ACUTE LEUKEMIA Definition PB andor BM blasts 20
")
ACUTE LEUKEMIA Definition PB and/or BM blasts > 20 % of nucleated cell (NC) count
 n Clonal proliferation and accumulation of blast cells in blood,")
Acute lymphoblastic leukemia (ALL) n Clonal proliferation and accumulation of blast cells in blood, bone marrow and other organs n Disorder originates in single B or T lymphocyte progenitor n Heterogenous disease with different biological subtypes n Incidence in adults : 20% of acute leukemias n Etiology - unknown

clinical features 1. Bleeding 2. Fever/infection 3. Bone/joint pain 4. Hepatomegaly 5. Splenomegaly 6. Lymphadenopathy 7. CNS involvement
 are at higher risk")
Patients with very high WBC counts (> 100, 000/mm 3) are at higher risk for tumor lysis syndrome and leukostasis, both of which are considered oncologic emergencies and require prompt recognition and management. Tumor lysis syndrome can be due to spontaneous or treatment-mediated cell destruction and is characterized by hyperuricemia, renal failure, acidosis, hypocalcemia, and hyperphosphatemia. [Jabbour 2005 b

• Manifestations of leukostasis include dyspnea, chest pain, headache, altered mental status, cranial nerve palsies, and/or priapism.

laboratory findings 1. Blood examination - anemia, - thrombocytopenia, - variable leukocyte count, usually increased, - blood morphology: presence of blast cells 2. Bone marrow morphology - presence of blast cells, - suppression of normal hematopoiesis

Laboratory findings 3. Cytochemical stains 4. Immunophenotyping 5. Cytogenetics 6. Molecular studies
 L 1: small monomorphic L 2: large, heterogeneous L")
FAB Classification of ALL (1976) L 1: small monomorphic L 2: large, heterogeneous L 3: Burkitt cell-type

ACUTE LEUKEMIA Cytochemistry Precursor T-ALL B-ALL AML Myeloperoxidase - - + Sudan black - - + Nonspecific esterase (NSE) - - + with • Na fluoride inhibition M 5 • No Na fluoride inhibition M 4 Periodic acid. Schiff (PAS) +++ (coarse) - -ve to diffuse fine + Acid phosphatase - + -

Acute leukemia Mixed lineage Vs biphenotypic • Mixed lineage leukemia: Two different blast populations ALL AML • Biphenotypic leukemia: The same blast population both myeloid and lymphatic markers

EGIL* scoring system for biphenotypic leukemia *European Group for the Immunological characterization of Leukemia Score 2 1 0. 5 B-lineage T-lineage Myeloid lineage CD 79 a Cy Ig. M Cy CD 22 CD 3 (cy/m) Anti-TCR Anti-MPO Anti-lysozyme CD 19 CD 10 CD 2 CD 5 CD 8 CD 10 CD 13 CD 33 CD w 65 Td. T CD 24 Td. T CD 7 CD 1 a CD 14 CD 15 CD 64 CD 117 To diagnose biphenotypic leukemia, the score should be at least: 2 in the myeloid lineage + 2 in the lymphatic lineage

Acute leukemia ALL with myeloid coexpression Myeloid coexpression = at least 20 % of blasts + ve for at least one marker of: CD 13, CD 33, CD 65 s.
 Subtype Pro-B C-ALL Pre-B B-cell Td. T")
AL: Immunophenotyping ALL B-ALL (incidence = 76%) Subtype Pro-B C-ALL Pre-B B-cell Td. T + + + - CD 19 + + CD 10 Cy Ig. M + + + S Ig +
 Compartment T-cell type Positive markers Pro-T CD 7")
AL: Immunophenotyping ALL T-ALL (incidence =24%) Compartment T-cell type Positive markers Pro-T CD 7 Compartment I (early T) Pre-T CD 2 and/or CD 5 and/or CD 8 Compartment II Thymic T CD 1 a Compartment III Mature T s. CD 3
 (1) Precursor B-cell ALL (pro-B, C-ALL, pre-B):")
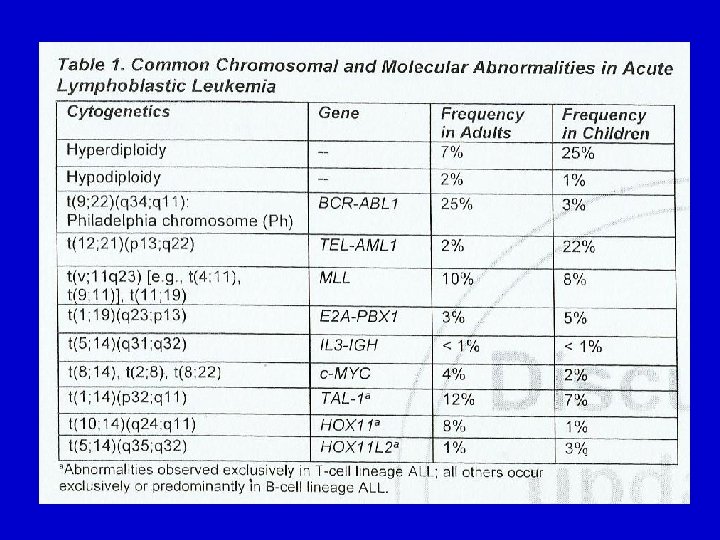
Acute leukemia WHO Classification of ALL (1999) (1) Precursor B-cell ALL (pro-B, C-ALL, pre-B): Ch abn. Fusion gene t (9; 22) BCR/ABL t (V; 11) e. g. t (4; 11) MLL rearranged e. g. MLL/AF 4 t (1; 19) E 2 A/PBX 1 t (12; 21) Tel/AML 1 (2) Burkitt–cell (mature B-cell) ALL: (3) Precursor T-cell ALL: (4) Mature T-cell ALL:
 *30% of adult ALL")
Cytogenetic classification of ALL Bad Prognosis • Ph-chromosome t(9; 22) *30% of adult ALL *3% of pediatric ALL Good Prognosis • t(12; 21) (Tel/AML 1) *30% of pediatric ALL • Hypoploidy • Hyperploidy (DNA index < 1. 12) (DNA index =1. 12 -1. 6) • t(4; 11)

Algorithm for diagnosis of AL Lymphoblastic lymphoma Clinically suspected + blasts in PB Morphology + cytochemistry of PB + BM < 20% blasts in BM ALL (L 1, L 2) ALL (L 3) AML < 20% blasts in BM Burkitt lymphoma Immunophenotyping B-lineage Pro-B C-ALL Pre-B T-lineage Mature B Early Thymic Cytogenetics / Molecular genetics t (4; 11) ALL 1/AF 4 t (9; 22) BCR/ABL Mature
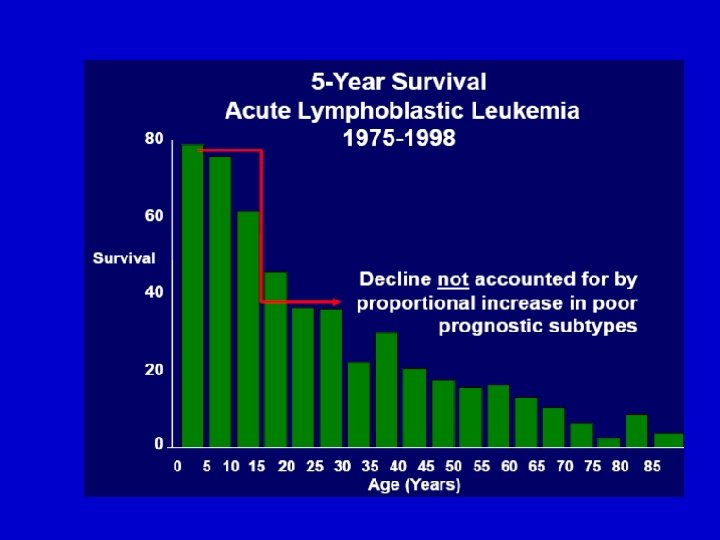

Acute Lymphoblastic Leukemia Outcome • High remission rates possible in adults and children • Leukemia-free survival in children 2 -10 years of age: 80% Most adults experience relapse Complete Leukemia. Remission Free Survival Adults Children (2 -10 yrs of age) 80% to 90% 35% 97% 80% Pui CH, et al. N Engl J Med. 2006; 354: 166 -178.

ALL: Typical Treatment • Induction, consolidation, maintenance phases – CNS prophylaxis with IT-MTX CNS Prophylaxis (IT-MTX) Induction 11/1/2020 Consolidation Maintenance Over a period of months 2 -3 years Free Template from www. brainybetty. com 21

• ALL therapy is one of the most complex types of anticancer programs. Multiple drugs are combined into regimen-specific sequences of various doses and durations. • The backbone of ALL induction regimens is a combination of vincristine, corticosteroids, and anthracyclines. This combination achieves complete remission rates of 72% to 92% with a median remission duration of approximately 18 months

Adult ALL: Large Clinical Trials N Age Treatment CR, % DFS, % GMALL 02/84 562 28 BFM 75 39 GMALL 05/93 1163 35 BFM, HD-ARA-C, HD-MTX 87 35 -40 CALGB 8811 198 35 BFM, ↑ Cy, ↑ ASP 85 36 CALGB 19802 163 41 BFM, ↑ Cy , ↑ DNR 78 35 GIMEMA 778 28 BFM ± Cy 82 29 MRC-UKALL XA 618 > 15 BFM + early intensification 89 -- MRC/ECOG 1521 BFM + HD-MTX ± SCT 91 38 UCSF 8707 84 BFM intensified 93 52 92 23 38 Hyper-CVAD 11/1/2020 288 27 Cy, D, AD, HD-MTX, HD 40 Free Template from ARA-C www. brainybetty. com
 At diagnosis Favorable Unfavorable Age 15 -20 yrs")
Prognostic factors in adult ALL (1) At diagnosis Favorable Unfavorable Age 15 -20 yrs >50 yrs WBC (B-lineage) <30 000/µL >30 000/µL • Pro B-ALL • Early T-ALL • Mature T-ALL Immunophenotype Thymic T-ALL Cytogenetics & Molecular genetics • Normal diploid • T(9; 22)/BCR-ABL karyotype (? ) • T(4; 11)/ALL 1 -AF 4 • Hyperdiploid karyotype (? ) 11/1/2020 Free Template from www. brainybetty. com 24
 Response to treatment Favorable Time to CR MRD")
Prognostic factors in adult ALL (2) Response to treatment Favorable Time to CR MRD after induction MRD during consolidation 11/1/2020 Unfavorable CR in 2 -4 ws CR >4 ws <10 -3 >10 -3 <10 -4 or negative >10 -4 or increasing Free Template from www. brainybetty. com 25

Risk-adapted treatment of ALL Age Risk <50 yrs 50 -60 yrs >60 yrs Standard-risk protocol COAP • No further treatment or risk only • Maintenance X 2 -3 yr or • Allogeneic BMT High risk High-risk protocol Mature 6 full blocks i. e. B-cell (A 1 B 1 A 2 B 2 A 3 B 3) • Maintenance X 2 -3 yr • No BMT • High-risk protocol with ABMT arm • No allo BMT COAP only 4 incomplete blocks (without HD MTX) i. e. a 1 b 1 a 2 b 2 + BMT 11/1/2020 Free Template from www. brainybetty. com 26
 Induction (phase I &")
Risk-adapted treatment procedure for adult ALL (other than mature B-ALL) Induction (phase I & II) CR Standard risk High risk Consolidation (phase I &II) MRD<10 -4 MRD >10 -4 Donor End of therapy Donor Allo BMT 11/1/2020 No donor Maintenance Free Template from X 2 -3 yrs www. brainybetty. com No donor HAM Allo BMT Auto BMT 27

2 Treatment of standard-risk group 11/1/2020 Free Template from www. brainybetty. com 28
 CR Consolidation (phase I &II)")
Treatment of standard-risk group Induction (phase I & II) CR Consolidation (phase I &II) MRD>10 -4 MRD<10 -4 Donor End of therapy 11/1/2020 Allo BMT Free Template from www. brainybetty. com No donor Maintenance X 2 -3 yrs 29

Induction treatment of standard-risk group L-Asparaginase 5000 U/ m 2 30 min inf on saline MTX 15 mg ITH inj 24 Gy DNR 45 mg/m 2 VCR 2 mg I. v. VCR/Pred 60 mg / m 2 P. O. D 1 -28 1 7 1 8 15 22 28 Prephase Days Induction treatment Phase I 11/1/2020 Free Template from www. brainybetty. com 31

Details of induction treatment of standard-risk group Prephase If TLC >25000 and/or marked organomegaly • VCR : 2 mg I. V. …………. … D 1 • Pred: 60 mg / m 2 P. O. ………………. . D 1 -7 11/1/2020 Free Template from www. brainybetty. com 32

Details of induction treatment of standard-risk group Phase I induction • VCR: 2 mg I. V. ………………. . . D 1, 8, 15, 22 • DNR: 45 mg/m 2 (30 min. inf. ). . . D 1, 8, 15, 22 • L-Asp: 5000 U/m 2 ………………. D 15– 28 • Prednisone: 60 mg /m 2 P. O. . . . D 1 -28 followed by dose reduction in 3 phases of 3 days each: 1/2 1/4 1/8 of the dose then stop. • MTX: 15 mg intrathecal …. . ……. D 1 11/1/2020 Free Template from www. brainybetty. com 33

L-asparaginase in ALL • Used only in ALL • Enzyme that depletes serum L-asparagine • Activity related to serum L-asparagine depletion • No myelosuppression • No late effects • Unique adverse effects 11/1/2020 Free Template from www. brainybetty. com 34

L-asparaginase: Toxicity • Hypersensitivity – Neutralizing antibodies • Liver dysfunction – Liver enzymes, bilirubin, low albumin • Hemostasis – Bleeding: low clotting factors – Clotting: low antithrombin III, protein S • Pancreatitis, diabetes mellitus, CNS effects (lethargy, somnolence) 11/1/2020 Free Template from www. brainybetty. com 35

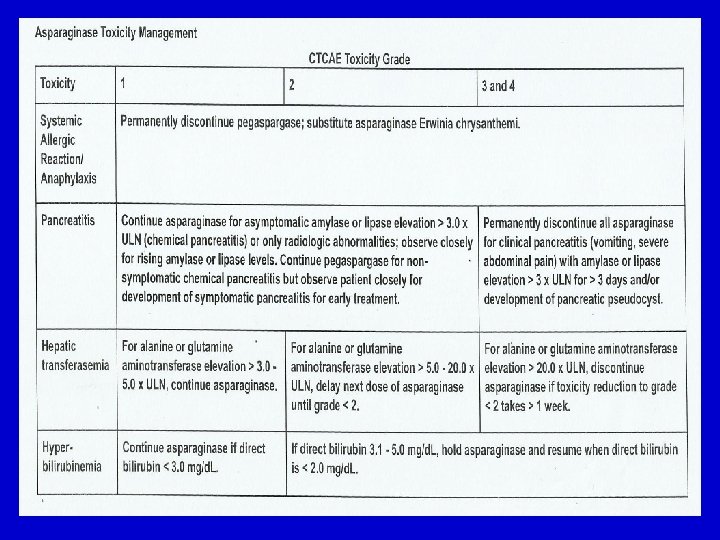
There are three formulations of asparaginase available: Asparaginase (L-asparaginase isolated from E. coli ) Erwinia asparaginase (L-asparaginase isolated from Erwinia chrysanthemi, previously called Erwinia carotova 6)7 Pegaspargase (L-asparaginase isolated from E. coli and attached to polyethylene glycol) Erwinia asparaginase is serologically and biochemically distinct from asparaginase, although the antineoplastic activity and toxicity is similar. Pegaspargase has a longer half -life and decreased toxicity.

Details of induction treatment of standard-risk group L-Asparginase • Give Erwina-Asp if possible (less adverse reactions) • Check Fibrinogen before giving L-Asp. : Ø If < 100 mg/dl give FFP 15 ml/kg or 2 gm fibrinogen for correction but continue therapy. Ø If < 50 mg /dl or prothrombin conc. falls to < 30% stop L -Asp and substitute as above. • Check blood sugar & amylase during L-asp. treatment (3 times / week) and correct hyperglycemia. • The half-life of fibrinogen is 96 hrs. Daunorubicin • DNR dose of day 15 may be omitted if the counts are very low (with no blasts in BM) 11/1/2020 Free Template from 37 www. brainybetty. com


Details of induction treatment of standard-risk group Cranial prophylaxis • All standard-risk patients receive 24 Gy cranial irradiation • During cranial irradiation, MTX 15 mg intrathecal is given as 4 doses ( twice / week) 11/1/2020 Free Template from www. brainybetty. com 40
 disease is uncommon at diagnosis (< 10%) in patients")
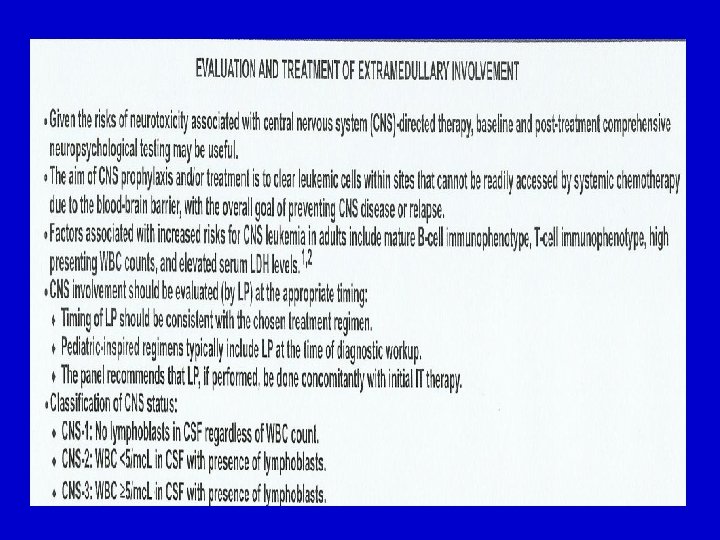
Although central nervous system (CNS) disease is uncommon at diagnosis (< 10%) in patients with acute lymphoblastic leukemia (ALL), it can increase to as high as 50% to 75% of patients at 1 year without central nervous system (CNS)–directed therapy.

In the absence of IT therapy, isolated CNS recurrence can account for 10% to 16% of relapses, warranting the inclusion of IT chemotherapy in CNS prophylactic regimens. In a study, the use of IT chemotherapy in combination with the hyper-CVAD regimen (hyperfractionated cyclophosphamide, vincristine, doxorubicin, dexamrthasone alternating with methotrexate and high-dose cytarabine) reduced the incidence of CNS relapse to 4%. [Kantarjian 2000]

Details of induction treatment of standard-risk group Phase II induction To be started when neutrophils rise to >1500 /µL and platelets >100 000 / µL. • Cyclophosphamide: 650 mg/m 2 I. V. short inf. ……. … D 1, 14, 28 • ARA-C: 75 mg/m 2 short inf. ……………. D 3, 4 , 5 , 6 11/1/2020 D 9, 10, 11, 12 D 16, 17, 18, 19 D 23, 24. 25, 26 44 Free Template from www. brainybetty. com

Details of induction treatment of standard-risk group Phase II induction In this phase marked neutropenia usually occurs after the 2 nd cycle of ARA-C: § As the patient is in CR it is allowed to stop therapy in between cycles until hematological recovery occurs. § Do not reduce doses or leave out cycles 11/1/2020 Free Template from www. brainybetty. com 45

Consolidation treatment of standard-risk group Phase I consolidation Triple ITH injection ADR 25 mg/m 2 VCR 2 mg I. V. Pred 60 mg / m 2 P. O. D 1 -28 1 8 15 22 28 11/1/2020 Free Template from www. brainybetty. com Days 46

Consolidation treatment of standard-risk group Phase I consolidation • VCR 2 mg I. V. ……………. • ADR 25 mg/m 2 I. V. ………. • Pred 60 mg / m 2 P. O. ……. reduced as previously) • Triple intrathecal …………. D 1, 8, 15, 22 D 1 -28 (then D 1 » ARA-C 40 mg » MTX 15 mg » Dexamethasone 4 mg 11/1/2020 Free Template from www. brainybetty. com 47

Consolidation treatment of standard-risk group Phase II consolidation • Cyclophosphamide: 650 mg/m 2 short inf. . . D 1 • ARA-C: 75 mg /m 2 short infusion …………… D 3, 4, 5, 6 9, 10, 11, 12 100 mg /m 2 ……………. . . D 25, 26, 27, 30 • VP 16: 100 mg /m 2 short infusion ……. . . D 25, 26, 27, 30 • Triple intrathecal ………………. . . D 1 ØARA-C 40 mg ØMTX 15 mg ØDexamethasone 4 mg 11/1/2020 Free Template from www. brainybetty. com 48

Consolidation treatment of standard-risk group Maintenance therapy Duration: 2 -3 years (depending on MRD study) • 6 -MP: 60 mg/m 2 P. O. in the morning before breakfast • MTX: 20 mg /m 2 I. V. (obligatory) once weekly. CBC should be checked on a weekly basis. 11/1/2020 Free Template from www. brainybetty. com 49

Adult ALL: Maintenance Therapy • Weekly methotrexate + daily 6 -mercaptopurine • • Duration: 2 -3 years Appropriate for all cases except B-cell and Ph+ ALL Poor outcome if omitted No randomized trials in adults 11/1/2020 Free Template from www. brainybetty. com 50

• No maintenance therapy is given in mature B-cell ALL as these patients have a high cure rate with short-term dose-intense regimens, and relapses beyond the first year in remission are rare. • The best maintenance therapy for patients with Ph-positive ALL remains disputed, but should incorporate effective BCR-ABL (breakpoint cluster region–Abelson) tyrosine kinase inhibitors.
 • 6 -mercaptopurine dose varies – Higher sensitivity in")
Adult ALL: Maintenance Therapy (cont’d) • 6 -mercaptopurine dose varies – Higher sensitivity in patients with inherited deficiency of thiopurine methyltransferase • Elevation of liver enzyme – Recovery after discontinuation of therapy – No need to withhold or reduce dose in absence of severe liver toxicity 11/1/2020 Free Template from www. brainybetty. com 52

Consolidation treatment of standard-risk group Maintenance therapy Dose reduction: TLC PLT 2 000 - 3 000 100 -150 X 106 2/3 1 500 – 3 000 50 -100 X 106 1/2 < 1 500 < 50 X 106 11/1/2020 Dose of MTX and 6 -MP Free Template from www. brainybetty. com No treatment 53

Consolidation treatment of standard-risk group Maintenance therapy Triple intrathecal prophylaxis: Intrathecal • MTX 15 mg every 2 • ARA-C 40 mg months till • Dexa 4 mg. end of maintenance 11/1/2020 Free Template from www. brainybetty. com 54

3 Treatment of high -risk group 11/1/2020 Free Template from www. brainybetty. com 55
 CR Donor No donor HAM")
Treatment of high-risk group Induction (phase I & II) CR Donor No donor HAM Allo BMT 11/1/2020 Auto BMT Free Template from www. brainybetty. com 56

Treatment of high-risk group For this group 1 cycle of HAM is added after induction and before ABMT for patients who have no donor : - ARA-C: 1 gm/m 2 (3 hr inf / 12 hr) …………. D 1 -3. - Mitoxantrone: 12 mg/m 2 (30 min iv inf) … D 3 -5. On day 3 mitoxantrone should be given before the morning dose of ARA-C Dexamethasone eye drops should be given every 6 hrs on day 1 -7 11/1/2020 Free Template from www. brainybetty. com 57

Treatment of high-risk group Regimen: Induction by high risk protocol as Hyper-CVAD Regimen Overall, 92% of patients obtained a CR. The 5 -year survival and percentage of patients in CR at 5 years were both 38%. Patients with Ph+ ALL had a 92% CR rate but only a 12% 5 year survival. Patients with T-cell ALL had a 75% CR rate and a 48% 5 year survival Patients with Burkitt ALL had a 93% CR rate and a 67% 5 year survival.

Hyper-CVAD Regimen • Part A – Dexamethasone, vincristine, doxorubicin, cyclophosphamide • Part B (after WBC recovery) – High-dose MTX, high-dose cytarabine – No asparaginase • Parts A and B repeated 4 times 11/1/2020 Free Template from Kantarjian H, et al. J Clin Oncol. 2000; 18: 547 -561. www. brainybetty. com 59

Hyper-CVAD Regimen 11/1/2020 Free Template from www. brainybetty. com 60
: • First CR – Allo SCT or MUD in high-risk")
Stem Cell Transplantation (SCT): • First CR – Allo SCT or MUD in high-risk patients – Role in standard-risk patients unclear but not recommended – Auto SCT: no benefit over chemotherapy • Second CR – Allo SCT 11/1/2020 Free Template from Hahn T, et al. Biol Blood Marrow Transplant. 2006; 12: 1 -30. www. brainybetty. com 61

Allo BMT vs Auto BMT in Patients With Ph- ALL: MRC UKALL XII/ECOG E 2993 High-Dose Methotrexate (3 doses) Patients with Ph- ALL aged < 55 yrs in complete remission after induction therapy Sibling Allo BMT (n = 389) Yes HLA-matched sibling donor available? (N = 919) No High-Dose Methotrexate (3 doses) 11/1/2020 Rowe JM, et al. ASH 2006. Abstract 2. Free Template from www. brainybetty. com Auto BMT (n = 530) Consolidation/Maintenance Chemotherapy: 2. 5 years 62

Allo BMT vs Auto BMT in Patients With Ph- ALL: 5 -Year Results • Improved OS with allo BMT vs auto BMT or postinduction chemotherapy in standard-risk Ph- patients Outcome by Risk Group, % Donor (n = 389) No Donor (n = 530) P Value Overall 5 -yr survival 53 45 . 02 • High risk 40 36 . 50 • Standard risk 63 51 . 01 39 62 <. 0001 10 -yr relapse rate • High risk 11/1/2020 • Standard risk Free Template from www. brainybetty. com 27 50 63 <. 0001
")
Allo BMT vs Auto BMT in Patients With Ph- ALL: 5 -Year Results (cont’d) • Better EFS, OS with consolidation/maintenance chemotherapy vs auto BMT – No role for auto BMT in postremission Phnegative ALL » Allo BMT treatment of choice in standard -risk patients Outcome by Risk Group, % Chemother apy Auto BMT P Value Overall 5 -yr survival • High risk • Standard risk 11/1/2020 Overall EFS 47 40 49 Free Template from 42 www. brainybetty. com 37 32 41 33 . 06. 2. 2. 02 64 Rowe JM, et al. ASH 2006. Abstract 2.
 ALL • t(9; 22) bcr/abl translocation • Precursor B cell •")
Philadelphia Chromosome (Ph+) ALL • t(9; 22) bcr/abl translocation • Precursor B cell • Incidence continuously increasing with age – Rare in children; 50% incidence in ALL patients older than 55 years of age • Associated with very poor outcome – No cure with intensive ALL chemotherapy (all ages) – Cure with SCT • Lower cure rate than other ALL subtypes 11/1/2020 Free Template from www. brainybetty. com 65

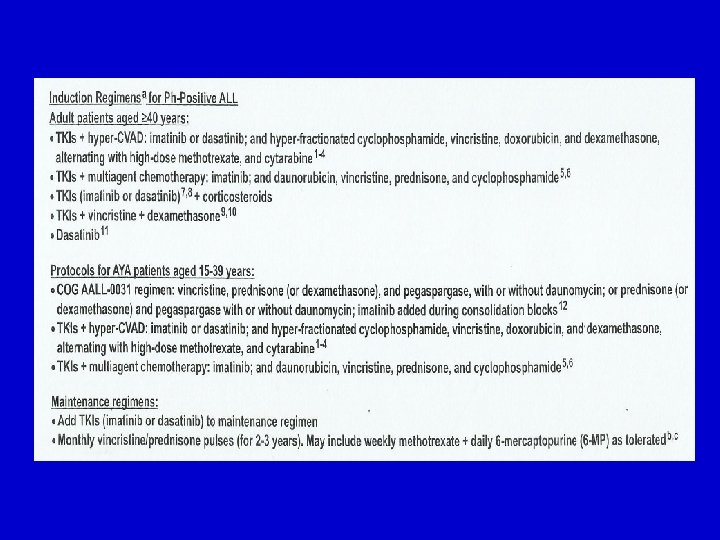
Imatinib in Ph+ ALL • Induces high response rate as single agent – Response generally not durable • In combination with ALL chemotherapy – Higher CR rate: 90% to 97% and improved outcome compared with chemotherapy alone[1, 2] – Increased access to transplantation for more patients[3] – Improves outcome of subsequent SCT[3] – Concurrent administration of imatinib + chemotherapy superior to alternating schedule[4] 1. Thomas DA, et al. Blood. 2004; 103: 4396 -4407. 2. Yanada M, et al. J Clin Oncol. 2006; 24: 460 -464. 3. Lee S, et al. Blood. 2005; 105: 3449 -3457. 11/1/2020 Free Template from 4. Wassmann B, et al. Blood. 2006; 108: 14691477. www. brainybetty. com 66

• Imatinib mesylate, in combination with hyper-CVAD in a phase II study of newly diagnosed Ph-positive ALL patients • In the overall study population, the 3 -year CR duration was 68% vs 24% for hyper. CVAD alone, and the 3 -year overall survival rate was 54% vs 15% for hyper. CVAD alone. Similar results have been reported with other studies of Imatinib and dose-intensive chemotherapy programs.

ALL in Older Adults • • • Low CR and survival rates Lower rate of T-cell ALL High rate of Ph-positive ALL Often excluded from clinical trials Often receive attenuated chemotherapy 11/1/2020 Free Template from www. brainybetty. com 70

Complications Observed in Older Adults With ALL • Comorbid conditions • More severe mucositis related to pain medications • Events associated with specific chemotherapies – Vincristine: neuropathy, constipation – Steroids: hyperglycemia, infections – L-asparaginase: encephalopathy (lethargy and somnolence) • Low marrow reserve – Adding G-CSF improves CR rate 11/1/2020 Free Template from www. brainybetty. com 71

1 Treatment of Mature B-cell Type 11/1/2020 Free Template from www. brainybetty. com 72
: Burkitt’s Leukemia • Rapid cell proliferation and very high")
B-Cell ALL (FAB L 3): Burkitt’s Leukemia • Rapid cell proliferation and very high LDH • t(8; 14), t(2; 8), t(8; 22) – Rearrangement of myc protooncogene (ch 8) with Ig heavy chains (ch 14) or light chains (ch 2 or 22) • Short intensive chemotherapy – High-dose MTX and cyclophosphamide • Intensive CNS prophylaxis • No maintenance • Cure rate: 60%; relapse rare 6 months after CR 11/1/2020 Free Template from www. brainybetty. com 73
 Patients < 50 yrs Give 2 full blocks")
Treatment of mature B-cell type (1) Patients < 50 yrs Give 2 full blocks (A 1+B 1) CR No CR Low-risk High-risk Continue for another 4 blocks till CR A 2+B 2 +A 3 + B 3 HLA identical donor Then stop treatment 11/1/2020 Available Allo BMT Free Template from www. brainybetty. com Not available Auto BMT 74

Treatment of mature B-cell type Prephase – Cyclophosphamide: 200 mg/m 2 (1 hr inf. )---- D 1 -5 – Prednisone: 60 mg /m 2 P. O. . . ……………. D 1 -5 11/1/2020 Free Template from www. brainybetty. com 75

Treatment of mature B-cell type Block A § § § § VCR: 2 mg I. V……………. . D 1 MTX: 3 gm /m 2 ( over 24 hrs)………. . D 1 Ifosphamide: 800 mg/m 2 (1 hr inf. )……. D 1 -5 VP 16 or vumon : 100 mg/m 2 (1 hr inf. ). . D 4, 5 ARA-C: 150 mg/m 2 1 hr inf/12 hr……. . . D 4, 5 Dexamethasone : 10 mg/m 2 I. V. … D 1 -5 Triple intrathecal : …………. . D 1& 5 üMTX 15 mg üARA-c 40 mg üDexamethasone 4 mg 11/1/2020 Free Template from www. brainybetty. com 76

Treatment of mature B-cell type Block B § § § after 2 weeks give block B VCR: 2 mg I. V. ………………. . D 1 MTX: 3 gm /m 2 ( over 24 hrs)…………. …… D 1 Cyclophosphamide: 200 mg/m 2 (1 hr inf. ). . . D 1 -5 Doxorubicin: 25 mg/m 2(short infusion)…… D 4, 5 Dexamethasone : 10 mg/m 2 I. V. ……… D 1 -5 Triple intrathecal : ……………. . . D 1& 5 üMTX 15 mg üARA-c 40 mg üDexamethasone 4 mg 11/1/2020 Free Template from www. brainybetty. com 77
 •")
Treatment of mature B-cell type How to administer HD MTX (3 gm/m 2) • Route: Ø 10% of the dose short infusion over ½ hr Ø 90% of the dose continuous I. V. infusion over 23½ hr • Hydration: - Ø 3 L / m 2 glucose/saline ØAdd to each bottle: 20 m. Eq Na. HCo 3 & 10 m. Eq Kcl Ø 40 mg Lasix given at 6; 12 hrs after start of MTX. 11/1/2020 Free Template from www. brainybetty. com 78
 •")
Treatment of mature B-cell type How to administer HD MTX (3 gm/m 2) • Start leucovorin rescue: 1 hr infusion in at least 150 ml solvent (high Ca content): ØAt hr 42 30 mg/m 2 ØAt hr 48 15 mg/m 2 ØAt hr 54 15 mg/m 2 11/1/2020 Free Template from www. brainybetty. com 79
 Patients > 50 yrs Give 4 incomplete blocks")
Treatment of mature B-cell type (2) Patients > 50 yrs Give 4 incomplete blocks (without HD MTX) a 1 + b 1 + a 2 + b 2 CR No furtherapy 11/1/2020 Free Template from www. brainybetty. com 80
 (1) CNS leukemia 11/1/2020 Free")
Treatment of ALL The sanctuaries (CNS and testis) (1) CNS leukemia 11/1/2020 Free Template from www. brainybetty. com 81

CNS leukemia Diagnosis CNS Leukemia is diagnosed by at least one of the following criteria: CSF • Leukocytic Cell count > 5/ l + morphological evidence of blasts in the cytospin (fresh within 10 minutes of sampling). • protein , glucose. CT CP Evidence of leptomeningeal infiltration. Headache Vomiting Visual disturbances Cranial nerve palsies especially VII 11/1/2020 Free Template from www. brainybetty. com Seizures 82
 Papilloedema 2) Hemorrhage 3) Fungal infection (opaque")
CNS leukemia Fundus ex. Look for: 1) Papilloedema 2) Hemorrhage 3) Fungal infection (opaque vitreous) 4) CMV ( pale optic disc ) 5) Leukemic infiltration 11/1/2020 Free Template from www. brainybetty. com 83
 Patients with initial CNS presentation • Are not regarded")
Treatment of CNS leukemia A) Patients with initial CNS presentation • Are not regarded as high-risk based on this presentation alone. • If such patients receive adequate therapy, their prognosis is not worse. • These patients should be stratified according to other known risk factors and treated in their group according to the previous plan. 11/1/2020 Free Template from www. brainybetty. com 84
 Patients with initial CNS presentation • However these patients")
Treatment of CNS leukemia A) Patients with initial CNS presentation • However these patients should receive triple intrathecal therapy (and not MTX alone as usual) - MTX 15 mg - ARA-c 40 mg - Dexa Trendelnberg position X 2 hrs. 4 mg • To be started in the prephase and repeated 2 times / week until CSF is free and then 5 more doses are given (twice/week). 11/1/2020 Free Template from www. brainybetty. com 85
 Patients with initial CNS presentation Furtherapy Standard-risk pts Craniospinal irradiation after phase II")
A) Patients with initial CNS presentation Furtherapy Standard-risk pts Craniospinal irradiation after phase II of induction (in this situation, the irradiation is given as prophylaxis against recurrence. Patients are usually already free after ITH therapy) Triple intrathecal injections are given every 2 months for 2 years High-risk pts Patients will receive allo or auto BMT i. e. No CNS irradiation (irrespective whether maintenance treatment is indicated or not) 11/1/2020 Free Template from www. brainybetty. com 86
 Patients with CNS relapse (± BM relapse) Triple ITH twice/week till CSF is")
B) Patients with CNS relapse (± BM relapse) Triple ITH twice/week till CSF is clear + Concomitant systemic treatment e. g. HAM 5 more doses Allo or auto BMT if possible If allo or auto BMT are not possible (such patients usually had cranial prophylaxis 24 Gy before) Complete 30 Gy on the cranium and add 24 Gy on the spine followed by triple ITH every 2 months for at least 24 months No consolidation or maintenance treatment 11/1/2020 Free Template from is effective in such patients. www. brainybetty. com 87
 (2) Testicular relapse 11/1/2020 Free")
Treatment of ALL The sanctuaries (CNS and testis) (2) Testicular relapse 11/1/2020 Free Template from www. brainybetty. com 88

Testicular relapse • Either isolated or accompanied by BM relapse Diagnosis US guided biopsy Management Orchiectomy Or 30 Gy irradiation on both testes (even if one only is affected) 11/1/2020 + One course of HAM concomitantly Free Template from www. brainybetty. com Immediate allo or auto BMT (if eligible) 89

Treatment of primary refractory ALL • Patients who do not enter into CR after induction (phase I & II) One course of HAM If no response Ida FLAG If no response 11/1/2020 Palliative treatment Free Template from www. brainybetty. com 90
 BM Relapse >1 yr after")
Treatment of BM Relapse • (irrespective of risk group) BM Relapse >1 yr after induction treatment ≤ 1 yr after induction treatment Re-induction with the same protocol Salvage Course HAM not given before CR 2 Available donor No available donor Allo BMT One course of HAM FLAG or AVVV HAM CR 2 Available donor No available donor Allo BMT Discontinue treatment 11/1/2020 HAM given before Free Template from 91 No consolidation or maintenance treatment is effective in such patients www. brainybetty. com

Treatment of BM Relapse In both groups CNS-directed triple intrathecal injections should be given every two months for 24 months 11/1/2020 Free Template from www. brainybetty. com 93

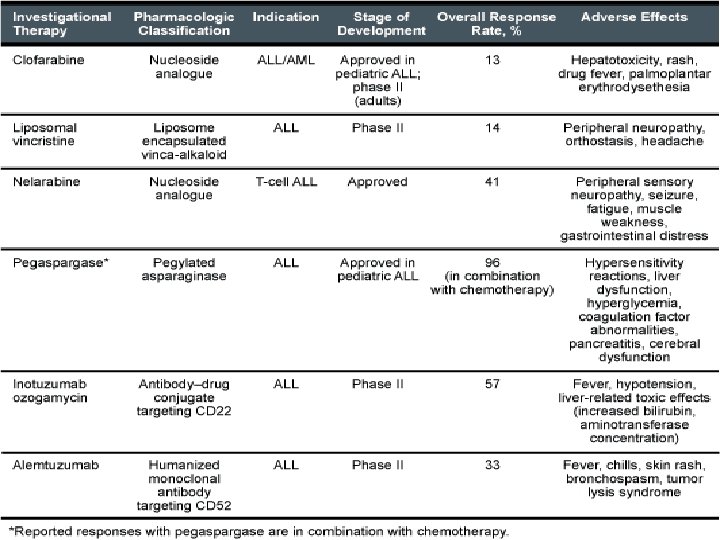
New Chemotherapies • Rituximab. Anti-CD 20 May potentiate chemotherapy in B-cell malignancies . • Alemtuzumab. Anti-CD 52. • Liposomal encapsulated drugs: • Liposomal vincristine diminished neurotoxicity • Liposomal daunorubicin diminished cardiotoxicity • Pegylated asparaginase Long half-life (6 days) • Cytarabine liposome injection (IT) 11/1/2020 Free Template from 94 www. brainybetty. com
 Pro-drug of ara-G. Effective in T-ALL")
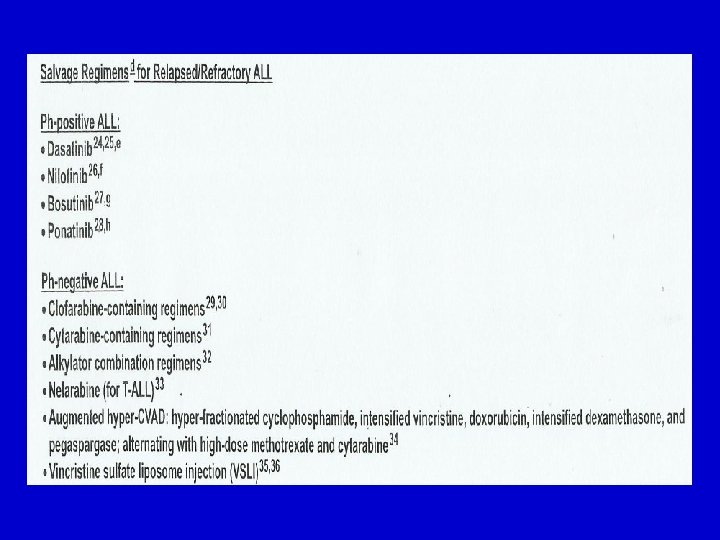
New Chemotherapies • Antimetabolites – Nelarabine (relapsed T-ALL) Pro-drug of ara-G. Effective in T-ALL Inhibits purine nucleoside phosphorylase (PNP). – Clofarabine (Nucleoside analog ); inhibits ribonucleotide reductase and DNA polymerase. Approved for relapsed childhood ALL. – Trimetrexate (dihydrofolate reductase inhibitor) 11/1/2020 Free Template from www. brainybetty. com 95

Pegylated Asparaginase • In children – More rapid reduction in marrow blasts during induction – Lower incidence of neutralizing antibodies – Similar safety profile as native form • In adults – Similar toxicity to native form after Avramis VI, et al. Blood. 2002; 99: 1986 -1994. 11/1/2020 Free Template from 96 Panosyan EH, et al. J Pediatr Hematol Oncol. 2004; 26: 217 -226. single and multiple www. brainybetty. com • Pegylated E. coli L-asparaginase • Less immunogenic • Long half-life – Less frequent dosing – Continuous asparagine depletion

T-Cell ALL: Gamma Secretase Inhibitor MK 0752 • NOTCH 1 gain-of-function mutations in 50% of T-ALL • Gamma secretase inhibitors abrogate(inhibit) stimulatory effects of NOTCH 1 11/1/2020 Free Template from De. Angelo D, et al. ASCO 2006. Abstract 6585. www. brainybetty. com 97

Common cytogenetic abnormalities in T-ALL
 chromosomal translocation")
Chromosomal translocation of NOTCH 1 causes T cell leukaemia The t(7: 9) chromosomal translocation in T-ALL patients is characterised by the juxtaposition of the 3’ part of the human Notch 1 gene into the T cell receptor β locus. This leads to expression of truncated Notch 1 transcripts from the TCR? promoter, causing T cell leukaemia (T-ALL).

ALL: Targeted Treatments • Targets include BCR/ABL, CD 20, and FLT 3 overexpression, among others ALL Subtype Target Treatment Ph+ BCR/ABL Imatinib, dasatinib, nilotinib T cell NUP 214 -ABL 1 NOTCH 1 mutation Imatinib, dasatinib, nilotinib Gamma secretase inhibitor Mature B cell CD 20 Rituximab Precursor B cell CD 20 Rituximab All subtypes CD 52 Alemtuzumab FLT 3 overexpression CEP 701, PKC 212 MLL and hyperdiploidly 11/1/2020 Free Template from www. brainybetty. com 100

ALL: Novel Management Approaches • Minimal residual disease evaluation – Define prognostic groups for treatment selection • Microarray analysis (gene expression profiles) – Prognosis – Identify new targets 11/1/2020 Free Template from www. brainybetty. com 102
 has become")
• Measurement of MRD in patients with acute lymphoblastic leukemia (ALL) has become an increasingly important prognostic factor for assessing risk of patient relapse. • Persistence of MRD early in complete remission typically does not have the same significance as detection of residual disease in later stages of therapy.

• A recent study suggested that detection of MRD by flow cytometry at the time of allogeneic hematopoietic stem cell transplantation in either adult or children with ALL was predictive for decreased overall survival, leukemia-free survival, and event-free survival after transplant [Sanchez-Garcia 2013]

Minimal Residual Disease • Methods – Multicolor flow cytometry or PCR – Prognostic levels defined for children; prognostic time points and levels yet to determined for adults Time of Evaluation Prognosis Minimum Residual Disease Children • At CR • After CR < 0. 01% 11/1/2020 Free Template from > 0. 1% www. brainybetty. com Excellent outcome High relapse risk 105

Minimal Residual Disease and Prognosis in ALL • 4730 patients on AIEOP-BFM ALL 2000 (pediatric) • MRD measured by RT-q. PCR at Days 33 and 77 5 -Yr EFS by MRD-D 33/77, % Pre B-ALL (Day 33/Day 77) T-ALL (Day 33/Day 77) Neg 92/88 94/92 ≤ 10 -4 82/69 91/77 10 -3 66/56 75/50 MRD Levels ≥ 10 -2 53/38 60/33 • MRD more + in T-ALL on D 33 (84% vs 56%) and D 77 (52% vs 22%) • High MRD predictive of poorer survival for both disease types • D 33 measurement more predictive of 5 -year EFS > 90%

Minimal Residual Disease and Prognosis in ALL • Separate study tested MRD at 0. 1% level in 165 patients with ALL with CR (85. 5%) following induction and consolidation therapy • Patients assigned to standard-risk (23%) or high-risk (77%) groups • MRD only significant predictive factor in multivariate analysis for – Relapse incidence (HR: 2. 5; P =. 006) – Leukemia-free survival (HR: 2. 1; P =. 01) Parameter, % MRD+ MRD- P Value MRD evaluated after induction (37% MRD+) 82 29 . 00007 MRD evaluated after consolidation (26% MRD+) 62 41 . 05 3 -yr leukemia-free survival 26 65 . 008 Overall relapse incidence 73 28 . 004 • Standard-risk group 92 20 . 01 3 -yr relapse incidence • High-risk group Holowiecki J, et al. ASH 2007. Abstract 2821. 70 33. 05
- Slides: 107