Acute infective endocarditis with vegetations Ventricular Aneurysm complicating











 atelectasis: - It occurs when either local or generalized fibrotic")

 the acute onset of dyspnea, (2) decreased arterial oxygen pressure (hypoxemia), (3) development")

 - ARDS is a clinical syndrome caused by diffuse")








- Slides: 27
Acute infective endocarditis with vegetations
Ventricular Aneurysm complicating MI
Acutemyocardial infarction
Left ventricular rupture complicating MI
Respiratory system Fatima Obeidat, MD
n t l u n g. T h i s a f r e q u e n t o c c u r r e n c e w i t h p 1. Atelectasis n n Also known as collapse, is loss of lung volume caused by inadequate expansion of airspaces. It results in shunting of inadequately oxygenated blood from pulmonary arteries into veins, thus giving rise to hypoxia.
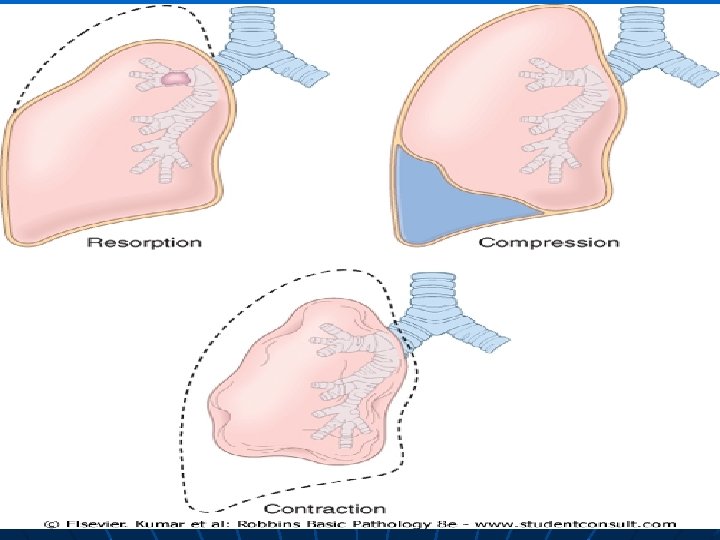
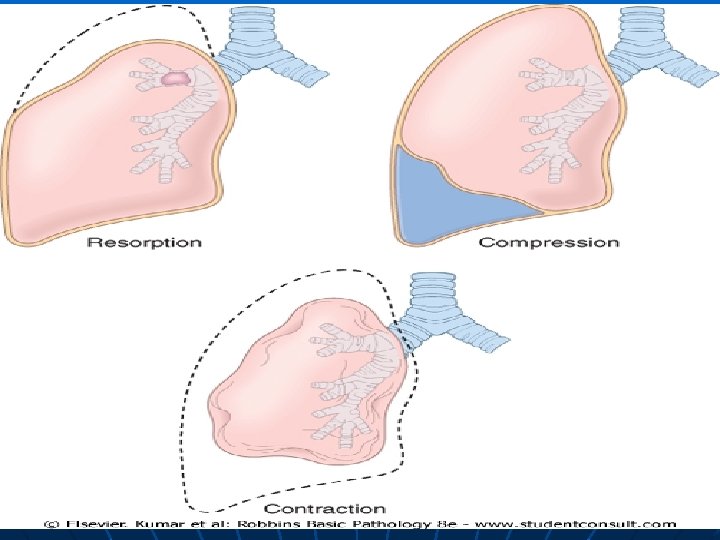
n On the basis of the underlying mechanism or the distribution of alveolar collapse, atelectasis is classified into three forms:
A. Resorption atelectasis Occurs when total obstruction prevents air from reaching distal airways. The air already present gradually becomes absorbed, and alveolar collapse follows.
- Causes 1. The most common cause is total obstruction of a bronchus by a mucous or mucopurulent plug, this frequently occurs postoperatively 2. but may also complicate bronchial asthma, chronic bronchitis, 3. or the aspiration of foreign bodies, particularly in children.
B. Compression Atelectasis - sometimes called passive or relaxation atelectasis is usually associated with accumulations of fluid, blood, or air within the pleural cavity, which mechanically collapse the adjacent lung.
Causes 1. This is a frequent occurrence with pleural effusions 2. Leakage of air into the pleural cavity (pneumothorax). 3. Basal atelectasis resulting from the elevated position of the diaphragm commonly occurs in bedridden patients, in patients with ascites, and in patients during and after surgery.
C. Contraction (or cicatrization) atelectasis: - It occurs when either local or generalized fibrotic changes in the lung or pleura prevent expansion of the lung NOTE: Atelectasis (except that caused by contraction) is potentially reversible and should be treated promptly to prevent hypoxemia and superimposed infection of the collapsed lung.
n - - ACUTE LUNG INJURY The term acute lung injury encompasses a spectrum of pulmonary lesions (endothelial and epithelial), which can be initiated by numerous conditions. Clinically, acute lung injury manifests as
(1) the acute onset of dyspnea, (2) decreased arterial oxygen pressure (hypoxemia), (3) development of bilateral pulmonary infiltrates on radiographs, (4) absence of clinical evidence of primary left-sided heart failure.
- - Since the pulmonary infiltrates in acute lung injury are usually caused by damage to the alveolar capillary membrane rather than left-sided heart failure , they represent an example of noncardiogenic pulmonary edema. Acute lung injury can progress to the more severe acute respiratory distress syndrome,
Acute Respiratory Distress Syndrome (ARDS) - ARDS is a clinical syndrome caused by diffuse alveolar capillary and epithelial damage. - There is usually rapid onset of lifethreatening respiratory insufficiency, cyanosis, and severe arterial hypoxemia that is refractory to oxygen therapy and that may progress to multisystem organ failure.
n n The histologic manifestation of ARDS in the lungs is known as diffuse alveolar damage. ARDS can occur in a multitude of clinical settings and is associated with either direct injury to the lung or indirect injury in the setting of a systemic process.
- Direct causes - Pneumonia - Aspiration of gastric contents -Indirect cause - Pancreatitis - Septic Shock
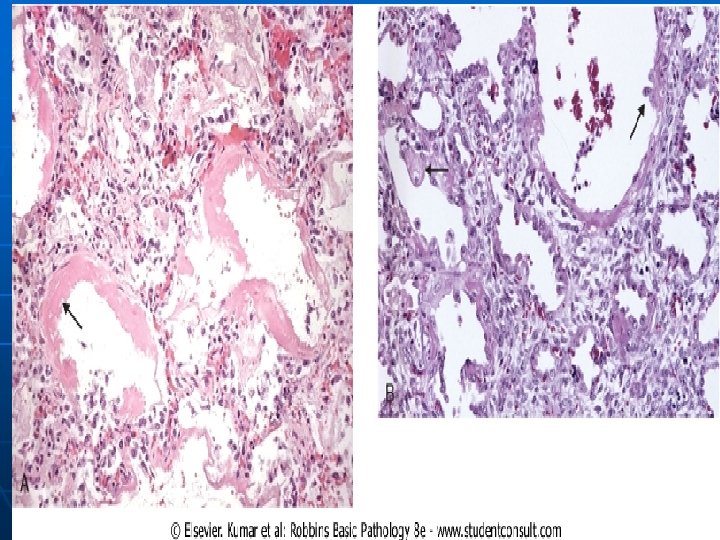
Morphology In the acute phase of ARDS - Microscopically, there is: a. necrosis of alveolar epithelial cells, b. interstitial and intra-alveolar edema and hemorrhage, and (particularly with sepsis) collections of neutrophils in capillaries. n
The most characteristic finding is the presence of hyaline membranes, particularly lining the distended alveolar ducts. - Such membranes consist of fibrinrich edema fluid admixed with remnants of necrotic epithelial cells. a.
In the organizing stage there is a. marked proliferation of type II pneumocytes in an attempt to regenerate the alveolar lining. b. Resolution is unusual; more commonly there is organization of the fibrin exudates, with resultant intra-alveolar fibrosis. n
n - - Clinical Course Approximately 85% of patients develop the clinical syndrome of acute lung injury or ARDS within 72 hours of the initiating insult. Despite improvements in supportive therapy the mortality rate among ARDS cases seen yearly is still about 60%.
Predictors of poor prognosis in ARDS include : a. advanced age, b. underlying bacteremia (sepsis), c. and the development of multisystem (especially cardiac, renal, or hepatic) failure. -
- - If the patient survive the acute stage, diffuse interstitial fibrosis may occur and continue to compromise respiratory function. However, in most patients who survive the acute insult and are spared the chronic sequela, normal respiratory function returns within 6 to 12 months