Acute Arthritis Dr Mge Bakgil Kalayc Acute Arthritis

Acute Arthritis Dr. Müge Bıçakçıgil Kalaycı

Acute Arthritis • The sudden onset of inflammation of the joint, causing severe pain, swelling, and redness. • Structural changes in the joint itself may result from persistence of this condition.

Signs of Inflammation • Swelling • Warmth • Erythema • Tenderness • Loss of function

Key Points • Distinguish arthritis from soft tissue non articular syndromes • If the problem is articular distinguish single joint from multiple joint involvement • Inflammatory or non-inflammatory disease • Always consider septic arthritis!

Is it an articular or extra-articular problem? • ARTICULAR PERI-ARTICULAR • • • pain in plane of tendon active > passive linear swelling localised tenderness localised erythema/heat pain all planes active = passive capsular swelling/effusion joint line tenderness diffuse erythema/heat

Arthritis, Bursitis is NOT arthritis Prepatellar bursitis

Olecranon bursitis
 Swelling Erythema Warmth AM stiffness")
Inflammatory Vs. Noninflammatory Feature Inflammatory Noninflammatory Pain (when? ) Swelling Erythema Warmth AM stiffness Systemic features î ESR, CRP Synovial fluid WBC Examples Yes (AM) Soft tissue Sometimes Prominent Sometimes Frequent WBC >2000 Septic, RA, SLE, Gout Yes (PM) Bony Absent Minor (< 30 ‘) Absent Uncommon WBC < 2000 OA, AVN

History • Eye and mouth dyrness • Raynauds • Photosensitivity • Oral and genital ulsers • Recurrent swelling of parotis • Recurrent thrombophlebitis • Recurrent abortus • Uveitis

History n Inflamatory back pain n Epilepsy history, cerebro-vascular events n depression n Muscle weakness n Recurrent fever n Skinrash n Recurrent serosits

• INFLAMMATION • Acute/chronic • Monoarthritis • Oligoarthritis • Polyarthitis

• Is it acute or chronic? < 6 weeks Acute > 6 weeks chronic • Minutes to hours : hemarthrosis • Hours to days: septic, reactive, crystals • Days to weeks: autoimmune ( RA), CTD, viral • Weeks to months: degenerative, other
 in one joint • Occasionally polyarticular diseases")
Acute Monoarthritis • Inflammation (swelling, tenderness, warmth) in one joint • Occasionally polyarticular diseases can present with monoarticular onset: (RA, JRA, Reactive and enteropathic arthritis, Sarcoid arthritis, Viral arthritis, Psoriatic arthritis)
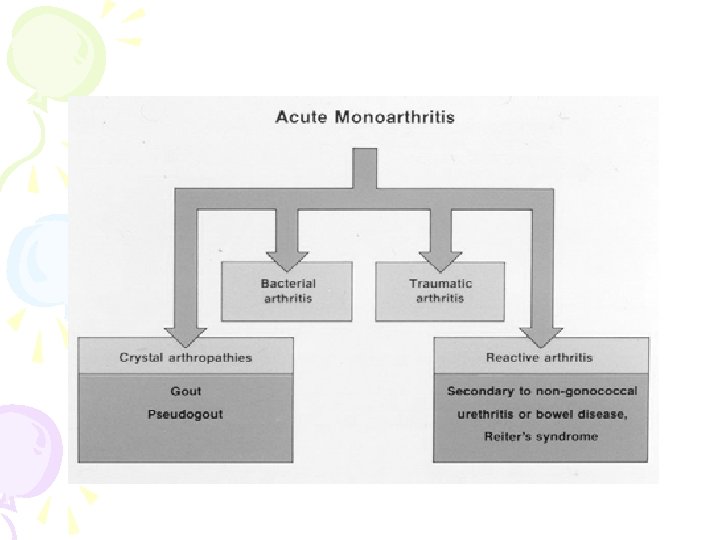

Acute Monoarthritis Etiology • THE MOST CRITICAL DIAGNOSIS TO CONSIDER: INFECTION ! • Septic • Crystal deposition (gout, pseudogout) • Traumatic (fracture, internal derangement) • Other (hemarthrosis, osteonecrosis, presentation of polyarticular disorders)

• Joint aspiration must be done! • Needed for immediate diagnosis. • Bloody joint aspirate- plain X-ray. • Analysis of synovial fluid provide discrimination of infection and crystal artropathy.

septic arthritis • • common organisms Staphylococci or Streptococcus young adults, significant incidence gonococcal arthritis Elderly & immunocompromised gram (-) organisms Anaerobes more common with penetrating trauma

Who gets septic arthritis? • pre-existing joint disease • prosthetic joints • low SE status, IV drug abuse, alcoholism • diabetes, steroids, immunosuppression • previous intra-articular steroid injection

Symptoms & signs of septic arthritis • Typically hot, swollen, red tender joint with reduced range of movement, difficulty weight bearing • Systemic upset • Night and rest pain • Large joints more commonly affected than small

Symptoms & signs of septic arthritis • Delayed or inadequate treatment leads to irreversible joint damage • 10 -15% of cases, > one joint - so polyarticular presentation does not exclude septic arthritis • presence of fever not reliable indicator- if clinical suspicion high – treat • Delayed or inadequate treatment leads to irreversible joint damage

Investigations • Synovial fluid aspiration – volume/viscosity/cellularity/a ppearance – gram stain/culture – Absence of organism does not exclude septic arthritis – polarised light microscopy (crystals) – suspected prosthetic joint sepsis should ALWAYS be referred to orthopaedics

Septic Joint - Gonococcal • Often preceded by disseminated gonococcemia • Sexually active individual, fever, chills, skin lesions, migratory arthralgias and tenosynovitis persistent monoarthritis • Genitourinary disease often asymptomatic

Disseminated Gonococcemia – Pustules

Tests to Perform on Synovial Fluid • Gram stain and cultures. • Total leukocyte count/differential: inflammatory vs. non-inflammatory. • Polarized microscopy to look for crystals. • Not necessary routinely: Chemistry (glucose, total protein, LDH) unlikely to yield helpful information beyond the previous tests.

Normal OA RA/Infl Septic Appearanc e Clear Opaque Viscosity High Low WBC/mm <200 200 -10. 000 2000 -75000 >30. 000 %PM <25% <50% >75%

Urate crystals Gram positive coccus

Investigations • Always blood cultures • significant proportion blood cultures + ve in absence of + synovial fluid cultures • FBC ESR & CRP • BUT absence of raised WBC, ESR or CRP not exclude diagnosis of sepsis if clinical suspicion high always treat

Other investigations • CRP useful for monitoring response to treatment • Urate may be normal in acute gout and of no diagnostic value in acute gout or sepsis • Measure urea, electrolytes & liver function for end organ damage (poor prognostic feature) • Renal function may influence antibiotic choice

Other tests? • If skin pustule is present, suggestive of gonococcal infection, then skin swab should be taken • If history suggests possibility of genitourinary or respiratory tract infection then culture sputum (and CXR) & urine & take anogenital & throat swabs where appropriate

Questions to Ask – History Helps in DD • Pain come suddenly, minutes? – fracture. • 0 ver several hours or 1 -2 days? – infectious, crystals, inflammatory arthropathy. • History of IV drug abuse or a recent infection? – septic joint. • Previous similar attacks? – crystals or inflammatory arthritis. • Prolonged courses of steroids? – infection or osteonecrosis of the bone.

Imaging • Plain X rays no benefit in diagnosis but form baseline for any future joint damage. May show chondrocalcinosis. • MRI useful in distinguishing sepsis from OA but less good between sepsis & inflammation • MRI sensitive for osteomyelitis

Antibiotic treatment of septic arthritis • Local and national guidelines • Liaise with micro. guided by gram stain • Conventionally given iv for 2 weeks or until signs improve, then orally for around 4 weeks

Joint drainage & surgical options • medical aspiration, surgical aspiration via arthroscopy or open arthrotomy • Suspected hip sepsis – early orthopaedic referral – may need urgent open debridement

Gout • Caused by monosodium urate crystals • Most common type of inflammatory monoarthritis • Typically: first MTP joint, ankle, knee • Pain very severe • May be with fever and mimic infection • The cutaneous erythema may extend beyond the joint and resemble bacterial cellulitis

Acute Gouty Arthritis

Risk Factors • Primary gout: Obesity, hyperlipidemia, diabetes mellitus, hypertension, and atherosclerosis. • Secondary gout: alcoholism, drug therapy (diuretics), myeloproliferative disorders, chronic renal failure.

Urate Crystals • Needle-shaped

CPPD Crystals Deposition Disease • Can cause monoarthritis clinically indistinguishable from gout – Pseudogout. • Pseudogout is most common in the knee (50%) and wrist. • Reported in any joint (Including MTP). • CPPD disease may be asymptomatic (deposition of CPP in cartilage).
 Rod or rhomboid-shaped Weakly positive birefringent")
Ca pyrophosphate (pseudogout) Rod or rhomboid-shaped Weakly positive birefringent

What are other differentials for acute monoarticular pain?

Monoarthritis - differential diagnosis Psoriatic arthritis – Onycholysis – Subungual hyperkeratosis – Pitting – Extensor surfaces, scalp, umbilicus

Monoarthritis - differential diagnosis Reactive arthritis • Prodromal GI /GU Infection eg campylobacter, salmonella, shigella, Yersinia, chlamydia • Pustular psoriasis and circinate balanitis
 – Palindromic rheumatism")
Monoarthritis - differential diagnosis – Trauma and haemarthroses (warfarin, bleeding disorders) – Palindromic rheumatism – 24 -48 hours inflammatory monoarthritis, can evolve into polyarthritis eg RA

Other Tests Indicated for Acute Arthritis • 1. Almost always indicated: – Radiograph, bilateral – CBC • 2. Indicated in certain patients: – Cultures – PT/PTT – ESR – Serum Uric acid level • 3. Rarely indicated: – Serologic: ANA, RF

Acute Inflammatory Oligoarthritis • A patient with 2 -4 joints is said to have pauci- or oligoarticular arthritis

Differential diagnosis of acute inflammatory oligoarthritis • Infection – Disseminated gonococcal infection – Nongonococcal septic arthritis – Bacterial endocarditis – Viral • Postinfection – Reactive arthritis – Rheumatic fever (post strep) • Spondyloarthropathy • Ankylosing spondylitis • Psoriatic arthrit • Inflammatory bowel disease • Oligoarticular presentation of RA, SLE, still disease • Gout and pseudogout
 GIT : Campylobacter, Yersinia, Salmonella, Shigella")
Acute Inflammatory Oligoarthritis Reactive arthritis ( Re. A) GIT : Campylobacter, Yersinia, Salmonella, Shigella Genitourinary: Chlamydia, Gonococcus Throat: β hemolytic streptococcus
 Typical joints: DIPs, big and")
Acute Inflammatory Oligoarthritis Psoriasis associated arthritis ( Ps. A) Typical joints: DIPs, big and small together

Polyarthritis • Inflammation of 5 or more joints • Diagnosis cannot always be made • with certainty in <6 weeks • Bacterial infection less likely but • viruses common cause of acute polyarthritis

Acute Polyarthritis • • • Infection Gonococcal Meningococcal Rheumatic fever Bacterial endocarditis • Viral (rubella, parvovirus, Hep. B) • • Inflammatory RA JRA SLE Reactive arthritis Psoriatic arthritis Polyarticular gout Sarcoid arthritis
 • Additive")
Temporal Patterns in Polyarthritis • Migratory pattern: Rheumatic fever, gonococcal (disseminated gonococcemia) • Additive pattern: RA, SLE, psoriasis • Intermittent: Gout, reactive arthritis

Patterns of Joint Involvement • Symmetric polyarthritis involving small and large joints: viral, RA, SLE, one type of psoriatic (the RA-like). • Asymmetric, oligo- and polyarthritis involving mainly large joints, preferably lower extremities, especially knee and ankle : reactive arthritis, one type of psoriatic, enteropathic arthritis. • DIP joints: Psoriatic.

Viral Arthritis • Younger patients • Usually presents with prodrome, rash • History of sick contact • Polyarthritis similar to acute RA • Prognosis good; self-limited • Examples: Parvovirus B-19, Rubella, Hepatitis B and C, Acute HIV infection, Epstein-Barr virus, mumps

Viral Arthritides - Parvovirus

Rheumatoid Arthritis • Symmetric, inflammatory polyarthritis, involving large and small joints • Acute, severe onset 10 -15 %; subacute 20% • Hand characteristically involved • Acute hand deformity: fusiform swelling of fingers due to synovitis of PIPs • RF may be negative at onset and may remain negative in 15 -20%! • RA is a clinical diagnosis, no laboratory test is diagnostic, just supportive!

Acute Polyarthritis - RA

Acute Sarcoid Arthritis • Chronic inflammatory disorder – noncaseating granulomas at involved sites • 15 -20% arthritis; symmetrical: wrists, PIPs, ankles, knees • Common with hilar adenopathy • Erythema nodosum • Löfgren’s syndrome: acute arthritis, erythema nodosum, bilateral hilar adenopathy

Acute Polyarthritis in Sarcoidosis

Reactive Arthritis • Infection-induced systemic disease with inflammatory synovitis from which viable organisms cannot be cultured • Association with HLA B 27 • Asymmetric, oligoarticular, knees, ankles, feet • 40% have axial disease (spondylarthropathy) • Enthesitis: inflammation of tendon-bone junction (Achilles tendon, dactylitis) • Extraarticular: rashes, nails, eye involvement

Enthesitis in Reactive Arthritis
 is rarely polyarticular. • Tophi develop")
Polyarticular gout • Pseudogout ( Calcium pyrophosphate mono/oligo) is rarely polyarticular. • Tophi develop with time. • Joint aspiration ( 5% gouty arthritis normouricaemic during attack)

Diagnostic criteria for SLE ARA 1985 • • • Photosensitity • Raynaud’s • maculopapular rash • polyarthritis • serositis • Cytopenias • Coomb’s pos haem. anemia • haematuria or proteinuria • CNS • Pos ANA, SSA, anticardiolipin, LAC • Pos double stranded DNA

SLE-skin and joints Butterfly rash Rash and arthritis Muco-cutaneous Photosensitive alopecia
 • • FULL HISTORY AND PHYSICAL")
Work-up of Acute Arthritis – Polyarthritis (>5 joints) • • FULL HISTORY AND PHYSICAL EXAM. FBC, biochemistry CRP, ESR RF, CCP (filaggrin) , ANA (DNA , ENA if pos) • Serology for: parvovirus, Hep B and C, Borrelia • X ray both hands and feet (erosions), chest • Blood cultures and Echocardiogram
 (+)")
Monoarthritis Detailed history end Physical exammination X-ray trauma or focal bone pain (-) (+) Fracture, tm Synovial fluid WBC>2000 PMNL> %75 (-) Non-inflammatuar Soft Tissue trauma Osteoarthritis Osteonecrosis Mechanical problem Bloody Coagulopathy malignancy Trauma (+) İınflammatuar arthrritis Culture (+) Septic arthritis Crystal (+) Crystal arthritis Steril inflamatuar fluid RA, JIA, Sp. A, FMF, Behçet, SLE
 (+) FMS, , myofasial pain, tendinitis")
Polyarthritis-polyarthralgia Detailed history and physical examination Poliartthritis (-) (+) FMS, , myofasial pain, tendinitis Tender points (+) (-) Symptom duration >6 week (+) (-) Viral arthralji, osteomalasia, hypotyroid, malignancy, PMR, depression Viral arthritis, ARA Systemic rheumatological diseases, systhemic rheumatological diseases Osteoarthritis Further investigation Complate blood count, urine analysis, ESR, CRP, RF, ANA ASO, LFT, Hepatitis B, C, radiology viral arthralgia, throat culture

• Management �Dependent upon diagnosis �If infection cannot be excluded must treat as infection �May need supportive care until symptoms resolve �Persistent symptoms require treatment plan
- Slides: 67