Acute Pelvic Pain Barbara Plovie MN ARNP BC

Acute Pelvic Pain Barbara Plovie, MN, ARNP, BC April, 2011

LEARNER OBJECTIVES n Identify acute pelvic pain as an urgent patient complaint. n Apply universal and etiology specific subjective, objective, assessment, and plan to at least two case studies. n Access acute pelvic pain standard of care resources.

CHIEF COMPLAINT Perforation or ischemia n Rapid onset n Colic/cramping Muscular contraction or obstruction n Entire abdomen Reaction to an irritating fluid in the peritoneum n Referred pain Pelvic organ innervation Berek (2007) .

PELVIC NERVES n Abdominal wall n Lower abdominal wall, lower back, vulva n Pelvic floor n Uterus, cervix, broad ligament, bladder n Ovaries, fallopian tubes n T 12 – L 1 n L 1 – L 2 n S 2 – S 4 n T 11 – L 2 and S 2 – S 4 T 11 – L 2 Berek, n

UNIVERSAL SUBJECTIVE GYN HX n n n n Menstrual, LMP Bleeding, discharge Contraception Sexual activity Gyn infections Pregnancy/Infertility Gyn/medical diagnosis PAIN HX n n n How and when started Intermittent/constant Dull/sharp/crampy Scale 1 to 10 GI sx Urinary sx Berek (2007); Barnhart (2008)

UNIVERSAL OBJECTIVE n n n Vital signs Urine h. CG, UA, CT/GC, ? culture Abdominal exam CVA tenderness Pelvic exam Wet mount

A DAY IN THE LIFE www. artdiamondblog. co m

TWILIGHT 16 yo accompanied by her mother c/o abdominal pain x 24 hours. Twilight denies nausea or vomiting and can’t remember her LMP. Missy also denies sexual activity and feels that her mother is over reacting. Missy wants to get back to school. WHAT ELSE DO YOU WANT TO KNOW?

WHAT IS YOUR DIFFERENTIAL? Pulse elevated n Hct = 34% n Sed rate WNL n Urinalysis WNL n Urine h. CG is positive n Twilight refuses a pelvic exam n Abdominal exam reveals diffuse lower pelvic pain, normal bowel tones, no CVA tenderness n

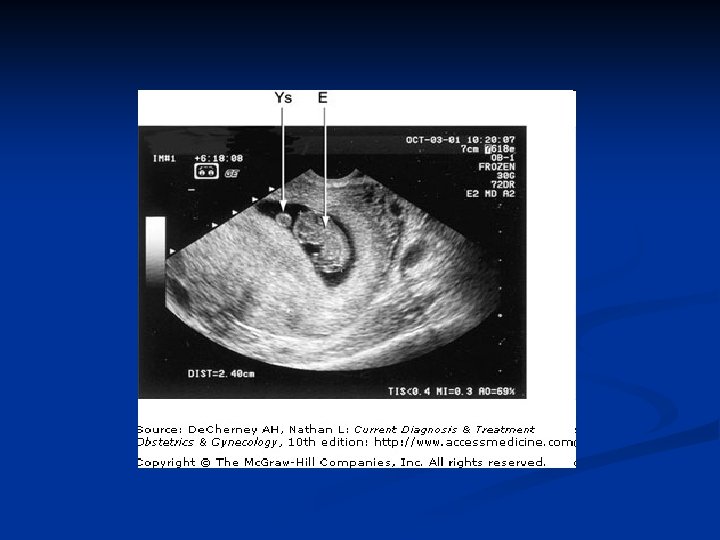
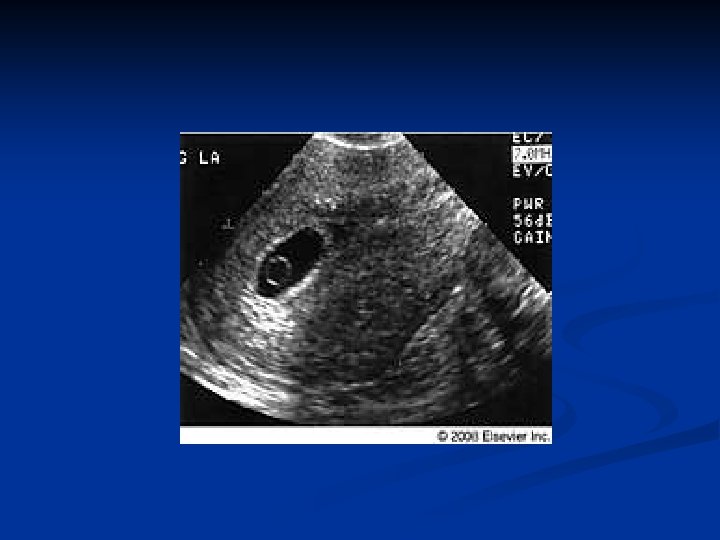
PREGNANCY Transvaginal Ultrasound Prenatal labs Viable IUP Intrauterine sac Ectopic

VIABLE IUP Objective n n Urine culture CBC Sed rate Abd ultrasound Differential n n n n UTI Kidney, ureters Appendicitis Cholilithiasis PID Musculoskeletal Ovarian cyst

INTRAUTERINE SAC Objective Quantitative h. CG n Repeat h. CG 48 hrs n Repeat U/S n ? Progesterone n Differential Ectopic n Early IUP n Blighted ovum n Ectopic and abortion precautions

ECTOPIC PREGNANCY

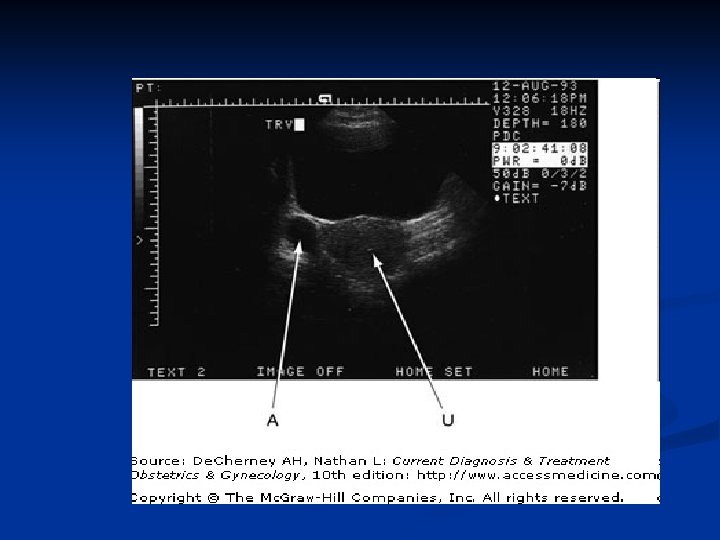
ECTOPIC ETIOLOGY n Tubule pathology SUBJECTIVE n Universal subjective n Triad 50% accurate Amenorrhea n ? IUD ACOG (2005); Berek (2007) Bleeding Pain

OBJECTIVE n Universal objective n Quantitative h. CG n Progesterone n Ultrasound n Repeat h. CG 48 hours n RH status if bleeding n Consider: CBC, sed rate ACOG (2008); Berek (2007)

SURGERY D&C Laparoscopy Hemodynamically unstable -orn Mass > 3. 5 cm -orn Cardiac motion n < 50% h. CG 48 hrs -andn h. CG < 2000 -andn Indeterminate U/S n Berek (2007)

Medical Management n Method of action n Indications n Contraindications n Single, two dose, multiple dose

METHOTREXATE DAY 1 Stat h. CG plateau or rising n Serum creat, CBC, SGOT, Blood type, RH n Methotrexate dose 50 mg/meter sq IM n D/C folic acid, NSAIDs, ETOH, sunlight n Administer Mic. Rhogam if known RH n

DAY 4 n Repeat h. CG and HCT DAY 7 h. CG, CBC, SGOT n Repeat MTX dose if < 15% fall in h. CG n Follow up h. CG every 2 -3 days initially n Then h. CG wkly until non-pregnant value n Contraception x 2 mo ACOG (2008) n

TWILIGHT IS PREGNANT DIFFERENTIAL NEXT STEP n Viable IUP n Abdominal U/S n Threatened AB n Depending on U/S, n Ectopic serum h. CG n Refer for care n Ovarian cyst Confidentiality!

GYNECOLOGIC PAIN INFECTION PID OVARY CYST TUBAL ABSCESS NON GYN TORTION SIMPLE HEMORRHAGIC

CHAU Chau thinks that she has the flu. She is c/o cramping lower abdominal pain that seems to be worsening as the day goes on. She’s now feverish and she is becoming nauseous. Her LMP was one week ago. She’s had multiple abdominal surgeries due to a car accident and doesn’t know if she has an appendix or not. WHAT ELSE DO YOU WANT TO KNOW?

WHAT IS YOUR DIFFERENTIAL ? Temp 100 F, P elevated, BP WNL n WBC slightly elevated n Sed rate slightly elevated n Abdominal exam compromised due to multiple incisions and pt body habitus, some diffuse pain, no rebound tenderness n No CVA tenderness n + vaginal amine odor noted, + clue cells n

PEVIC INFLAMMATORY DISEASE www. cmdrc. com/Data/Images/Female 1. jpg

PID ETIOLOGY Ascending infection with inflammation n 50% CT/GC, 50% other n SUBJECTIVE Lower abdominal pain n Vaginal discharge n Abnormal bleeding n Fever/chills n Urinary sx n MAY BE ASYMTOMATIC Berek (2007)

MINIMUM CRITERIA If no other cause of symptoms identified and Cervical motion tenderness -OR- Uterine tenderness -OR- Adnexa tenderness
 Discharge WBC on")
ADDITIONAL CRITERIA n n n Temp >101 F (38. 3 C) Discharge WBC on wet mount Sed rate C-reactive protein CT or GC confirmed CDC (2008)

CDC GUIDELINES Ceftriaxone 250 mg IM single dose ORCefoxitin 2 g IM + probenecid 1 g po OROther third generation cephalosporin IM plus Doxycycline 100 mg po bid x 14 days with or without Metronidazole 500 mg po bid x 14 days

ALTERNATIVE assume community and pt risk of GC is low Levofloxacin 500 mg po dly x 14 days OR Ofloxacin 400 mg po bid x 14 days with or without Metronidazole 500 mg po bid x 14 days Note: regimens with a quinolone agent are no longer recommended for PID

FOLLOW UP n Pelvic rest n Partner exam n 3 days post dx n 7 to 10 days post dx n STD test of cure n Prevention & contraception Marrazzo, et al. (2007); Berek (2007); Youngkin & Davis (2004)

HOSPITALIZE n Surgical emergency n Pregnancy n Severe illness n Cannot use oral antibiotics n Tubo-ovarian abscess CDC (2008)

CHAU has PID n RX according to CDC guidelines and pt med allergy hx n Probable bacterial vaginosis n Add oral metronidazole n Follow up visit in 3 days

NALALIA Natalia left her daughter’s soccer practice due to a strong vaginal odor she was sure everyone else could smell. Pt is just finishing her menses and is surprised that she is still cramping. She is distraught and needs to return to soccer practice before her daughter misses her. WHAT ELSE DO YOU WANT TO KNOW?

WHAT IS YOUR DIFFERENTIAL ? Vitals WNL n Pt refuses blood draw n Urinalysis WNL n Negative h. CG n WBC on wet mount n Normal abdominal exam, no CVA tenderness n Pelvic exam reveals retained tampon n Bimanual exam WNL n

NATALIA is at risk for PID Can RX as though pt has PID n Or, RX Doxycycline 100 mg bid x 7 days n Give PID and toxic shock precautions n Pelvic rest x 7 days n Follow up by phone n Note: Reassure pt re frequency of retained tampon in normal Gyn practice n

TUBO-OVARIAN ABSCESS ETIOLOGY n Sequela of acute salpingitis n Usually bilateral, can be unilateral SUBJECTIVE n Pain and temp > 7 days n PID sx Berek (2007)

OBJECTIVE BILATERAL EXAM Tender n Firm n Fixed bilateral masses n ULTRASOUND Confirm diagnosis n Indeterminate Laparoscopy n Hospitalize (Berek, 2007)

www. gfmer. c h

ASHONTI Ashonti is accompanied by her husband. She called him home from work with sudden onset sharp, debilitating right lower quadrant pelvic pain. By the time Adam got home, the pain subsided. The couple was concerned and decided to come in. Ashonti’s LMP was three weeks ago. The couple is planning pregnancy. WHAT ELSE DO YOU WANT TO KNOW?

WHAT IS YOUR DIFFERENTIAL ? Vitals WNL n CBC WNL n Sed rate WNL n Urinalysis WNL n Wet mount WNL n h. CG negative n Abdominal exam reveals mild right lower quadrant pain, no CVA tenderness n Pelvic exam is WNL with some diffuse left adnexa pain n

ASHONTI RUPTURED A CYST n Ashonti is now off hormonal contraception which may inhibit ovarian cysts n Offer an abdominal and transvaginal U/S to verify your diagnosis n Follow up by phone

FUNCTIONAL OVARIAN CYSTS

OVARIAN CYST ETIOLOGY Physiologic n Follicular or corpus luteum n Simple or hemorrhagic n SUBJECTIVE Adolescence n Sudden onset of pain, ? unilateral n Luteal phase n Generalized abdominal pain n Dizziness, faint, nausea Berek (2007) n

OBJECTIVE INTACT Unilateral enlarged n Moveable n Unilateral tenderness n Ultrasound n RUPTURED ? Enlarged n Moveable n Unilateral tenderness n Diffuse dull pain n www. ovariancystfree. com

SIMPLE OVARIAN CYST gynaecologist 4 u. co m

HEMORRHAGIC CYST radiology. rsnajnls. or g

HEMOPERITONEUM OBJECTIVE n n n Vital signs Distended abdomen Rebound tenderness Ultrasound CBC, sed rate, blood type & RH

ZAMINA Zamina is 17 yo and accompanied by her gym coach and father. Morgan doubled up in pain during competition. She has amenorrhea during gymnastics season according to her father. Zamina is in too much pain to answer any questions. This is an emergency and the aid car is ten minutes away. What would you do for Morgan during that ten minutes?

R/O OVARIAN TORTION n Abdominal U/S with color flow n While it is tempting to initiate an IV and draw blood, the medics can perform these procedures in the aid car. They cannot perform an U/S.

TORTION GYN ETIOLOGY n n Benign cystic teratoma Polycystic ovary SUBJECTIVE n n Rapid onset pelvic pain Severe and constant -or- intermittent Lifting, exercise, intercourse Autonomic reflexes (nausea, emesis, anxiety) Berek (2007)

OBJECTIVE n Mild temp n CBC, sed rate mild leukocystosis n Abdominal tenderness n Lower localized rebound tenderness n Large unilateral pelvic mass ORDER U/S with DOPPLER FLOW

www. gfmer. ch
")
Voget (2006)

BELLA While she is there, Bella’s mom, Monica would like to be seen for central lower pelvic pain that she’s had on and off for the past two weeks. She has seen her primary care provider with no relief. Bella is post menopausal and has no medical insurance. WHAT ELSE DO YOU WANT TO KNOW?

WHAT IS YOUR DIFFERENTIAL? Vitals WNL n CBC WNL n Sed rate WNL n Urinalysis low specific gravity, + blood, +WBC n Wet mount WNL n Abdominal exam reveals low central pelvic discomfort, no CVA tenderness n Pelvic exam no CMT, adnexa right and left not felt, low central pelvic pain, no fundal tenderness n

BELLA has a UTI n Don’t let the UA fool you. Monica has been pushing fluids n Urine culture n At risk for pyelo due to length of sx n RX with broad-spectrum generic antibiotic for at least one week

NON GYN CONTINUE WORK UP n Urine culture n Abdominal ultrasound n CT with contrast n Consult n ? Refer

SUMMARY n Same day appointment n Universal objective at check-in n Arrange ultrasound n Consult as necessary n Follow up

DON’T CHASE ZEBRAS media. gmu. edu

CLINICAL CUUNDRUM Adeena is a 16 yo who presents with her mother for an ER follow up visit. Adeena was in the ER three days ago with a c/o pelvic pain. U/S at that time revealed a right collapsing hemorrhagic cyst. Adeena’s mother brings a copy of the ER visit and U/S report. Adeena’s pain has now resolved. You prescribe birth control pills for cyst suppression and schedule an U/S in 8 weeks for follow up. media. gmu. edu

TWO WEEKS LATER Adeena’s pain has not resolved. Her father initially refused to have his daughter on birth control pills. The father now consents to initiating BCP. FOUR WEEKS LATER Four weeks later, Adeena returns to clinic after missing three days of school due to pelvic pain. She is taking the birth control pills continuously as prescribed. She has a negative pregnancy test. All labs WNL. media. gmu. edu

profile. myspace. co m
- Slides: 65