ACUTE PERICARDITIS PERICARDIAL EFFUSION TAMPONADE 1 2 3

 2) 3) 4) 5) Anatomy of pericardium Overview of pericardial disease Etiology Clinical")






 Chest pain Sudden onset localized to anterior chest wall pleuritic sharp Positional: may")















, viral, fungal � CA - Esp lung, breast, Hodgkin’s,")





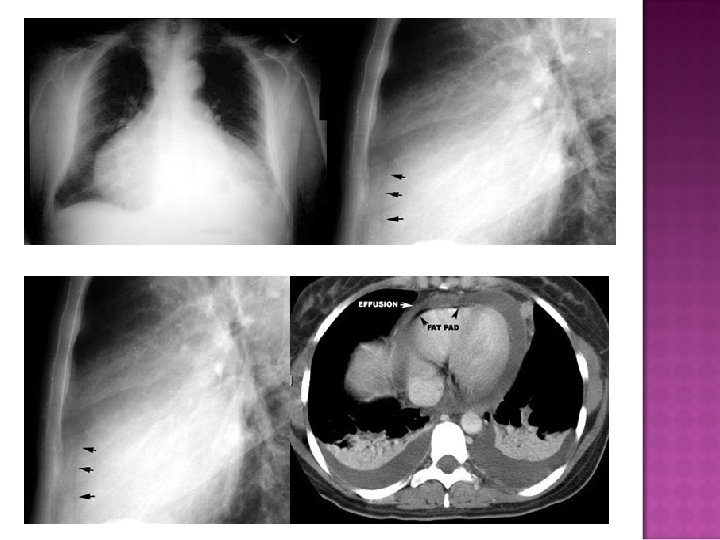
 fat pad sign �Separation of mediastinal / retrosternal fat and epicardial")




- Slides: 49
ACUTE PERICARDITIS PERICARDIAL EFFUSION TAMPONADE
1) 2) 3) 4) 5) Anatomy of pericardium Overview of pericardial disease Etiology Clinical presentation Treatment
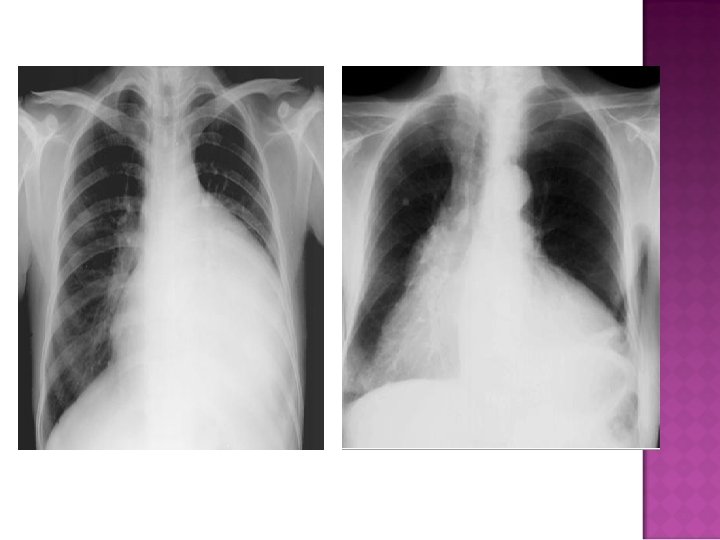
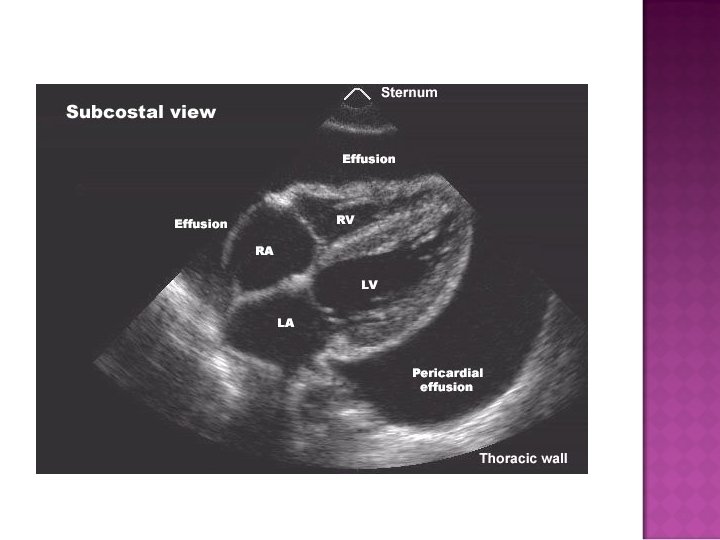
Normal amount of pericardial fluid: 15 -50 cc Two layers: Outer layer is the parietal pericardium and consists of layers of fibrous and serous tissue Inner layer is visceral pericardium and consists of serous tissue only
Fibroelastic sac consisting of 2 layers Visceral at epicardial side Parietal at mediastinal side Pericardial fluid formed from ultrafiltrate of plasma
� Acute Fibrinous Pericarditis � Pericardial Effusion �Cardiac tamponade � Recurrent Pericarditis � Constrictive Pericarditis
� 0. 1% � 5% of hospitalized patients of patients admitted to Emergency Department for non-acute myocardial infarction chest pain
� Exact incidence and prevalence are unknown � Diagnosed in 0. 1% of hospitalized patients and 5% of patients admitted for non-acute MI chest pain � Observational study: 27. 7 cases/100, 000 population/year
Chest pain: anterior chest, sudden onset, pleuritic; may decrease in intensity when leans forward, may radiate to one or both trapezius ridges Pericardial friction rub: most specific, heard best at LSB EKG changes: new widespread ST elevation or PR depression Pericardial effusion: absence of does not exclude diagnosis of pericarditis Supporting signs/symptoms: Elevated ESR, CRP Fever leukocytosis
1) Chest pain Sudden onset localized to anterior chest wall pleuritic sharp Positional: may improve if pt leans forward, worse with lying flat 2) Cardiac auscultation: Pericardial friction rub Present in up to 85% of pts with pericarditis without effusion friction of the two inflamed layers of pericardium, typically triphasic rub, heard with diaphragm of stethoscope at left sternal border 3) Characteristic ECG changes 4) Pericardial effusion
Stage 1: hours to days Diffuse ST elevation -sensitive v 5 -v 6, I, II ST depression I/a. VR PR elevation a. VR PR depression diffuse -especially v 5 -v 6 PR change is marker of atrial injury Stage 2: Normalization
Stage 3: Diffuse T wave inversions ST segments isoelectric Stage 4: EKG may normalize T wave inversions may persist indefinitely
ST elevation in pericarditis Starts at J point Rarely exceeds 5 mm Retains normal concavity Non-localizing Arrhythmias very unlikely in pericarditis (suggest myocarditis or MI)
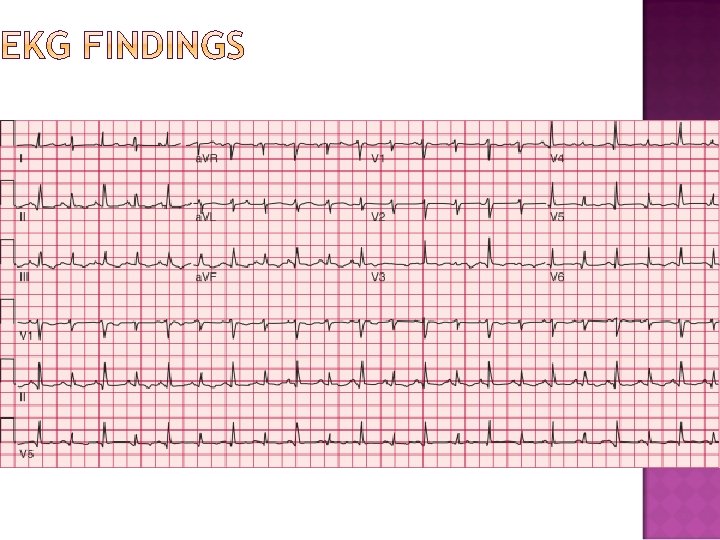
51 yo man with acute onset sharp substernal chest pain two days prior
Electrocardiogram in acute pericarditis showing diffuse upsloping ST segment elevations seen best here in leads II, III, a. VF, and V 2 to V 6. There is also subtle PR segment deviation (positive in a. VR, negative in most other leads). ST segment elevation is due to a ventricular current of injury associated with
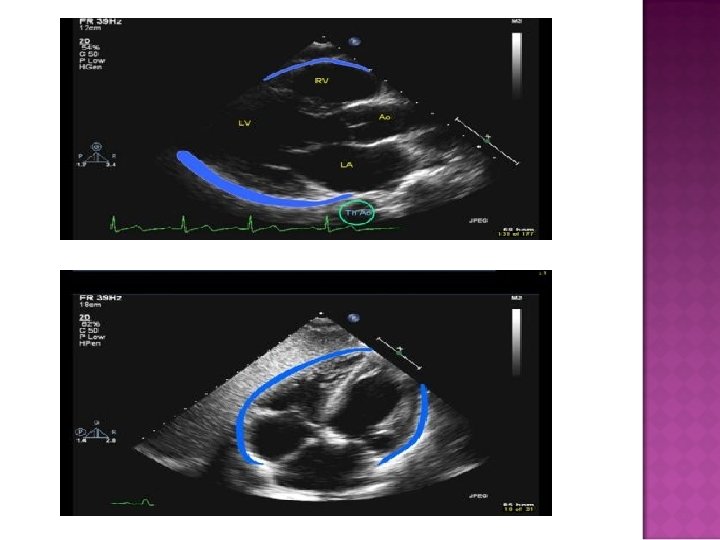
Small Moderate Large Location Posterior Inferior to LV Extends to apex Circumscribes heart *Meas. @ Diastole <10 mm 10 -15 mm >15 mm *maximal width of pericardial stripe
Low voltage and Electric Alternans
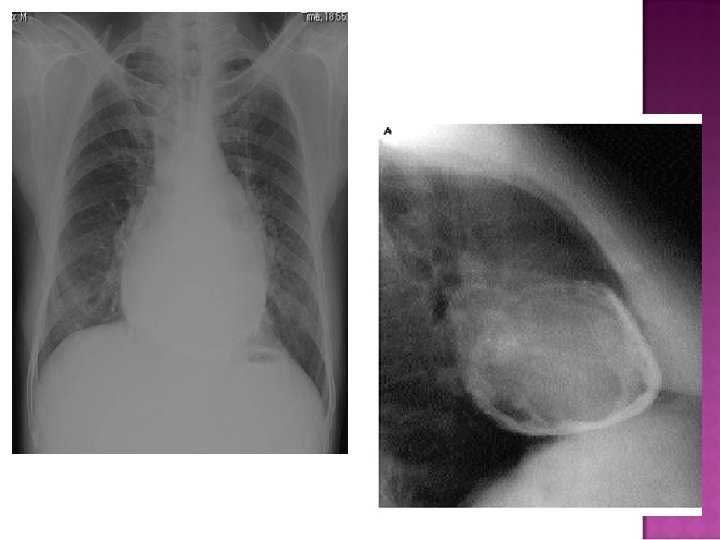
Cardiomegaly due to a massive pericardial effusion. At least 200 m. L of pericardial fluid must accumulate before the cardiac silhouette enlarges.
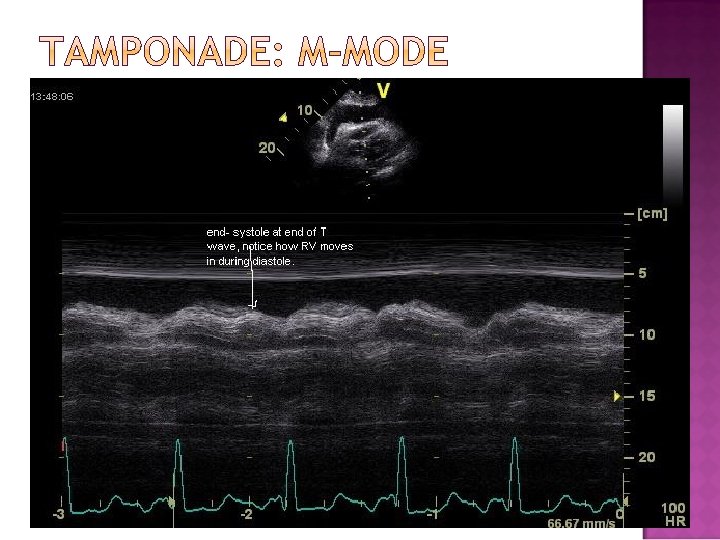
� M-Mode
� M-mode Cannot determine volume of accumulated fluid accurately
Aspirin NSAIDs Colchicine: can reduce or eliminate need for glucocorticoids Glucocorticoids: should be avoided unless required to treat patients who fail NSAID and colchicine therapy Many believe that prednisone may perpetuate recurrences Intrapericardial glucocorticoid therapy: sx improvement and prevention of recurrence in 90% of patients at 3 months and 84% at one year Other immunosuppression Azothoprine (75 -100 mg/day) Cyclophosphamide Mycophenolate: anecdotal evidence only Methotrexate: limited data IVIG: limited data Pericardiectomy: To avoid poor wound healing, recommended to be off prednisone for one year. Reserved for the following cases: If >1 recurrence is accompanied by tamponade If recurrence is principally manifested by persistent pain despite an intensive medical trial and evidence of serious glucocorticoid toxicity
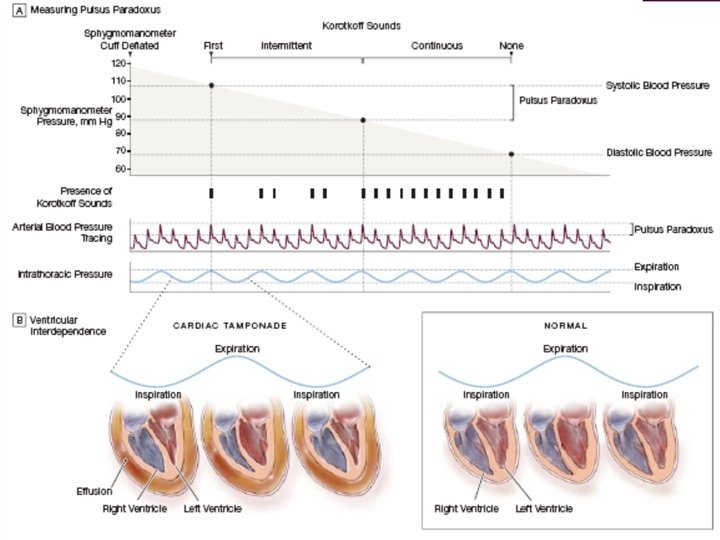
� Normal amt of pericardial fluid = 20 -50 m. L � Tamponade occurs when lg or rapidly formed effusions inc’d pressure in the pericardial space throughout the cardiac cycle � During inspiration, RV volume inc’s & in tamponade, the RV is unable to expand into the maximally stretched pericardium Lward bulging of the interventricular septum dec’d LVEDV dec’d cardiac output & dec’d SBP during inspiration
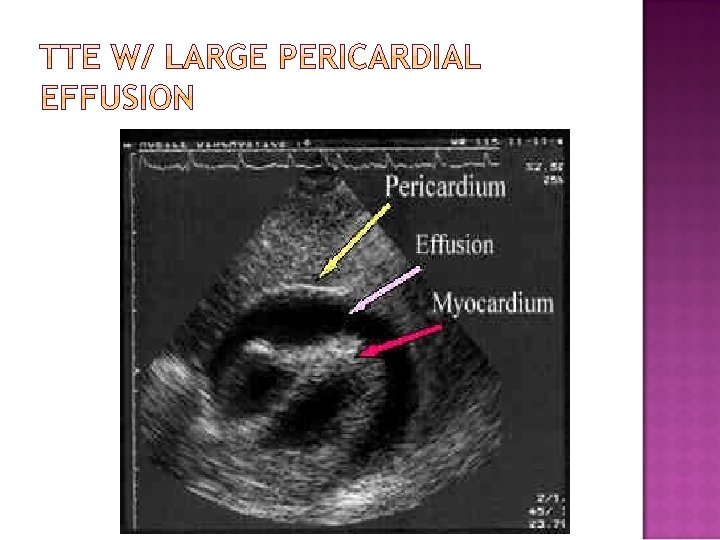
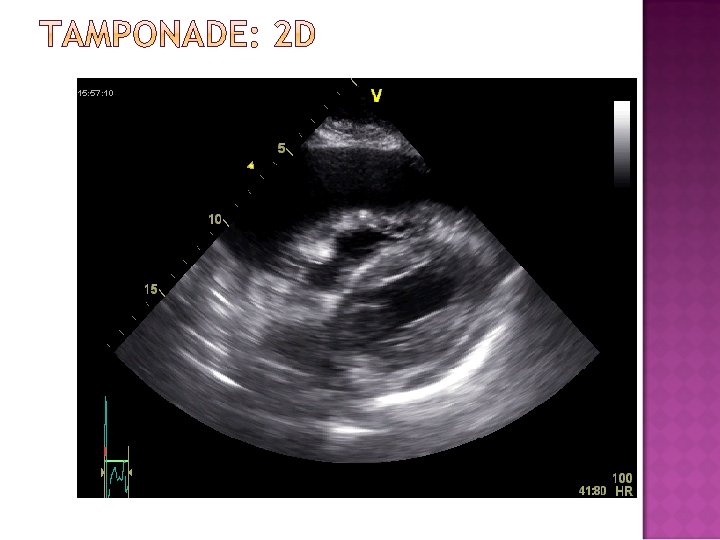
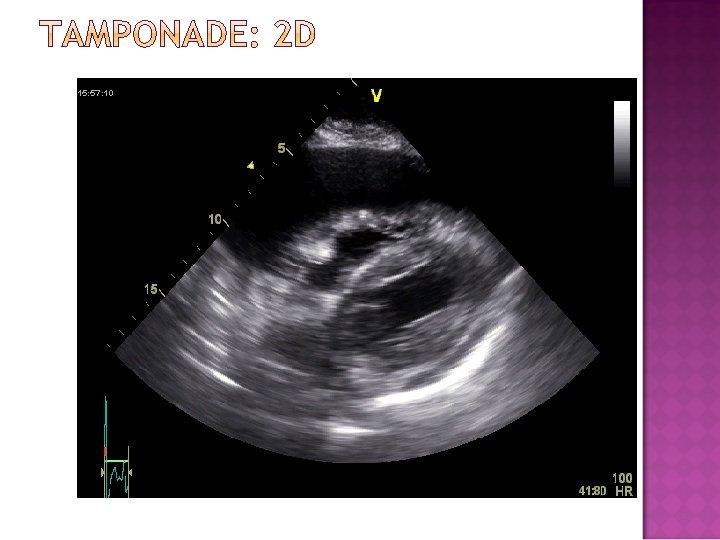
�Pressure in pericardium exceeds s �Compressive effect in intrachamber �Diagnostic techniques � 2 D looking for RA/RV collapse during diastole �M-mode for RA/RV collapse during diastole �Doppler of Mitral and Tricuspid inflow Mitral inflow to decrease by 25% with inspiration Tricuspid inflow increased by 40% with inspiration �IVC diameter fails to increase with inspiration
� HIV, bacterial (incl mycobacterial), viral, fungal � CA - Esp lung, breast, Hodgkin’s, mesothelioma � Radiation tx � Meds - Hydralazine, Procainamide, INH, Minoxidil � Post-MI (free wall ventricular rupture, Dressler’s syndrome) � Connective tissue dzs – SLE, RA, Dermatomyositis � Uremia � Trauma � Iatrogenic – (eg, from TLC / PA Cath / TV pacemaker insertion, coronary dissection & perforation, sternal bx, pericardiocentesis, GE jnx surgeries) � Other - Pneumopericardium (d/t mech ventilation or gastropericardial fistula), Pleural effusions � Idiopathic
� Sxs � Chest Pain, dyspnea, near-syncope � Generally more comfortable sitting forward � Sxs c/w the underlying cause of tamponade � Physical � Beck’s sounds Exam Triad - Elev’d JVP, hypotension, dec’d heart JVP w/ preserved x descent and dampened or absent y descent Generally w/ narrow pulse pressure � Tachycardia, other signs of HF (tachypnea, diaphoresis, cool extremities, cyanosis, etc) � Pulsus paradoxus � Dec’d or absent cardiac impulse � +/- Friction rub
Dec in SBP > 10 -12 mm. Hg w/ inspiration Can also occur in pts w/ COPD, pulm dz, PTX, severe asthma Can have tamponade w/o pulsus paradoxus In pts w/ pre-existing elev’s in diastolic pressures and/or volume (eg, LV dysfnx, AI and ASD)
� Tamponade � Other is a Clinical Diagnosis Detection Methods �EKG �CXR �TTE �R Heart Cath �CT, MRI
� Common Findings � Sinus tachycardia � Non-specific ST segment and T wave changes � Changes assoc’d w/ acute pericarditis (incl diffuse STE & PR depression) � Other Findings � Dec’d voltage (non-specific and can also be d/t emphysema, infiltrative myocardial dz, PTX, etc) � Electrical alternans (specific but relatively insensitive for lg effusions) 2/2 anterior-posterior swinging of the heart w/ each beat Best seen in leads V 2 to V 4 � Combined P wave and QRS complex alternation (specific for cardiac tamponade)
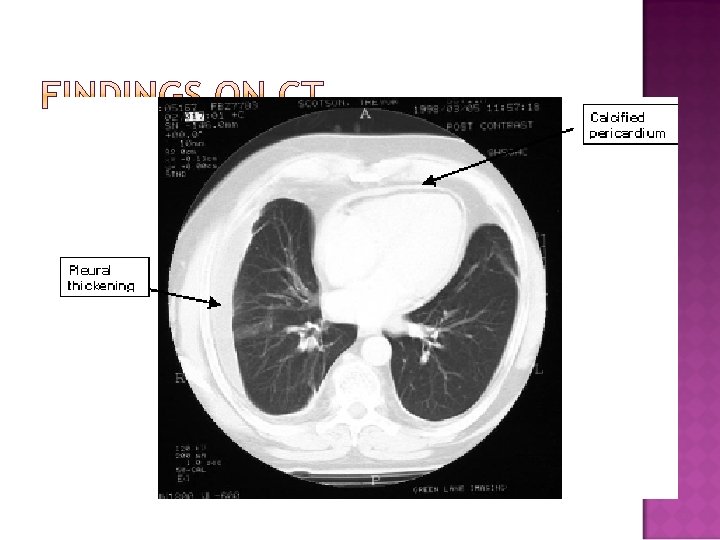
� Sudden inc in size of cardiac silhouette w/o specific chamber enlargement � Effacement of the normal cardiac borders � Development of a “flask” or “H 2 O-bottle” shaped heart
�May have (+) fat pad sign �Separation of mediastinal / retrosternal fat and epicardial fat by > 2 mm
Normal in patients with acute pericarditis unless pericardial effusion is present Enlarged cardiac silhouette Requires 200 cc of fluid
� If mild, can sometimes tx w/ medical mgmt � Including 1 or more of the following: NSAIDs, Colchcine, and/or steroids, depending on the suspected cause. � Require very close monitoring, including w/ serial TTEs and/or RHC
� Most require urgent/emergent pericardiocentesis Closed pericardiocentesis � Open Pericardiocentesis in the OR � � Generally in cath lab but can be at bedside Subxiphoid approach under echo guidance is most common - minimizes risk & can assess completeness of fluid removal Can alternatively use Fluoroscopic guidance Pigtail catheter often left in place May be best for loculated effusions, effusions containing clots or fibrinous material, and/or effusions that are borderline in size Allow for bx and creation of a pericardial window for recurrent effusions Bedside pericardiocentesis if pt is in extremis
� 16 - or 18 -gauge needle inserted at angle of 30 -45° to the skin, near the left xiphocostal angle, aiming toward the L shoulder