Acute treatment of migraine Dr Mark Weatherall London

















- Slides: 27
Acute treatment of migraine Dr Mark Weatherall London Headache Centre 2010
The intangibles l l l Doctor-patient relationship Realistic expectations Education
Triggers l l l Hormonal Dietary Psychological Environmental Sleep Drugs
10 steps to success l l l Make the diagnosis Use the right drugs Use effective doses Treat early when the pains mild Treat associated symptoms
10 steps to success l l l Choose appropriate route of delivery Observe contraindications Use prior experience to select/reject drugs Avoid drugs with high potential for MOH Combine medications if necessary
Where to start? paracetamol 1 g l or, aspirin 900 mg l or, ibuprofen 600 -800 mg l +/- domperidone 10 -20 mg l taken as soon as possible*ª l * i. e. as soon as the patient knows that this is a migraine ª if there is aura, take at the start of the headache phase
Variations on a theme l l l if early nausea, you can use: soluble aspirin suppositories*: l l diclofenac 75 mg domperidone 30 mg *be French!
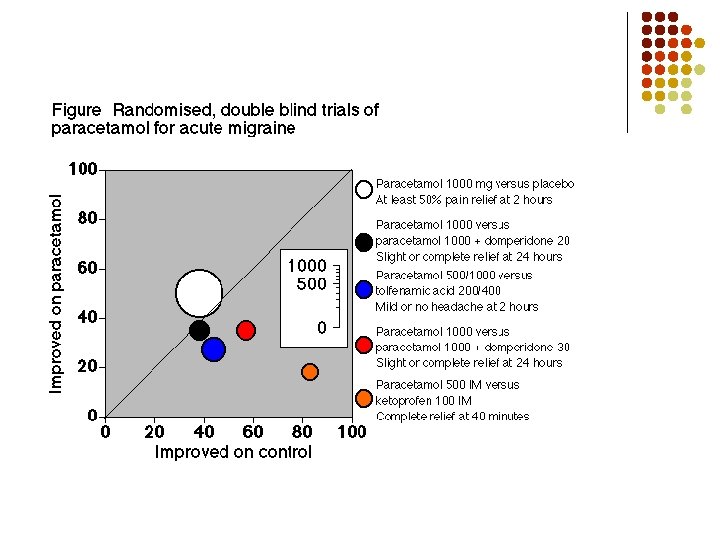
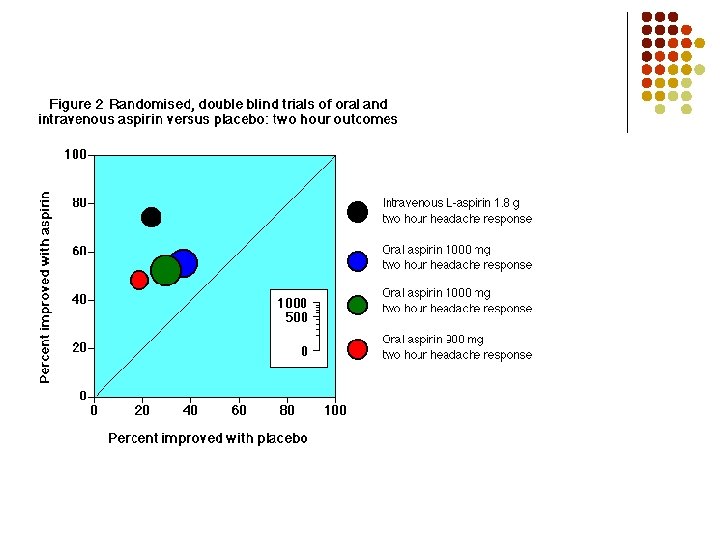
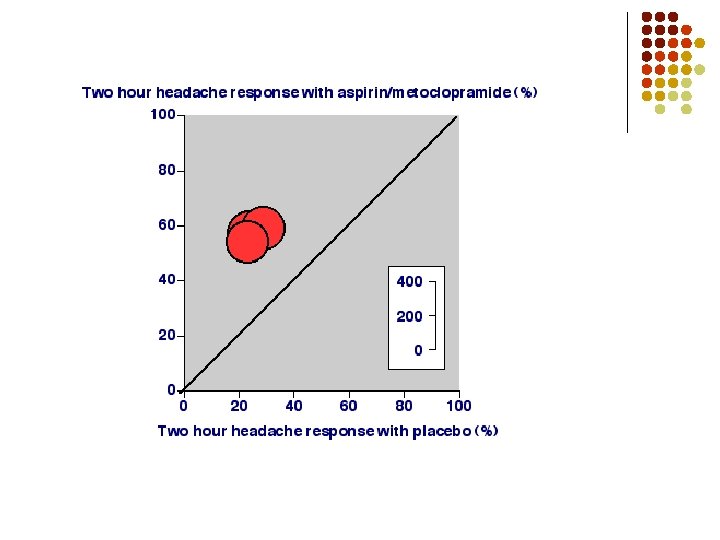
Headache response at 2 hr
Problems, problems… l Not effective l l Contraindications l l dose? timing? route? combination? asthma, upper GI problems, renal impairment Side effects l GI, CNS
Codeine…? l l … is NOT a treatment for headache the WHO analgesic ladder should NOT be applied to headache management
Triptans l l l 5 -HT 1 B/1 D receptor agonists seven different formulations options for route of delivery l l oral tablets or melts nasal spray subcutaneous injection taken as soon as possible*ª¹ * i. e. as soon as the patient knows that this is a migraine ª if there is aura, take at the start of the headache phase ¹ this is a race against the development of allodynia
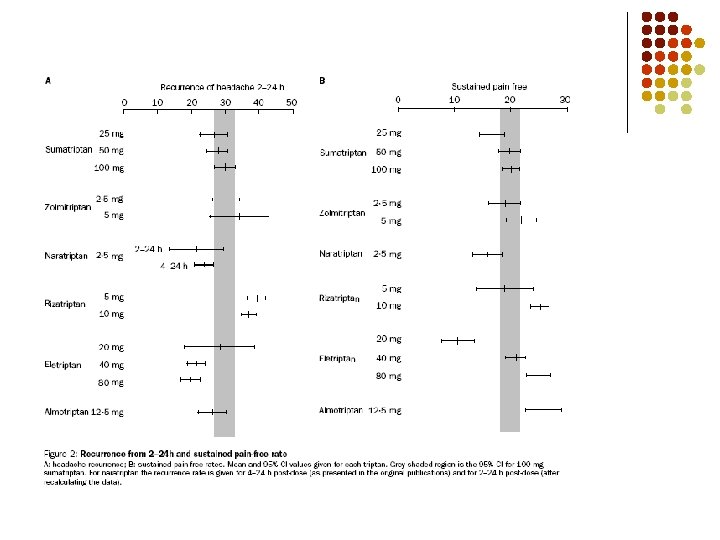
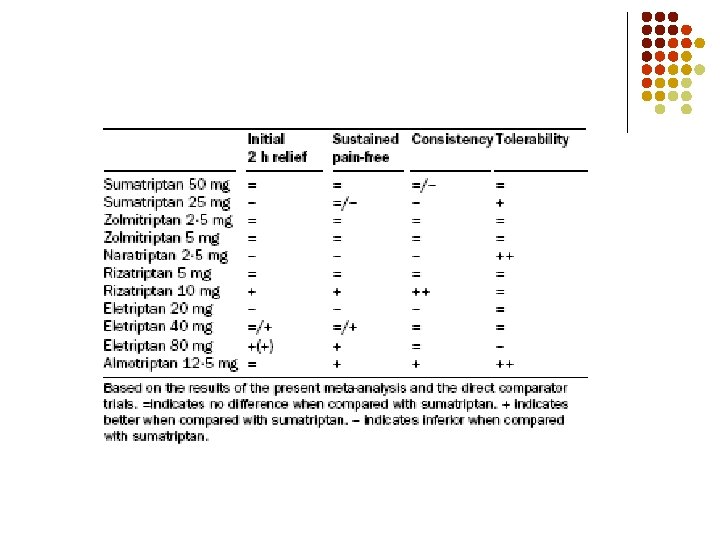
Which triptan?
Headache response at 2 hr
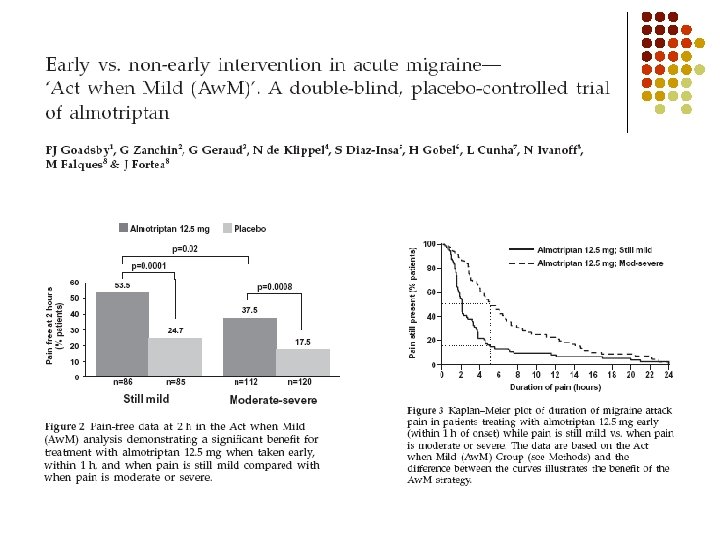
Pain freedom at 2 hr
Problems, problems… l Ineffective l l Headache recurrence l l switch? combination with NSAID? Contraindications l l dose? timing? route? switch? HT, IHD SE l nausea, GI, CNS, ‘triptan chest’
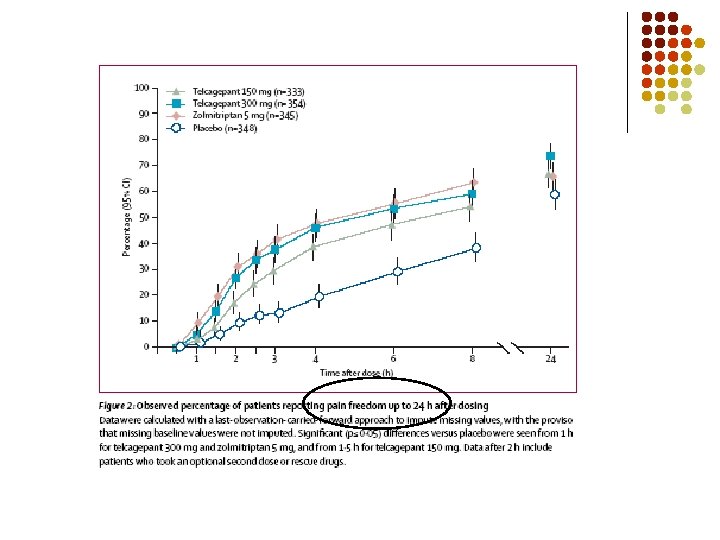
Is the future ‘pants’? l CGRP antagonists l l l two with data recently published proof-of-concept trial of intravenous BIBN 4096 BS (now called olcagepant) was published in NEJM in 2004 phase II study of oral CGRP antagonist MK-0974 (now called telcagepant) presented at IHS 2007 and published in Neurology in 2008
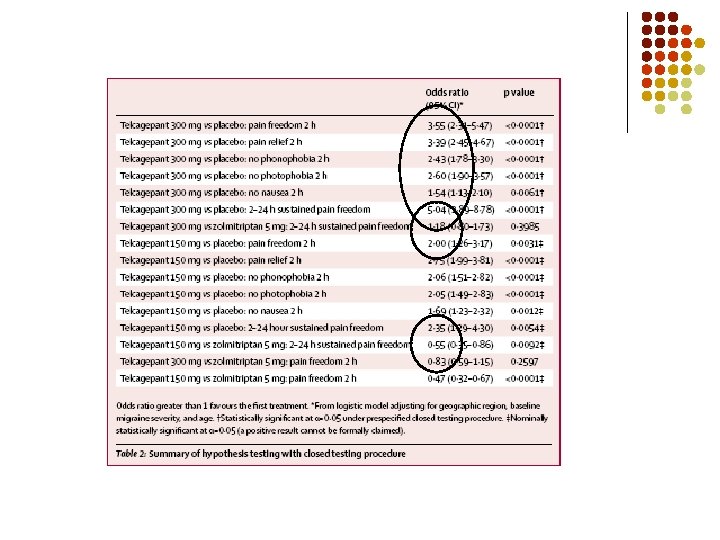
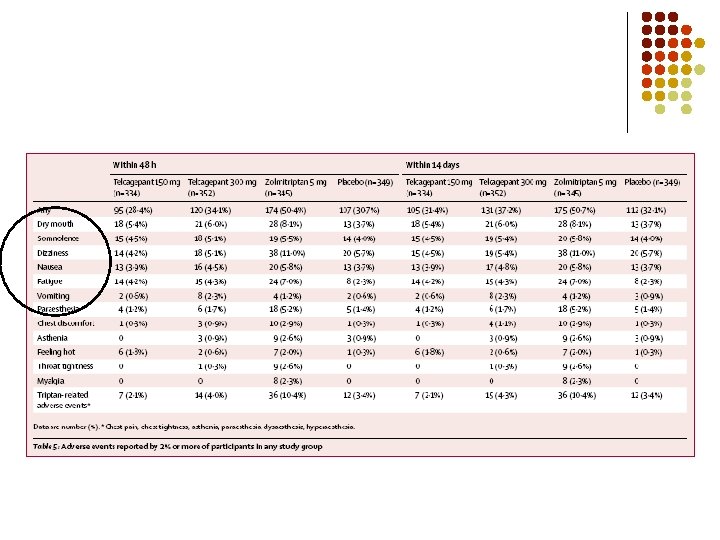
l multicentre phase III R-PT-PC-DB-T of oral telcagepant 150 or 300 mg vs zolmitriptan 5 mg and placebo published in The Lancet in last four weeks