Acute Pain management in the Opioid dependent patient


")















 Crombie IK, Davies HT, Macrae WA Cut and thrust:")



: 32 -9 (2008)")


 Acetaminophen and NSAIDs if")





- Slides: 34
Acute Pain management in the Opioid dependent patient Siva Raghavan MD FRCA FFPMRCA FRCPC
Outline § Acute pain management in opioid dependent patients can be very challenging § Universal agreement is lacking § Recent APS post-operative pain management guidelines § Chronic post surgical Pain and strategies to minimize it § Opioid prescription and crisis in the community
Acute pain management: Scientific evidence 4 th edition (ANZCA and FPM Australia)
OPIOID DEPENDENT PATIENT COMING FOR SURGERY Patient’s fears: - Fear of withdrawal symptoms - Fear of under-treatment due to prejudice - Fear of being perceived as “manipulative” Clinician’s concerns: - Pain management can be very challenging - Analgesic requirements can be high due to opioid tolerance and opioid induced hyperalgesia - Inadequate pain control: RS/ CVS complications and hospital stay Concern about overtreatment of pain and respiratory depression Reports of pain may be fabricated Diversion of prescription opioids
Opioid dependence vs Addiction • Tolerance and withdrawal is not addiction. They are features of opioid dependence • Addiction (Opioid use disorder): (Psychological dependence) - Strong desire to take the drug - Difficulty in controlling its use - Persistent use despite being aware of harmful consequences - High priority given to drug use than to other activities § Most of the chronic pain patients are opioid dependent but not addicts
Common misconceptions Maintenance opioid therapy provides adequate analgesia X - Maintenance opioids need to be continued to prevent withdrawal - Additional opioids are needed to manage acute pain. - These patients need more opioids than opioid naive patients due to tolerance and opioid induced hyperalgesia Additional opioids for analgesia cause addiction relapse X - Unrelieved pain is a risk factor for relapse of addiction
Common misconceptions Additional opioids cause respiratory and CNS depression X - Opioid dependent patients have tolerance to respiratory and CNS depression PCA is inadequate in opioid tolerant patients X -Besides regional anesthesia, PCA is the best option for opioid-tolerant patients. Long acting opioids give better pain control X - Long acting opioids have higher incidence of unintentional overdose and are not recommended in opioid naïve patients.
Peri-operative opioid dosing Example 1: 59 year old man with chronic arthritic pains, on Morphine sulphate 90 mg q 12 h coming for a total knee replacement Allow MST 90 mg PO q 12 h to prevent withdrawal. Use short acting morphine/hydromorphone/oxycodone for acute pain
Peri-operative opioid dosing Example 2: 59 year old man with gastric cancer and chronic arthritic pains, on Morphine sulphate 90 mg q 12 h coming for Total gastrectomy. Patient refuses epidural analgesia.
OPIOID CONVERSION
Peri-operative opioid dosing Example 2: IV PCA will be a good choice for this patient 180 mg PO morphine = 60 mg iv morphine= 12 mg iv hydromorphone Partial cross tolerance allows 50% reduction in dose when switching opioids. Hence 180 mg/d PO morphine = 6 mg/d iv hydromorphone Run a PCA background infusion of hydromorphone @ 0. 25 mg/hr to prevent withdrawal Program bolus (0. 2 to 0. 4 mg) with lock out interval (5 -10 min) for acute pain
Peri-operative opioid dosing Example 3: 59 year old man with previous H/O substance use disorder, currently on methadone 80 mg/d. Methadone conversion is challenging due to long half life and high inter-patient variability in pharmacokinetics. Use conversion tables to guide you (conversion is complicated) ALWAYS USE LOWER DOSES AND TITRATE
Peri-operative opioid dosing Example 3: If able to take oral meds- continue Methadone 80 mg/d PO and give short acting opioid for acute pain If unable to take oral meds: - Oral methadone to iv morphine conversion is approx 2: 1 - IV morphine equivalent= 40 mg/d - 50% dose reduction ------- 20 mg/d morphine - Program PCA morphine with 1 mg/h background infusion (24 mg/d) - PCA bolus 1 mg with 5 minute lockout interval for acute pain
Peri-operative opioid dosing Example 4: Patient on buprenorphine / suboxone Problems: Partial μ agonist and κ antagonist Ceiling effect with analgesia High affinity to opioid receptors κ-receptor antagonism interferes with other opioids Broad inter-patient half life variability (24 -60 h)
Peri-operative opioid dosing Example 4: Patient on buprenorphine / suboxone - If on a low dose and severe pain is not anticipated, continue maintenance buprenorphine dose and use short acting opioid for acute pain - For major elective surgery, convert to oral morphine or methadone pre-op. Discontinue buprenorphine at least 72 h prior to surgery. Use opioid sparing adjuncts - For emergency surgery, use PCA morphine with background infusion (high doses may be needed). Use Opioid sparing adjuncts. Will need to be in a monitored setting (ICU)
Guidelines u Education: • Preoperative education- Patient and familycentered, individually tailored education • Parents and adult-caregivers should be educated about developmentally appropriate methods to assess pain and pain management options • Education to patients and primary caregivers on pain treatment plan and medication tapering after discharge
Patient education: Establish Clear goals Managing pain appropriately does not mean having “zero pain” Some ongoing pain is normal. Encourage mobility Talk about expected duration of use of opioids after surgery. Talk about “opioid sparing” pain relief strategies
Guidelines u Assessment: • Conduct pre-op evaluation of medical and psychiatric comorbidities, medications, history of chronic pain, substance abuse, previous response to analgesics • Use a validated pain assessment tool to track responses and adjust treatment plans. • Do not rely solely on “objective” measures like vital signs or pain-related behaviors • Adjust the pain management plan on the basis of adequacy of pain relief and presence of adverse events
Chronic post surgical pain (CPSP) Crombie IK, Davies HT, Macrae WA Cut and thrust: antecedent surgery and trauma among patients attending a chronic pain clinic. Pain. 1998; 76(1 -2): 167 -71 • 5130 patients, 10 outpatient clinics in North Britain • Surgery contributed to pain in 22. 5% of patients Macrae WA, Davies HTO. Chronic postsurgical pain. In: Crombie IK, Linton S, Croft P, Von Korff M, editors. Epidemiology of pain. Seattle: IASP Press; 1999. p. 125– 42. Definition of CPSP Pain after a surgical procedure that lasts for at least two months and other causes of pain have been excluded (eg, continuing malignancy, chronic infection)
2017 - IASP Global year against pain after surgery Current definition of CPSP Pain after a surgical procedure or increased after the surgical procedure At least 3 months’ duration with significant negative effect on QOL Pain is a continuation of acute post-op pain or may develop after an asymptomatic period Pain is localized to the surgical field or to a referred area (dermatome) Other possible causes have been excluded (eg, infection, cancer recurrence) Patricia Lavand’homme, PAIN 158(2017): S 50 -S 54
Chronic Post Surgical Pain
PATHOGENESIS OF CHRONIC POST-SURGICAL PAIN
Functional MRI – Neuroanatomy of pain processing Irene Tracey, BJA 101(1): 32 -9 (2008)
Risk factors for CPSP
Strategies to reduce Chronic post-surgical pain u Consider the indications for surgery u Minimally invasive surgical techniques u Good treatment of acute pain u Regional anesthesia (epidurals, spinals, nerve blocks, local infiltration) u Drugs affecting central sensitization- ketamine, gabapentin, pregabalin u (2 weeks’ perioperative treatment with pregabalin reduced neuropathic pain 3 months and 6 mths after TKR from 9% and 5% respectively to 0) Buvanendran et al, Anesth Analg 2010
u • • • Multimodal “opioid sparing” analgesia (APS guidelines) Acetaminophen and NSAIDs if there are no contraindications Gabapentin / pregabalin iv ketamine (0. 25 -0. 35 mg/kg bolus, 0. 1 -0. 5 mg/kg/h infusion) iv lidocaine (5 mg/kg infusion over 1 h) Subcutaneous/ intra-articular infiltration of local anesthetic Peripheral nerve blocks, continuous perineural LA infusions Neuraxial techniques: Spinal, epidural, combined spinal epidural Intrathecal and epidural opioids Clonidine as adjuvant in regional anesthetic techniques Oral opioids preferred over iv in people who can use the oral route Long acting opioids not recommended unless patient is already on long acting opioids before surgery
Treat acute pain aggressively BUT Remember there is a problem with opioids in the community
Problems with long term opioids u. Patients who used opioids for at least 90 days were more than 60% likely to still be on chronic opioids in 5 years (Martin et al. J Gen Intern Med 2011; 26: 1450 -7) u. Receiving one week supply of >2 opioid prescriptions after an acute back sprain is associated with a doubling of the patients’ risk for long term disability (Franklin et al. Spine 2008; 33: 199 -204) u. The goal of opioid therapy is to prescribe the briefest, least invasive and lowest dose regimen that minimizes pain and avoids dangerous side effects (Hegmann et al. J Occup Environ Med 2014; 56: e 143 -59; Bates et al. J Urol 2011; 185: 551 -5)
Source of abused prescription pain killer CDC 2011
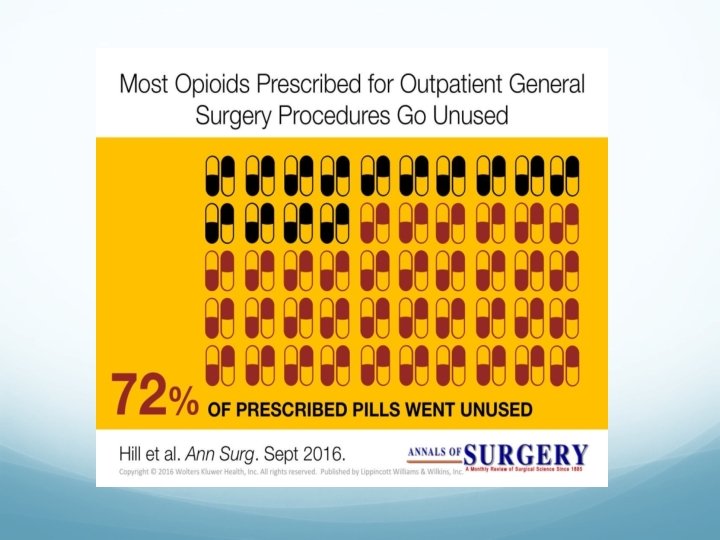
Excessive post-op opioid prescription • Opioid consumption following outpatient upper extremity surgery. Rodgers J, Cunningham K, Fitzgerald K, Finnerty E J Hand Surg Am. 2012 Apr; 37(4): 645 -50 67% of pills unused • Prescription Opioid Analgesics Commonly Unused After Surgery: A Systematic Review. Bicket MC, Long JJ, Pronovost PJ, Alexander GC, Wu CL JAMA Surg. 2017 Nov 1; 152(11): 1066 -1071 42% to 71% of prescribed opioids went unused In 2 studies examining storage safety, 73% to 77% of patients reported that their prescription opioids were not stored in locked containers
ACUTE PAIN MANAGEMENT IN THE OPIOID DEPENDENT PATIENT SUMMARY 1. Identify opioid user and abuser. Do not be judgmental 2. Consider comorbidities 3. Ensure baseline opioid requirements to prevent withdrawal 4. Provide effective analgesia and treat acute pain aggressively 5. Use multimodal analgesia 6. Prefer local and regional analgesia when suitable 7. Use strategies to minimize Chronic post-surgical pain 8. Do not induce weaning in the immediate perioperative period 9. Be mindful of the consequences of excessive opioid prescription