diagnostic testing • CBC, platelets count, Blood chemistry, coagulation profile. • CXR, AXR (look for calcifications), ECG, transesophageal echocardiogram. • Doppler segmental pressure is useful to localize the involved arterial segment and as a quantitative index to gauge the severity of the problem.

Management • If physical examination demonstrates clear evidence of embolization, the definitive therapy should not be delayed. • Immediate heparin i. v bolus of 80 units/kg, followed by i. v. infusion of 18 units/kg/h, & PTT should be maintained between 60 -80 sec. Heparin prevents proximal and distal propagation of thrombus, maintains patency of collateral vessels, and in addition can have a beneficial effect by reducing the extent of ischemic injury

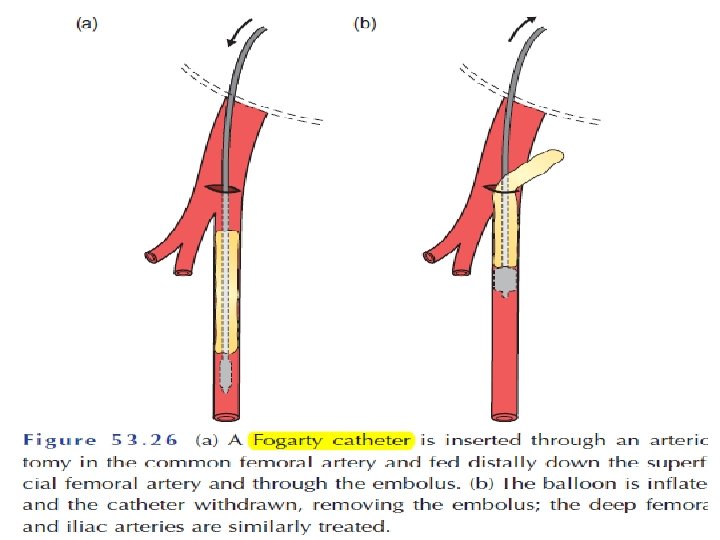
Surgical therapy • Embolectomy: - under local or general anesthesia. - Fogarty catheter used. - intraoperative thrombolysis When residual thrombus exists. - intraoperative arteriogramis necessary to define the position of the clots so that the catheter can be placed as close to the clot as possible. and When the viability of the extremity is threatened or when there are poor Doppler signals in the distal extremity. - Bypass grafting. ***Heparin is reinstituted 6 to 12 hours after surgery because of a significant incidence of recurrent embolism. ***Amputation (usually after 12 hs the limb is paralysed due to irreversible damage).

catheter embolectomy is done through the common femoral artery. Most aortic, iliac, superficial femoral, and popliteal artery occlusions can be managed successfully through this vessel.

• Thrombolytic therapy Useful in patients with clearly viable extremity in whom thrombosis is the likely underlying cause of their acute ischemia. In general the fresher the thrombus the more successful the thrombolysis. Urokinase is the agent of choice • Percutaneous aspiration thromboembolectomy Useful as an adjunct to thrombolysis to reduce the clot volume

Complications 1. Reperfusion injury: reestablishment of blood flow leads to further tissue death. * results from formation of oxygen-free radicals. *cause direct tissue damage & accumulation of WBCs & sequestration in the microvascular system, * it prolongs the ischemia despite restoration of axial blood flow. * currently no proved therapy limits the injury. 2. Compartment syndrome: * prolonged ischemia cause cell membrane damage & leak of fluid to interstitium. * edema increased intracompartmental pressure, when exceeds CPP, further muscle & nerves necrosis occur. * Fasciotomy should be done if ischemia>6 h * 2 incisions, one antrolateral, one posteromedial. * skin lift open, to be closed either secondarily or by graft later on.

Compartment syndrome: . ο Indications for fasciotomy: ♦ 4– 6 hour delay after vessel injury. ♦ Combined vein and artery injury. ♦ Concomitant fracture/crush, severe soft-tissue injury, muscle edema or patchy necrosis. ♦ Tense compartment/compartment pressures exceeding 40 mm Hg. ♦ Prophylactic for patients with prolonged transport times or long periods without observation (no surgical care available).

3. Myo-nephropathic syndrome: * products of ischemic muscles as K, lactic acid, myoglobin, Cr phosphokinase released to the circulation after reperfusion. leads to arrhythmias & renal failure * aggressive: hydration, diuresis as mannitol, mannitol intravenous sodium bicarbonate sufficient to alkalinize the urine Alkalinization of the urine reduces the extent of myoglobin precipitation in the renal tubules. Insulin and glucose given intravenously may be necessary for extreme or sudden elevations in serum potassium levels.

4. Catheter related complications: complications * early: early from arterial wall trauma includes perforation, rupture, intimal dissection, pseudoaneurysm formation. * late: development of accelerated atherosclerosis in the embolectomized vessel.

Vascular injury • • • Epidemiology Peripheral vascular trauma typically occurs in young men between the ages of 20 and 40 years. many vascular injuries of the head, neck are immediately fatal. High risk areas: areas • Upper extremity: axilla, deltopectoral groove, anticubital fossa. wound distal to the bifurcation of brachial artery: no serious limb ischemia. • Lower extremity: top of the leg till the mid calf.

Types of Injuries A. Penetrating Trauma 1. Stab wounds, 2. bullet wounds. 3. iatrogenic injuries from Percutaneous catheterization, and intra-arterial injection of drugs 4. high-velocity missiles & Shotgun blasts may produce arterial thrombosis due to disrupted intima even when the artery has not been directly hit.

B. Blunt Trauma • Motor vehicle accidents. • Multiple injuries include fractures and dislocations; dislocations and while direct vascular injury may occur, in most instances the damage is indirect due to fractures. This is especially likely to occur with fractures near joints, joints where vessels are relatively fixed and vulnerable to shear forces. For example, the Popliteal artery and vein are frequently injured in association with posterior dislocation of the knee. Fractures of large heavy bones such as the femur or tibia. • Contusions or crush injuries may result in complete or partial disruption of arteries, producing intimal flaps or intramural hematomas that impede blood flow.

Clinical Findings A. Hemorrhage • When pulsatile external hemorrhage is present, the diagnosis of arterial injury is obvious, but when blood accumulates in deep tissues of the extremity, the thorax, abdomen, or retroperitoneum, the only manifestation may be shock. • The presence of arterial pulses distal to a penetrating wound does not preclude arterial injury, either because the vessel has not thrombosed or because pulse waves are transmitted through soft clot. Conversely, the absence of a palpable pulse in an adequately resuscitated patient is a sensitive indicator of arterial injury. B. Ischemia.

C. Arteriovenous Fistula • With simultaneous injury of an adjacent artery and vein, a fistula may form that allows blood from the artery to enter the vein. • Because venous pressure is lower than arterial pressure, flow through an arteriovenous fistula is continuous; accentuation of the bruit and thrill can be detected over the fistula during systole. • Traumatic arteriovenous fistulas may occur as operative complications. • Long-standing large arteriovenous fistulas may result in cardiac failure. • spontaneous resolution of acute arteriovenous fistulas usually occurs.

• The time interval between injury & evaluation must be considered. - after more than 6 hs of warm ischemia at body temperature ( without cooling the extremity) results in irreversible nerve & muscle damage in 10% of patients.

Diagnosis • Arterial injury must be considered in any injured patient. Patients who present in shock following penetrating injury or blunt trauma should be assumed to have vascular injury until proved otherwise. • Any injury near a major artery should arouse suspicion. • A plain film may be helpful in demonstrating a fracture whose fragments could affect an adjacent vessel or a bullet fragment that could have passed near to a major vessel. Before the x-ray is taken, entrance and exit wounds should be marked with radiopaque objects such as safety pins.

Hard signs • 1. 2. 3. 4. 5. the presence of hard signs has a 92 -95% sensitivity for injuries requiring intervention Bruit or thrill is present in 45% of patients with an AV fistula. Active or pulsatile hemorrhage Pulsatile or expanding hematoma Signs of limb ischemia 6 Ps. Diminished or absent pulses: pulses not a sensitive prognostic sign, as up to 25% of patients requiring repair have normal pulses distal to the injury.

Soft signs • • 1. 2. 3. 4. Much less useful in predicting or excluding major peripheral vascular injuries. The vast majority of these lesions do not require emergent repair. Hypotension or shock Neurologic deficit due to primary nerve injury occurs immediately after injury, in contrast, ischemic neuropathy is delayed in onset (minutes to hrs). Stable non- pulsatile or small hematoma. The proximity of the wound to major vascular structure.
, (ABI determined by dividing")
• Doppler flow • An ankle brachial index (ABI), (ABI determined by dividing the systolic pressure in the injured limb by the systolic pressure in an uninjured arm, is highly reliable for excluding arterial injury after both blunt and penetrating trauma. An ABI < 0. 9 has sensitivity of 95%, specificity of 97%, for determining the presence of clinically significant arterial injury. Thus, only patients with "soft" signs and an ABI of < 0, 9 require arteriography.

• Color flow duplex ultrasonography This technology can provide images of vessels and velocity spectral analysis. *Color flow duplex scanning of an area of injury is noninvasive, painless, portable, and easily repeated for follow-up examinations. *duplex ultrasound identifies nearly all major injuries that require treatment. In addition to screening for arterial trauma, duplex scanning has been used to detect pseudoaneurysms, arteriovenous fistulas, and intimal flaps. *The technology is sophisticated and requires skill in operation and interpretation, which is not always immediately available.

• Arteriography is the most accurate diagnostic procedure for identifying vascular injuries. • Arteriography is also valuable when arterial injuries may have occurred at multiple sites to localize an injury. Complications of arteriography include : • groin hematomas, iatrogenic pseudoaneurysms, arteriovenous fistulas, embolic occlusions, and delays in diagnosis that may lead to irreversible ischemia in marginally perfused limbs. • Arteriography may be particularly useful in differentiating arterial injury from spasm.

• In general, it is risky to attribute abnormal physical findings in an injured patient to arterial spasm; an arteriogram is indicated in such patients. • MRA lacks sufficient resolution to detect significant arterial abnormalities. • CT scans may reveal intra-abdominal or thoracic hematomas or organ displacement, suggesting the presence of a hematoma. This suggests the need for arteriography or immediate surgery.

Management Aspects • Initial management. ο Control external bleeding immediately! Direct pressure to the bleeding wound is; temporary tourniquet (BP cuff) placed proximal to the injury site and inflated above systolic blood pressure may be useful. ο Administer IV antibiotics, tetanus toxoid, and analgesia. ο In most long-bone fractures, resuscitation and fracture alignment will restore distal flow. ο Indications for operation for a suspected vascular injury: ♦ Hard signs. ♦ Soft signs confirmed by duplex US and/or angiography.

Operative management. **Preparation of injured extremity as well as contralateral uninjured lower or upper extremity in case repair requires autogenous vein graft. **Longitudinal incisions usually directly over injured vessel followed by proximal and distal control. Once control is obtained, perform the following steps: ♦ Debride injured vessels to macroscopically normal wall. ♦ Pass balloon catheters proximal and distal to remove any residual thrombus. ♦ Flush both directions with heparinized saline

Type of repair will depend on the extent of injury. ο Lateral suture repair: Required for minimal injuries that, when repaired, will not compromise the lumen nor decrease pulse or Doppler signal. ο End-to-end anastomosis: Excise extensively damaged segments and perform anastomosis if able to mobilize ends (generally, < 2 cm gap) without tension. An oblique anastomosis is less likely to stenose. Interposition graft: Required if the vessel cannot be primarily repaired without undue tension. ♦ Autogenous vein grafts preferred, usually the contralateral greater saphenous vein (GSV). ♦ Prosthetic grafts may be required when autogenous vein is inadequate or unavailable. ◊ Polytetrafluoroethylene (PTFE) grafts
- Slides: 34