Acute Pulmonary Edema in the Cath Lab A

Acute Pulmonary Edema in the Cath Lab A Case Presentation

David Lu, MD I have no relevant financial relationships or disclosures

Case Presentation 67 yo F with hx of NIDDM, HTN, HLP, “atypical CP” 2013, and former smoker presents with 1 day of chest pain and dyspnea. • Began 9: 30 pm the night prior, while cooking • Left sided, substernal, radiation to neck, left arm, and felt like “rubber band” around chest • Pain lasted ~30 min before going to bed, recurred at 11 AM when walking across the parking lot • Arrived in ED at 1: 30 pm with SOB • ROS positive for nausea

PMHx - NIDDM - HTN - HLD - OA of hip/knee - Osteoporosis - ? Seizure disorder PSHx - Hysterectomy w BSO - Left ankle ORIF Family Hx - Noncontributory Medications - Atorvastatin - Losartan - Metformin - Nifedipine - Levetiracetam Allergies - Penicillin - Codeine - Tramadol Social Hx -Former smoker. Quit in 2014

Physical Exam VS: T 98. 8 F HR 99 BP 135/78 RR 21 Sp. O 2 98% on room air GEN: No acute distress, awake and alert HEENT: PEERLA, pink conj, EOMI, moist mucous membranes CHEST: clear to auscultation bilaterally, no wheezing, no crackles CV: regular rate, rhythm, good peripheral pulses, good cap refill ABD: normal sounds, no tenderness, no heptasplenomegaly, no masses SKIN: No rashes, no lesions NEURO: Alert and oriented x 3, normal reflexes, normal strength and sensation, normal gait

Baseline ECG

ECG in ED


Labs 13. 0 12. 0 40. 0 252 POC Troponin 1. 99 POC BNP 141. 0 INR 0. 9 138 102 11. 0 4. 1 20 0. 6 282 Ca 9. 5 Mg 1. 6 PO 4 3. 2

ED Course • SL Nitro x 1 significant improvement in chest pain • Aspirin 325 mg • Heparin gtt • Plavix • What should we do next on a Saturday?
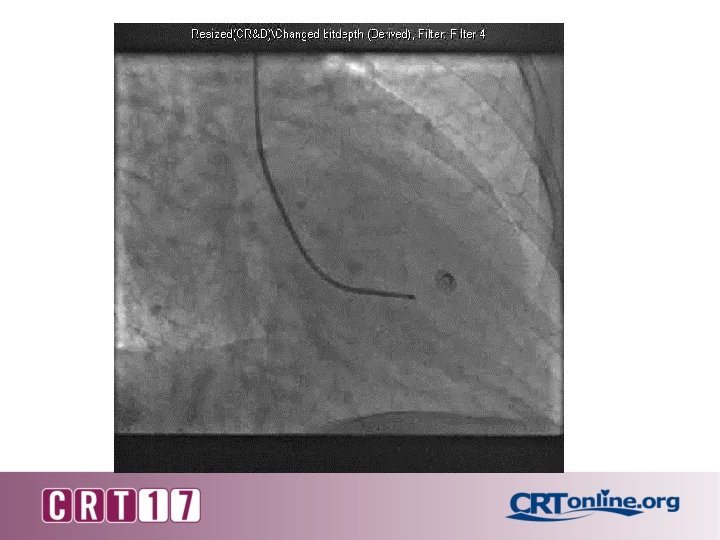
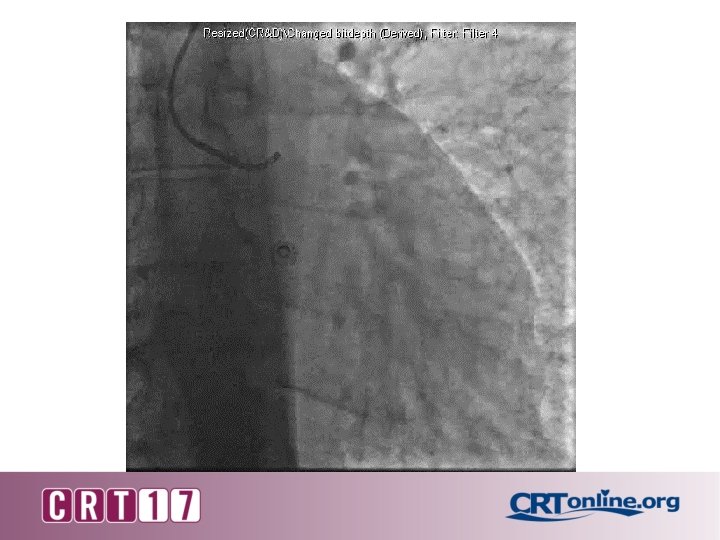

Taken to cath lab from ER for NSTEMI • Pt developed cough during angiogram • Suspecting allergic reaction, she was given IV diphenhydramine 50 mg • Reports difficulty breathing; sat up, broke sterile field • ED attending called for sedation and intubation • Auscultation of lungs revealed bilateral rales without wheezing or stridor

• After intubation, pt became hypotensive, unresponsive, and started frothing from the mouth • Dopamine initiated • Patient became bradycardic and eventually pulseless • CODE BLUE called at 15: 55 • Given multiple rounds of epinephrine, bicarb, calcium • Inline suction through the ET tube revealed copious amounts of pink froth

• Airway ventilation because increasingly difficult • Rhythm on monitor changed from PEA to asystole • Pacing wire was inserted, but failed to cross TV under fluoroscopic guidance • Cardiac US showed no pericardial effusion; no LV contraction • Pt was pronounced 17: 20 pm

What happened?

Mechanical Complications of AMI 1. Rupture of the LV wall rupture 2. Rupture of the interventricular septum 3. Acute mitral regurgitation

Papillary Muscle Rupture

Histology

1 -3 days 12 -24 hr 3 -7 days > 6 wks

Questions • • IABP Impella Emergency surgery? Percutaneous MV?

Thank You

Sequence of Changes in MI TIME GROSS 0 -6 hr None MICROSCOPIC None; wavy fibers (~4 hr) 6 -12 hr None/ Few “wavy” fibers Mottling 12 -24 hr 24 -72 hr 3 -7 d Pallor/ Coagulation Necrosis (Eosinophilic Mottling myocytes), few neutrophils; edema, hemorrhage Pallor Coagulation Necrosis, Dense neutrophil infiltrate, loss of nuclei and cross striations Pallor Macrophages replace neutrophils Granulation tissue forms from periphery

Sequence of Changes in MI TIME GROSS MICROSCOPIC 7 -10 d Yellow-gray center Macrophages, granulation tissue at edges 10 -21 d Gray Fibrosis increasing 6 wk-1 yr Scar reaches full Fibrosis tensile strength at 1 year

• 12 -24 hr: 1. 2. 3. 4. Coag. Necrosis Wavy fibers Edema Some neutrophils

• 1 -3 days: 1. Dense neutrophils 2. Loss of dead myocytes.

• 3 -7 days: 1. Completion of Myocyte removal. 2. Macrophages replace neutrophils. 3. Granulation tissue starts to form.

• 7 Days – few weeks: 1. Granulation Tissue 2. Fibrosis

• >6 weeks: 1. Fibrous scar develops. 2. Full strength at 1 yr.
- Slides: 29