Acute Kidney Injury 1 Renal Blood Flow What

Acute Kidney Injury 1

Renal Blood Flow • What are the 3 major determinations of renal blood flow? • Cardiac output • Renal perfusion pressure • Glomerular filtration hemodynamics

Acute Kidney Injury is characterized by: 1. Sudden decline in kidney function 2. Disturbances in fluid, electrolyte, and acid-base balances 3. Loss in clearance of small solutes 4. Decreased glomerular filtration rate (GFR)

RIFLE Classification System of Acute Kidney Injury Grade of Severity • Risk : • Serum creatinine increased 1. 5 times • GFR decreased 25%, • Urine output of <0. 5 ml/kg/hr x 6 hrs • Injury: • Serum creatinine increased 2 times • GFR decreased 50% • Urine output of <0. 5 ml/kg/hr x 12 hrs • Failure: • Serum creatinine increased 3 times • GFR decreased 75% • Urine output of <0. 3 ml/kg/hr x 24 h, anuria 12 hr , oliguria S E V E R I T Y

RIFLE Classification System of Acute Kidney Injury • Loss : complete loss of renal function for > 4 weeks • End-stage kidney disease: need for renal replacement therapy for > 3 months O U T C O M E S

3 categories of Acute Kidney Injury • Pre renal • Intra renal • Post renal 6

Acute Renal Failure • Prerenal Most common cause of ARF Caused by impaired renal blood flow GFR declines because of the decrease in filtration pressure • Intrarenal Acute tubular necrosis (ATN) is the most common cause of intrarenal failure Post-ischemic or nephrotoxic • Postrenal Occurs with urinary tract obstructions distal to the kidneys 7

Prerenal Acute Kidney Injury • Decreased blood flow to the kidneys • Kidneys attempt to compensate via autoregulation and release of renin • If renal hypo perfusion persists, AKI develops

What could cause pre-renal failure? 9

Pre-renal failure You Tube https: //youtu. be/6 i 6 UKQj. GJJs 10

Intrarenal Acute Kidney Injury • Also known as acute tubular necrosis • Renal tissue is damaged due to injury or insult • Results in • • Suppression of bone marrow Endocrine disturbance Coagulopathy Cardiovascular dysfunction

Acute Tubular Necrosis • Nephrotoxic injury • Ischemic injury • When severe AKI requires hemodialysis
 • Causes 75% of all cases of acute renal failure")
Acute Tubular Necrosis (ATN) • Causes 75% of all cases of acute renal failure • There is a destruction of the tubular segment of the nephron Causes uremia • The excess accumulation of by-products of protein metabolism in the blood • Causes renal failure

Etiology-how does it happen May follow two types of kidney injury 1. Most common cause is ischemic injury 2. Nephrotoxic injury • Usually in debilitated patients that are critically ill • Patients wo have undergone extensive surgery

1. Disruption In ischemic injury, blood flow to the kidneys is disrupted: • • • Circulatory collapse Severe hypotension Trauma Hemorrhage Dehydration Cardiogenic or septic shock Surgery Anesthetics Transfusion reactions

2. Nephrotoxicity Results from: • Ingesting or inhaling toxic chemicals • Carbon tetrachloride • Heavy metals • Methoxyflurane anesthetics • A hypersensitivity reaction of the kidneys • Antibiotics • Radiographic contrast agents

Specific cause and effects • Diseased tubular epithelium that allows glomerular filtrate (that should be excreted) to leak through the membranes and be reabsorbed into the blood • Obstructed urine flow from the collection of damaged cells, casts, RBCs, and other cellular debris within the tubular walls • Ischemic injury to glomerular epithelial cells • Causes cellular collapse and poor glomerular capillary permeability • Ischemic injury to the vascular endothelium • Eventually causes cellular swelling and tubular destruction

A lesson on lesions • Deep or shallow lesions may occur in acute tubular necrosis • With ischemic injury necrosis creates deep lesions • Destroying the tubular epithelium and basement membrane • Causes patches of necrosis in the tubules • Can also cause lesions in the connective tissue of the kidney • Nephrotoxic injury causes necrosis only in the epithelium of the tubules • Leaves the basement membrane of the nephrons intact • This type of damage may be reversible

19

Complications of ATN • Infections-typically septicemia • Complicates up to 70% of cases • Leading cause of death • GI hemorrhage, fluid and electrolyte imbalance, ad cardiovascular dysfunction • Either in the acute phase or the recovery phase • Neurologic complications are common in elderly patients • Excess blood calcium may occur during the recovery phase • Hypercalcemia

You Tube-Intrarenal https: //youtu. be/ISFEg. K 8 sfb 8? t=123 21

Postrenal Acute Kidney Injury • Flow of urine is disrupted or obstructed • Pressure increases in nephron • GFR slows • Serum creatinine and BUN rise • Nephron damage can occur

Obstruction can be caused by • Anatomic or functional defect • Obstructive uropathy • Severity based on: • • • Location Completeness Involvement of one or both upper urinary tracts Duration Cause • Effects of Blockage: • Hydroureter, Hydronephrosis • Tubulointerstitial firbrosis • Apoptosis 23

Post-renal failure https: //youtu. be/vn. TR_y 3 Sf-k? t=123 24

Hydronephrosis An abnormal dilation of the renal pelvis and the calyces of one or both kidneys It is caused by the obstruction of urine flow in the genitourinary tract

If the obstruction is in the urethra or bladder, hydronephrosis usually affects both kidneys If the obstruction is in a ureter, it usually affects one kidney

What conditions can cause this? Common causes • Benign prostatic hyperplasia • Urethral strictures • Stenosis of the ureter or bladder outlet Less common causes • Congenital abnormalities • Abdominal tumors • Blood clots • Neurogenic bladder • Tumors of the ureter and bladder

From bad to worse Untreated hydronephrosis can result in infection or pyelonephritis • Due to stasis that exacerbate renal damage • May create a life-threatening crisis

Generalized signs and symptoms • Nausea and vomiting • Abdominal fullness • Dribbling • Urinary hesitancy

Essential tests • Voiding urography • Retrograde pyelography • Injection of a radiocontrast agent into the ureter in order to visualize the ureter and kidney with fluoroscopy or radiography • Fluoroscopy • an imaging technique that uses X-rays to obtain real-time moving images of the interior of an object • Renal ultrasound

AKI Assessment & Diagnosis • Laboratory • BUN: not most reliable indicator of renal damage • Creatinine: reflects renal damage • Urinalysis: Na level, osmolality, specific gravity reflect concentrating / diluting ability • Electrolyte levels: Potassium, Magnesium, Calcium most affected

Urinalysis • Dilute urine • Low osmolality • High sodium levels • Urine sediment containing RBCs and casts

AKI Assessment & Diagnosis • Hemodynamic Monitoring: fluid volume analysis • Fluid Balance: Weight, Skin turgor, Edema,

Goals for preventing AKI • Adequate hydration • Maintenance of renal perfusion • Limiting exposure to nephrotoxins • Drug protective strategies

Acute Kidney Injury • Medical Management Goals • Prevention • Correcting the causative mechanism • Promoting regeneration of remaining renal functional capacity • Management is based on category of AKI • Pre-renal • Intra-Renal • Post-Renal

Medical Management • Volume • Fluid Balance • Crystalloids and Colloids • Fluid Restriction • Fluid Removal • Electrolytes • Potassium • Sodium • Calcium • Phosphorus • Nutrition: limit protein, electrolyte, and fluid • Medications • Diuretics • Dopamine

Nursing Management • Recognizing risk factors for developing acute renal injury • Preventing infectious complications • Optimizing fluid balance • Avoiding electrolyte imbalance • Preventing anemia • Providing patient / family education
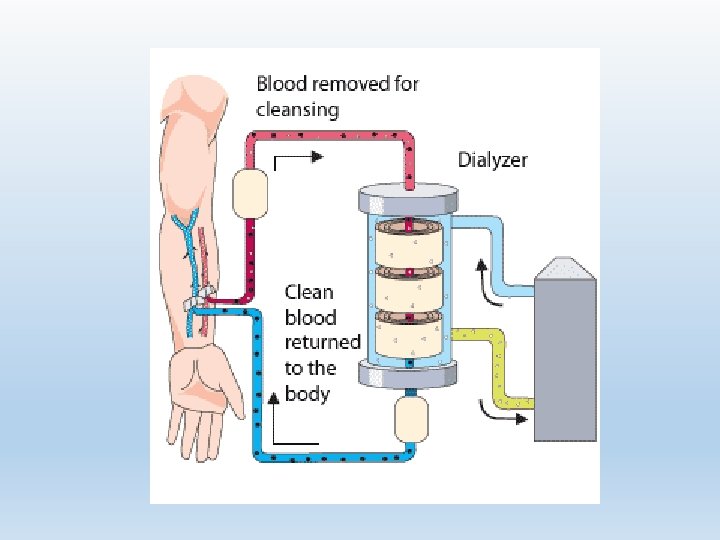
 Requirement Dialyzer")
Dialysis in the Critical Care Setting Hemodialysis Continuous Renal Replacement Therapy (CRRT) Requirement Dialyzer Anticoagulation Vascular access

Hemodialysis Indications Contraindications • Bun > 90, Serum Creatinine > 9 • Hyperkalemia • Drug toxicity • Intravascular and extravascular fluid overload • Metabolic acidosis • Symptoms of uremia • Mental changes • Contraindications to other forms of dialysis • Hemodynamic instability • Inability to anticoagulate • Lack of access to circulation • Ages extremes

 • Indications • Need for large fluid volume removal")
Continuous Renal Replacement Therapy (CRRT) • Indications • Need for large fluid volume removal in hemodynamically unstable patient • Hypervolemic patient unresponsive to diuretic therapy • Patient with multi organ dysfunction • Contraindications • Hematocrit > 45% • Inability to anticoagulate • Low mean arterial pressure • Terminal illness

Hemodialysis & CRRT • Nursing Management of Hemodialysis and CRRT • Surveillance for side-effects of dialysis • Monitoring fluid balance / electrolytes • Accurate I & O • Maintaining catheter patency • Preventing infection • Patient / family education

Pharmacology • Medication interactions with renal failure • Diuretics • Phosphate binding • Erythrocyte-stimulating hormone
- Slides: 45