Acute Leukemia Rakesh Biswas MD Professor Department of

Acute Leukemia Rakesh Biswas MD, Professor, Department of Medicine, People's College of Medical Sciences, Bhanpur, Bhopal, India

A 16 year old girl Extreme pallor gum bleeds, Purpura, With Lymphadenopathy and Hepatosplenomegaly

Possible causes: Investigations and treatment

Only a week later, D was ill again, with a fever, severe headache, and extreme lethargy.

During a sunny spring weekend, D would go outside to play, only to return minutes later exhausted, flopping herself onto the sofa to rest

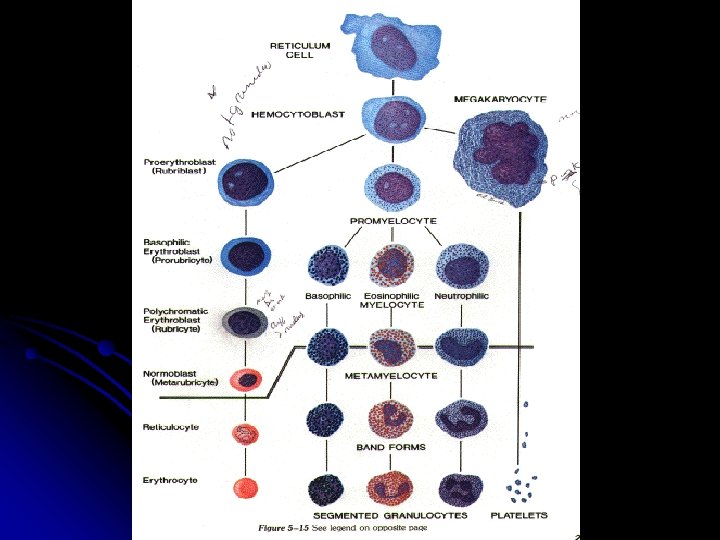
Leukemia Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood

Once inside the van and on our way out of the clinic parking lot, she asked, "Dad, what is leukemia? " "Can I die from this? "

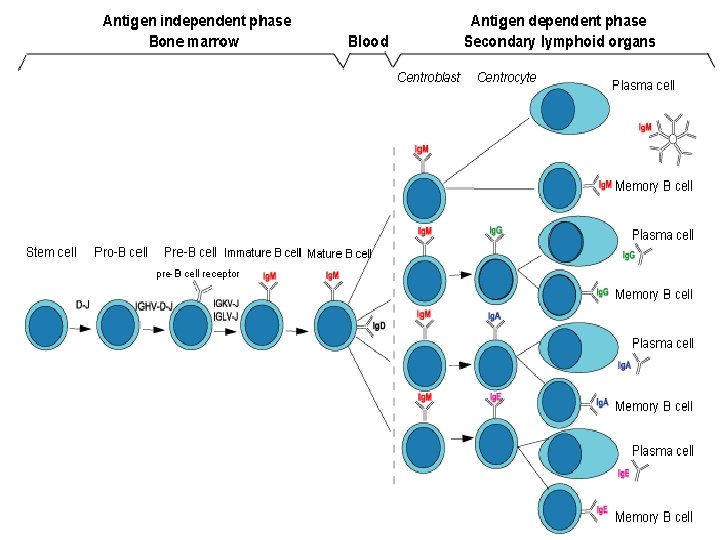
Classification Classified based on cell type involved and the clinical course l 1. Acute : l ALL l AML l 2. Chronic : l CLL l CML
 l B-cell l T-cell l Undifferentiated")
Subclassification l ALL l Common type( pre-B) l B-cell l T-cell l Undifferentiated

After the oncologist performed a bone marrow aspiration to confirm the diagnosis of leukemia, we learned specifically what type it was and the count. "D had acute lymphoblastic leukemia, early pre-B cell.

Myelomono
 Classification M 0: Minimally differentiated leukemia M 1: Myeloblastic leukemia without")
AML French-American-British (FAB) Classification M 0: Minimally differentiated leukemia M 1: Myeloblastic leukemia without maturation M 2: Myeloblastic leukemia with maturation M 3: Hypergranular promyelocytic leukemia M 4 Eo: Variant: Increase in abnormal marrow eosinophils M 4: Myelomonocytic leukemia M 5: Monocytic leukemia M 6: Erythroleukemia (Di. Guglielmo's disease) M 7: Megakaryoblastic leukemia Ref-Harrison’s Principle of Internal Medicine

l CLL l B-cell: common l T-cell: rare

l CML l Ph +ve l Ph –ve, BCR-abl -ve l Eosinophilic Leukemia l l Ph: Philadelphia chromosome BCR: Breakpoint cluster region; abl : Abelson oncogene
 l Malignant transformation of a myeloid precursor cell ;")
Acute Myeloid Leukemia ( AML) l Malignant transformation of a myeloid precursor cell ; usually occurs at a very early stage of myeloid development l Rare in childhood & incidence increases with age

Etiology Unknown / De-novo !! In majority Predisposing factors: l Ionizing radiation exposure l Previous chemotherapy : alkylating agents l Occupational chemical exposure : benzene l Genetic factors: Down’s Syndrome, Bloom’s, Fanconi’s Anemia l Viral infection ( HTLV-1) l Immunological : hypogammaglobulinemia l Acquired hematological condition -Secondary

Epidemiology l M>F ALL which predominantly affects younger individuals l AML – adults and the elderly l Median age gp-65 yrs l l Geographical variation-none
")
Clinical features General : Onset is abrupt & stormy (usually present within 3 months) l Bone marrow failure (anemia, infection , bleeding) l Bone pain & tenderness

Specific: M 2 : Chloroma: -presents as a mass lesion ‘tumor of leukemic cells’ l M 3 : DIC l M 4/M 5 : Infiltration of soft tissues, gum infiltration, skin deposits , Meningeal involvement-headache, vomiting, eye symptoms l

")
Skin Infiltration with AML (Leukemia Cutis)

Diagnosis l Blood count : WBC usually elevated (50, 000 - 1, 000 / cmm ); may be normal or low; often anemia & thrombocytopenia l Blood film : (as above) Blast cells

P. Smear AML
, l")
l Bone marrow aspirate & trephine: Hypercellular, l blast cells ( > 20%), l presence of Auer rods - AML type l Cytochemistry : Special stains to differentiate AML from ALL ; Positivity with Sudan black & Myeloperoxidase (MPO) in AML

Jemshidi trephine & Salah aspiration needle

Auer Rods in Leukemia cells
 & Sudan black (left) showing intense localised positivity in blasts")
MPO (right) & Sudan black (left) showing intense localised positivity in blasts

l Confirmation: l Immunophenotyping l Molecular genetics l Cytogenetics: Chromosomal abnormalities

Other Inv: Coagulation screen, fibrinogen, D- dimer l RFT, LFT l LDH, Uric acid l Urine l CXR l ECG, ECHO l

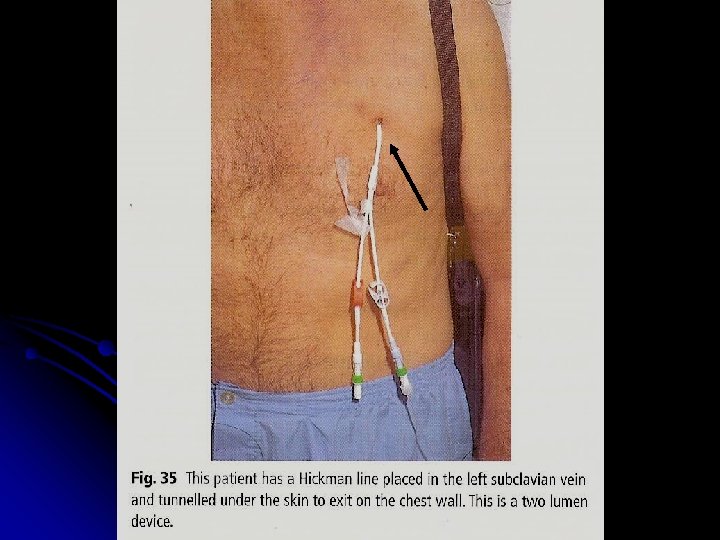
Management I. Supportive care : Anemia – red cell transfusion l Thrombocytopenia – platelet concentrates l Infection – broad spectrum IV antibiotics l Hematopoietic growth factors : GM-CSF, G-CSF l Barrier nursing l Indwelling central venous catheter l

l Metabolic problems : Monitoring hepatic / renal / hematologic function; Fluid & electrolyte balance, nutrition Hyperuricemia- hydration, Allopurinol l Psychological support

The white blood cell count in her peripheral blood was about 550, 000. Her bone marrow was packed with leukemia blasts. "

The next thing that occurred was a procedure called leukopheresis. This procedure lasted 4 hours and cut D’s white blood cell (WBC) count in half--to about 250, 000.

She was administered chemotherapy immediately following the leukopheresis procedure. The next day we learned that the chemo had produced an effect as well: The WBC had halved again--125, 000.
 vincristine, prednisone, anthracycline, (idarubicin or daunorubicin)")
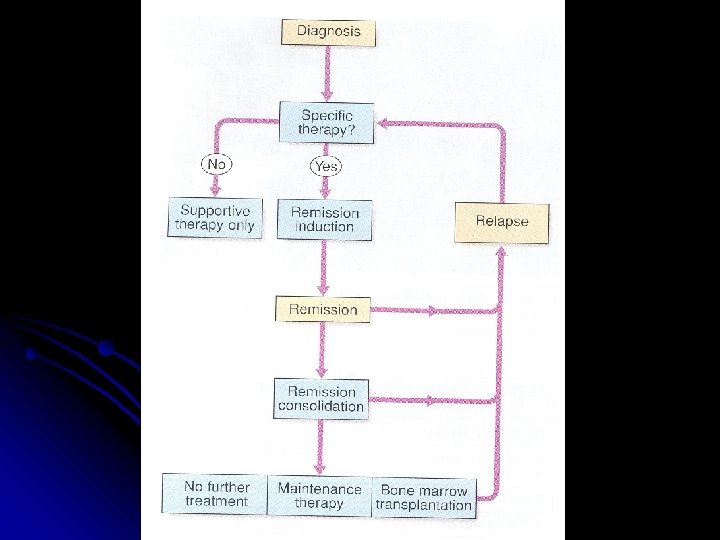
SPECIFIC THERAPHY: Chemotherapy : Induction: (4 -6 wks) vincristine, prednisone, anthracycline, (idarubicin or daunorubicin) cyclophosphamide, and L-asparaginase
.")
Consolidation: (multiple cycles of intensive chemotherapy given over a 6 to 9 month period). Cytosine arabinoside, high-dose methotrexate, etoposide anthracycline, (idarubicin or daunorubicin)
. LPs with intrathecal MTX every 3 months, Monthly")
Maintenance phase: (18 to 24 months). LPs with intrathecal MTX every 3 months, Monthly vincristine, Daily 6 -MP, and weekly MTX.

At day 29 of the induction protocol D was declared to be in complete remission. We were all relieved with this news.

Step two was the next phase of treatment called consolidation therapy. This entailed multiple combinations of drugs administered on a rotational basis (on various weeks) for the next six months.

For instance, she would receive an infusion of methotrexate for a couple of days and then take 6 MP by mouth for a week. Another cycle included VM-26 (Teniposide) and Ara-C.
: < 5% blast cells in normocellular bone marrow l")
l Complete remission ( CR): < 5% blast cells in normocellular bone marrow l Autologous BMT : Can be curative in younger patient (< 40 -50 yrs)

Exactly 5 months since her diagnosis, and 16 weeks of remission… "We're at the clinic. D has relapsed. Her white count is 27, 000. "

The Consolidation protocol had been dropped and replaced with a new induction protocol. After the bone marrow aspiration to determine the extent of the leukemia relapse, she was given doxirubicin, vincristine and L-asparaginase.

For several days following D‘s discharge from the bone marrow transplant unit, all of us loaf around the house and recuperate from our 90 day marathon…

…the first 30 days representing Ds' relapse and the induction therapy to obtain a second remission

Back in fighting form, D proceeds directly to the final 30 days of the marathon--the actual bone marrow transplant. BMT patients are in a delicate condition following discharge

Looking back, the nine weeks or so--the post BMT discharge period--was a sublime time for us. D was home and was feeling pretty good.

As D’s hair began to grow again, we rubbed her head every night at the dinner table, wondering what color it was going to be or if it was going to be curly or straight. We never found out.

On Monday, March 1, 1999 we went to clinic and waited for the lab results. The results came back as we feared. D had relapsed. Her white count was 47, 000. We were devastated.

l III. PALLIATIVE THERAPHY l Chemo, RT, Blood product support

Prognosis Median survival without treatment is 5 weeks l 30% 5 -yr survival in younger patients with chemotherapy l Disease which relapses during treatment or soon after the end of treatment has a poor prognosis l

Poor prognostic factors Increasing age l Male sex l High WBC count at diagnosis l CNS involvement at diagnosis l Cytogenetic abnormalities l Antecedent hematological abnormalities (eg. MDS) l No complete remission l

Two things that I will always remember about D: She was a collector of many things, trinket boxes, key rings. But she was first and foremost a collector of "FRIENDS. "

Among other things, she wrote: "Hair loss is a side effect of chemotherapy, and cancer is a side effect of life. "

Summary; Learning Points

THANK YOU
- Slides: 60