ACUTE KIDNEY INJURY IN ICU MODERATOR Dr Apurba

ACUTE KIDNEY INJURY IN ICU • MODERATOR: Dr. Apurba Kumar Borah • Presenter: Dr. Rajib Duarah • DEPT OF CRITICAL CARE MEDICINE • NH NARAYANA SUPERSPECIALITY HOSPITAL, GUWAHATI.

DEFINITION • In the ICU, AKI describes a syndrome characterised by a rapid (hours to days) decrease in the kidney’s ability to eliminate waste products such as urea and creatinine. Other typical clinical manifestations include decreased urine output, metabolic acidosis and hyperkalaemia.

DEFINITION • AKI can now be defined and classified using changes in serum creatinine and urine output using the so called RIFLE criteria. This classification uses the acronym of RIFLE, to divide AKI into the categories of Risk, Injury, Failure, Loss and ESKD. • Later on another consensus definition was proposed by the AKIN (Acute Kidney Injury Network) group, with minor modifications and, more recently, by the KDIGO consensus group
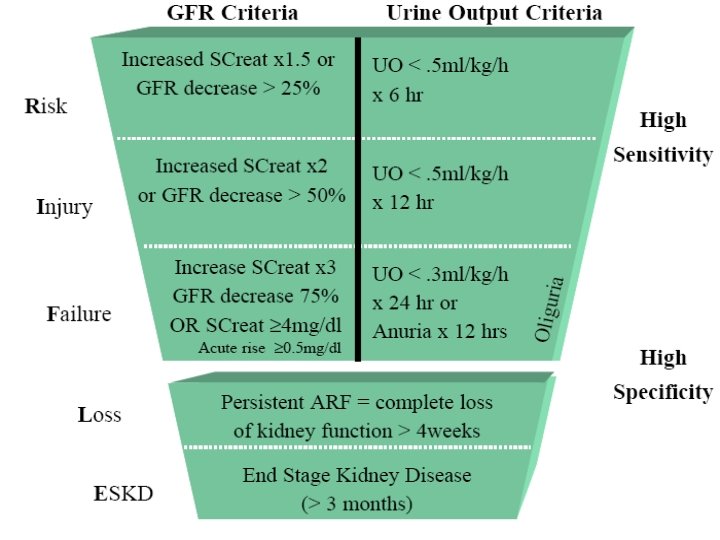

AKIN CRITERIA • Because of the limitations of the RIFLE criteria just mentioned, revised criteria were introduced by the Acute Kidney Injury Network (AKIN). The AKIN criteria require a smaller change in creatinine (≥ 0. 3 mg/d. L) for the diagnosis of AKI, and a time limit of 48 hours is imposed on the change in serum creatinine. Unfortunately, the RIFLE criteria were not abandoned after introduction of the AKIN criteria, so there are two competing systems for the diagnosis and classification of AKI at the present time.

AKIN Diagnostic criteria

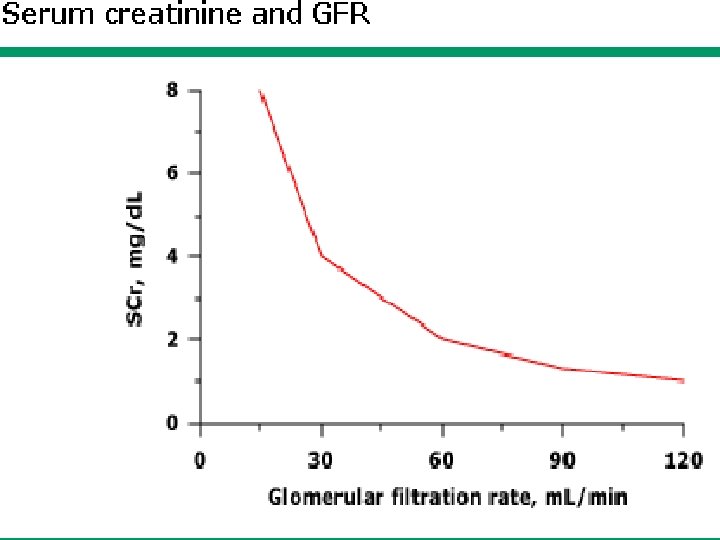
BUN or S. Creatinine without GFR • urea GI bleed, drugs, protein intake, aminoacid infusion, hypercatabolism and febrile illness. • Creatinine Rhabdomyolysis
![ESTIMATED EQUATIONS • Cockcroft-Gault equation Ccl [ml/min] = 140 - age LBW[ kg] S.](http://slidetodoc.com/presentation_image_h2/6d44d5c3071ce64cd2cf33996966324c/image-9.jpg "ESTIMATED EQUATIONS • Cockcroft-Gault equation Ccl [ml/min] = 140 - age LBW[ kg] S.")
ESTIMATED EQUATIONS • Cockcroft-Gault equation Ccl [ml/min] = 140 - age LBW[ kg] S. Cr[mg/dl] 72 • MDRD Equation GFR ml/min/1. 73 m 2 = 175*SCr[ exp- 1. 154] *age [exp – 0. 203] *0. 742 [female]

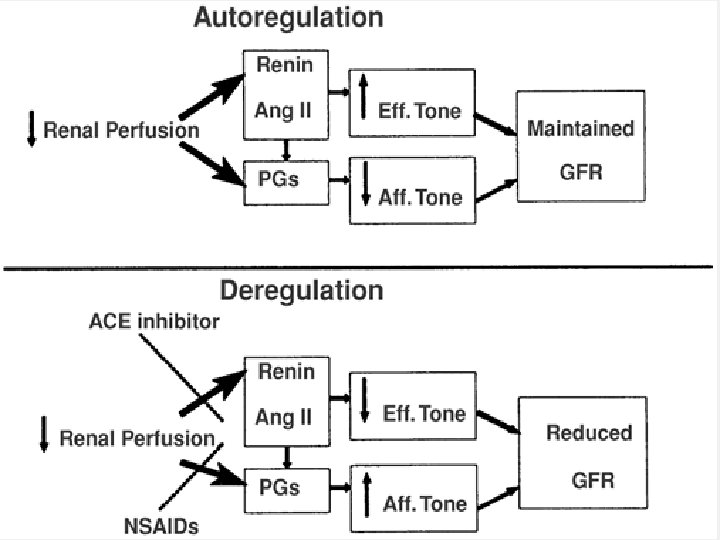
Causes of Acute Renal Failure • Prerenal azotemia Hypovolemia Reduced effective circulating volume Autoregulatory failure Intrinsic renal disease Glomerular diseases Vascular diseases (main renal artery and microcirculation) Tubulointerstitial disease Acute tubular necrosis Acute cortical necrosis Postrenal failure Ureteric obstruction (bilateral or solitary kidney) Lower tract obstruction (bladder neck or urethra)

CAUSES OF PRE-RENAL AZOTEMIA

CAUSES OF INTRA-RENAL AZOTEMIA

CAUSES OF POST-RENAL AZOYEMIA

INTENSIVE CARE SYNDROME ASS WITH ARF • Ischemic ARF Extracellular volume depletion Postoperative (particularly cardiac surgery) Severe ventricular dysfunction or cardiogenic shock Sepsis Pancreatitis Trauma Burns Acute bilateral cortical necrosis Nephrotoxicity and drug-induced ARF Myoglobinuric ARF Radiocontrast nephropathy Drugs

Ischemic renal failure Renal hypoperfusion Extra cellular volume depletion-diuresis, GI losses Transdermal fluid losses Post operative ARF-abdominal, vascular, cardiac Sepsis Pancreatitis Trauma-volume depletion, Hemorrhage, myoglobinuria • Radiocontrast induced • •

ARF AFTER CARDIAC SURGERY • 2/3 of post op ARF • Prolonged Cardio Pulmonary bypass, poor LV function • Mayers and Moren abbreviated form-use of vasoconstrictors overt form - poor LV function protracted form- second insult

• Acute bilateral cortical necrosis Obstetric complication –abruptio placenta, eclampsia, septic abortion, amniotic fluid embolism Snake bite, sepsis DIC, arsenic poisoning, renal graft rejection Myoglobinuriamassive skeletal injury, burns, heroin, amphetamine Hemoglobinuriabinds with haptoglobulin, filtered only saturated [Hb > 100 mg/dl]

DRUGS CAUSING AIN

Syndromes of Drug-Induced Renal Failure • Acute tubular injury Aminoglycoside antibiotics Cephalosporin antibiotics Antifungal agents (amphotericin) Antiviral agents (foscarnet) Heavy metals (cisplatin) Intratubular microobstruction Methotrexate Acyclovir Sulfamethoxazole Dextran Acute interstitial nephritis Autoregulatory failure Angiotensin-converting enzyme inhibitors Nonsteroidal antiinflammatory drugs

RENAL VASCULAR DISEASES Major vessels –renal artery occlusion , stenosis Micro vessels – emboli, atheroemboli Bilateral renal vein occlusion Hemolytic uremic syndrome-diarrhea, drugs ARF in cancer patients- tumor lysis syndrome [cysplatin], hypercalcemia, metastatic obstruction • ARF in liver diseases – hepatorenal syndrome • • •

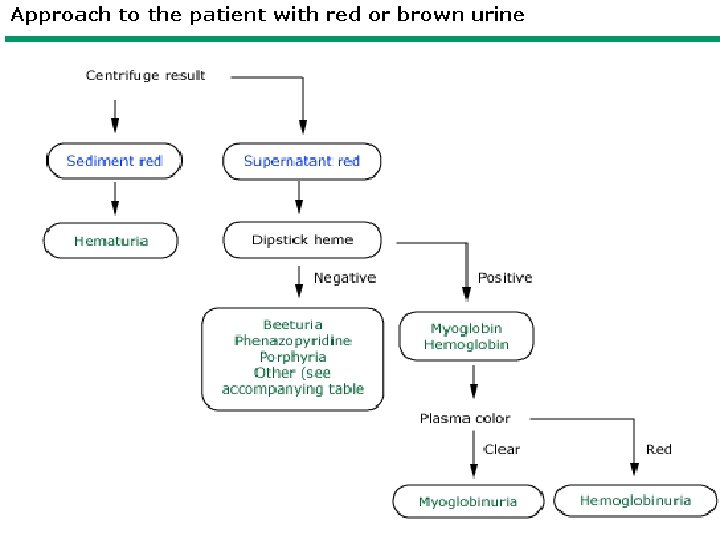
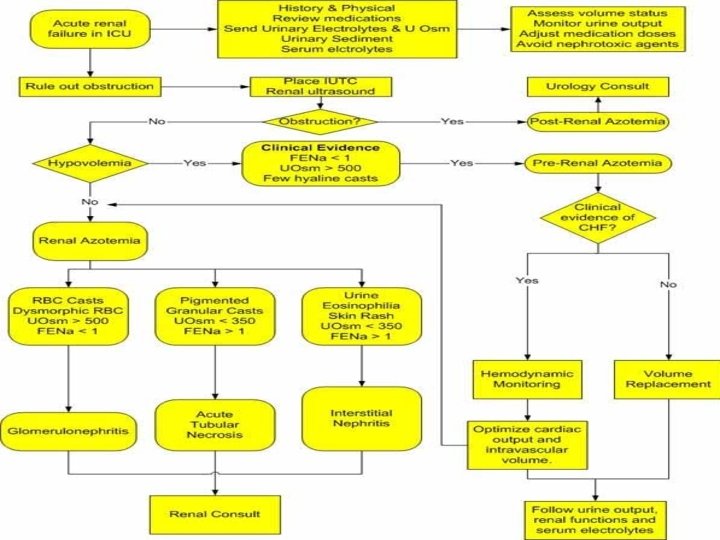
DIAGNOSIS • History - previous records, thirst, wt loss, drugs • Physical exam - signs of dehydration , high BP, signs of systemic diseases, obstructive symptoms • Urine tests - osmolality , electrolytes, Creatinine, protein, heme pigments, sp gravity. • Blood tests - CBC, routine chemistries, serology • Radiography- IVP, USG, CT, retrograde pyelography, isotopic scanning. • Renal biopsy

• Fe. Na = U Na/ S Na U Cr / S Cr • Most accurate screening test Effective in severe renal dysfunction and oliguria

Laboratory studies used to differentiate between prerenal ARF and ATN

URINE DEPOSITS

RBC CASTS

WBC CASTS

GRANULAR CASTS

EPITHELIAL CASTS

COMPLICATIONS

BIOMARKERS • • Kidney injury molecule Neutrophil gelatinase-associated lipocalin Cystatin C Troponin like renal injury factor Retinol binding protein Alpha 1, alpha 2 microglobulin N-acetyl glucosaminidase
 volume")
INITIAL MANAGEMENT • The early management of AKI should include the following: (a) volume infusion to promote renal blood flow, (b) discontinuing any nephrotoxic drugs, and (c)treating any conditions that predispose to AKI (e. g. , sepsis).

Fluid Challenges • If a prerenal source of AKI has not been ruled out, prompt volume infusion is warranted. Delays in correcting renal hypoperfusion can lead to intrarenal damage, so prompt attention to volume resuscitation is mandatory. Fluid challenges can be given in 500 ml to 1, 000 m. L aliquots for crystalloid fluids and 300 m. L to 500 m. Laliquots for colloid fluids, infused over 30 minutes

Intrarenal Disorders • The only early option available for halting or reversing the course of AKI due to intrarenal disorders (i. e. , ATN and AIN) is to discontinue possible offending drugs. • Despite its popularity in AKI, intravenous furosemide does not improve renal function in AKI, and does not convert oliguric to non-oliguric renal failure. Furosemide can increase urine output during the recovery phase of AKI , and a trial of furosemide is reasonable during this period to relieve fluid accumulation.

Contrast-Induced Renal Injury • Iodinated contrast agents can damage the kidneys in several ways, including direct renal tubular injury, renal vasoconstriction, and the generation of toxic oxygen metabolites. • The most effective preventive measure for contrast-induced nephropathy in high-risk patients is intravenous hydration(if permitted). • N-acetylcysteine (NAC) is a glutathione surrogate with antioxidant actions that has had mixed results as a protective agent for contrast induced nephropathy
 • AIN is an inflammatory condition that involves the renal")
Acute Interstitial Nephritis (AIN) • AIN is an inflammatory condition that involves the renal interstitium and presents as acute renal failure. However, oliguria is not always a feature of AIN, which means that AIN does not always qualify for the diagnosis of AKI. Most cases of AIN are the result of a hypersensitivity drug reaction, but infections (usually viral or atypical pathogens) can also be involved. Antibiotics are the most common offenders, particularly the penicillins. • A renal biopsy can secure the diagnosis. • AIN usually re-solves spontaneously after the offending agent is discontinued, but recovery can take months.

Myoglobinuric Renal Failure • Acute renal failure develops in about one-third of patients with diffuse muscle injury (rhabdomyolysis). The culprit is myoglobin, which is released by the injured muscle and is capable of damaging the renal tubular epithelial cells. • Aggressive volume resuscitation to promote renal blood flow is the most effective measure for preventing or limiting the renal injury in rhabdomyolysis. Alkalinizing the urine can also help to limit the renal injury. • About 30% of patients who develop myoglobinuric renal injury will require dialysis
 is the condition where an")
Abdominal Compartment Syndrome • • Abdominal compartment syndrome (ACS) is the condition where an increase in abdominal pressure leads to dysfunction in one or more vital organs. This organ dysfunction usually involves the bowel (splanchnic ischemia), the kidneys (AKI), and cardiovascular system (reduced cardiac output). ACS occurs when the IAP rises above 20 mm Hg and there is evidence of a newlydeveloped organ dysfunction. General measures for reducing IAP include sedation (to reduce abdominal muscle contractions), avoiding elevation of the head more than 20º above the horizontal plane, and avoiding a positive fluid balance. Specific measures are dictated by the source of the elevated IAP, and can include decompression of the stomach, small bowel, or colon, percutaneous drainage of peritoneal fluid, or surgery (e. g. , for abdominal injuries or bowel obstruction). Efforts to maintain an APP >60 mm Hg (with vasopressors to increase MAP, if necessary) is associated with improved outcomes in ACS. Surgical decompression is recommended for patients with ACS when the IAP cannot be reduced by conventional measures.

RENAL REPLACEMENT THERAPY • About 70% of patients with acute renal failure will require some form of renal replacement therapy (RRT). The usual indications for RRT in acute renal failure include (a) volume overload (b)life-threatening hyperkalemia or metabolic acidosis that is refractory to conventional measures (c)removal of toxins (e. g. , ethylene glycol) • Otherwise, the optimal timing for RRT in acute renal failure is unclear.

SUMMARY • INTRAVASCULAR VOLUME STATUS IS THE MOST IMPORTANT FACTOR IN THE EVALUATION OF ARF. • A DECREASE IN URINARY VOLUME IS OFTEN ONE OF THE INITIAL CLINICAL FINDING IN ARF. • The most common cause of ARF in hospitized patient is intrinsic renal failure due to ATN. Recognition and relief of urinary outlet obstruction should be given the highest priority, especially for patient with anuria

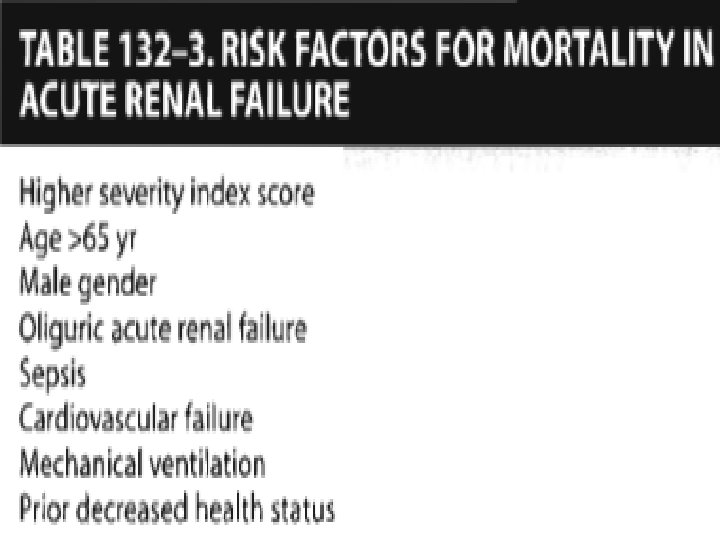
• The most important laboratory test for a patient with ARF is uninalysis. • Both urinary sediment and urinary indices in combination with serum values can often be extremely helpful in determining the cause of ARF. • Patients with oliguria UOP< 400 ml/d and rise in serum creatinine > 3 mg/dl at the time of admission have a poor prognosis • Mortality rate with ARF is about 50% and patients usually die of the sequelae of primary illness that lead to ARF and not ARF per say.

REFERENCES • • • FINK IRWIN RIPPE UPTODATE HARRISONS Paul Marino OH’s Manual
- Slides: 46