Acute Applications of Noninvasive ventilation NIV and its
 and its special application in SARS Dr Arthur")













 Nasal Face Helmet Pillows Total FM Amount")








 n n Multi-centre, prospective, observational study screened all patients admitted")






")

 vs CPAP")

 and Cochrane")












 and EMBASE (1990 to")


 vs standard therapy(20) – Solid organ")

- Slides: 57
Acute Applications of Noninvasive ventilation (NIV) and its special application in SARS Dr Arthur Chun-Wing LAU 刘俊颖 Associate Consultant, Department of Intensive Care & Honorary Associate Consultant, Division of Respiratory and Critical Care Medicine, Department of Medicine 香港东区尤德夫人那打素医院 Pamela Youde Nethersole Eastern Hospital Hong Kong SAR, China 29 Apr 2006
Objectives 1. 2. 3. To know about the practical aspects of NIV Literature review of the application and efficacy of NIV in various acute clinical conditions, including SARS Predictors of NIV failure in general
General benefits of NIV 1. 2. 3. 4. Avoid complications of endotracheal tube intubation Reduce ventilator-associated pneumonia (VAP) Improve clinical outcomes (morbidity, mortality, ICU and hosp LOS, costs) Patient comfort
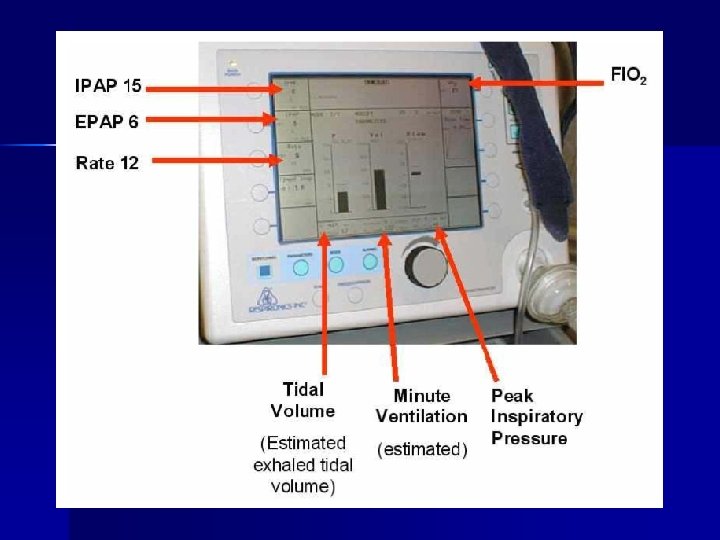
Practical aspects
Initiation of NPPV Ventilator type n Facial appliance as interface n Explain to patient n Adjust ventilatory pressures depending on clinical requirement n
ICU ventilators Siemens Servo i Viasys Avea Draeger Evita 4 Puritan Bennett 840
Hybrid ventilators Viasys Vela Bird VSO 2
Home ventilators Respironics Bi. PAP Vision Breas LTV 1000 Versamed i. Vent Breas PV 102 Sirio NIV-S
Ventilators ICU vent ilato rs Hybr id vent ilato rs Insp indep /exp ende lines nt nt Flow, 150 120 L/mi 140 n Soft comp easy Hom e vent ilato rs singl e < 120 easy
Factors to consider n n n “Hybrid” and “ICU” ventilators (independent inspiratory and expiratory line) are to be preferred for NIV in more severe patients Ventilator setting and ventilator’s performance depend on the interface (mask or helmet) BIPAP is to be preferred when helmet is used
Facial appliance Some facial appliance designed for specific NIV ventilators n For acute hypercapnia, low dead space volume and minimal leak essential n
Facial Nasal pillow Total face
Helmet Nasal prong device
Studies comparing interfaces Navalesi et al. CCM 2000; 28: 1785 n Kwok et al. CCM 2003; 31: 468 n Anton et al. RC 2003; 48: 919 n Antonelli Anes 2004; 100: 16 n
Masks (1: a little; 4: a lot) Nasal Face Helmet Pillows Total FM Amount of Ventilation 2 3 1 2 2 Claustrophobia 2 3 2 1 3 Ease to speak 3 1 4 3 2 Ease to cough 3 1 4 3 2 Air leak 3 2 1 3 1 Dead space 2 2 4 1 3 Comfort 2 1 4 3 2
Exhalation device 1. 2. In mask In circuit a. Whisper-Swivel b. Whisper-Swivel II c. Plateau valve Whisper-Swivel II, Respironics
No difference in daytime arterial blood gas levels, pulmonary functions, nocturnal vital signs or oximetry, or Ptc. CO 2 N = 7 only Hill N, et al 2002; 122: 84
Position of exhalation port and CO 2 rebreathing n Compare: n DESIGN: Lung model evaluation. Results: Facial-MEP with its exhalation port within the mask and the smallest mask volume demonstrated less rebreathed CO 2 Additional studies are necessary to confirm if mask design can clinically affect patient's inspiratory effort during noninvasive positive pressure ventilation. n n 1. A facial mask (inner volume of 165 m. L) with exhalation port within the mask (Facial-MEP) 2. Same facial mask with exhalation port in the ventilator circuit (Facial-WS) 3. Total face mask with exhalation port within the mask (inner volume 875 m. L, Total Face) Schettino GP, et al. Crit Care Med. 2003 Aug; 31(8): 2178 -82
Exhalation device
Humidification n n High flows and high FIO 2 result in dried retained secretions Use heated pass over humidifier
Literature review
Use of NIV in acute respiratory failure Prospective international study of all consecutive ICU patients requiring >12 hours MV (non-invasive and invasive) n 5183 patients (from 15757 total patients) n NIV used in 4. 9 n Esteban, A. et al. JAMA 2002; 287: 345 -355.
Ventilator Modes Used Each Day During the Course of Mechanical Ventilation Esteban, A. et al. JAMA 2002; 287: 345 -355.
NIV in ARF (2) n n Multi-centre, prospective, observational study screened all patients admitted to 16 ICU’s over a 2 month period in mid-2003 in Australia and New Zealand Non-intubated patients with hypoxemic ARF (except COPD and cardiogenic pulmonary edema) 200/1156 had hypoxemic ARF NIV was used in 77 (38. 5%) initially Bersten A, et al. ICM 2004; 30: S 5
Clinical conditions 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. COPD Acute cardiogenic pulmonary edema (CPE) Hypoxemic respiratory failure (ARF) Pneumonia Immunosuppressed with ARF ALI/ARDS Post-operative ARF Asthma Chest trauma Post-extubation ARF Weaning from mechanical ventilation SARS
COPD
COPD n n Largest RCT: 236 patients, multicentre, NIV vs standard therapy Plant P, et al. Lancet 2000; 355: 1931
Endotracheal intubation Keenan et al. Annals of Int Med 2003; 138: 861
Hospital mortality Keenan et al. Annals of Int Med 2003; 138: 861
Non-invasive positive pressure ventilation for treatment of respiratory failure due to exacerbations of chronic obstructive pulmonary disease - metaanalysis n Fourteen studies – – – – decreased mortality decreased need for intubation reduction in treatment failure rapid improvement within the first hour in p. H Pa. CO 2 dec respiratory rate dec complications associated with treatment reduced length of hospital stay was also reduced Ram FSF et al. Cochrane Database of Systematic Reviews. 1, 2006
Cardiogenic pulmonary edema (CPE)
Cardiogenic pulmonary edema n Initial RCT: – 39 patient RCT of CPAP 10 cm. H 2 O vs standard therapy – CPAP patients had n Improved respiratory rate, oxygenation and Pa. CO 2 n Dec intubation rate 0% vs 35% (p -= 0. 01) Bersten A, et al. NEJM 1991; 325: 1825
CPE: NIV complicated by AMI? 27 patient RCT of Bi. PAP (15/5) vs CPAP (10/10) n AMI rate higher in Bi. PAP gp, study thus terminated n No difference in rates of intubation, hypotension or mortality n Mehta S, et al. Crit Care Med 1997; 25: 620
CPE: meta-analysis Bi. PAP vs CPAP n No effect on n – Mortality – Need for intubation – Duration of hospital stay – Trend toward increased new AMI with Bi. PAP n RR 1. 5 (95%CI 0. 9 – 2. 5), p = 0. 12 Peter J, Moran J, et al. ANZICS ASM 2005, p 113
CPE: metaanalysis n n MEDLINE and EMBASE (from inception to October 2005) and Cochrane databases (library issue 4, 2005) were searched to identify relevant randomized controlled trials and systematic reviews published from January 1, 1988, to October 31, 2005. Conclusions – NIV reduces the need for intubation and mortality in patients with acute cardiogenic pulmonary edema – Although the level of evidence is higher for CPAP, there are no significant differences in clinical outcomes when comparing CPAP vs NIPSV. Masip J, et al. JAMA. 2005; 294: 3124 -3130
Masip J, et al. JAMA. 2005; 294: 31243130
Masip J, et al. JAMA. 2005; 294: 31243130
Masip J, et al. JAMA. 2005; 294: 31243130
How about CPE with hypercapnia? n n Hypothesis: CPE + inc PCO 2 = ? muscle fatigue, so BIPAP more helpful than CPAP Randomized prospective study in an emergency department in patients with acute pulmonary edema and arterial hypercapnia (Pa. CO(2) >45 mm. Hg) NIPSV (n=18) vs CPAP through a face mask (n=18). Conclusion: NIPSV as effective as CPAP, did not improve resolution time. Bellone A, et al. ICM 2005; 31: 807 - 811
Another meta-analysis n Comparing NIPPV and CPAP on n 23 trials (out of 43160 articles screened) fulfilling inclusion criteria Conclusions: n – Hospital mortality – Need for mechanical ventilation – CPAP and bilevel ventilation reduces the need for subsequent mechanical ventilation and reduces mortality – also suggest a trend towards reduced mortality after bilevel NIPPV. Peter JV, et al. Lancet 2006; 367: 1155– 63
Need for invasive mechanical ventilation Peter JV, et al. Lancet 2006; 367: 1155– 63
Mortality Peter JV, et al. Lancet 2006; 367: 1155– 63
Hypoxemic ARF n A mixed bag of diagnoses
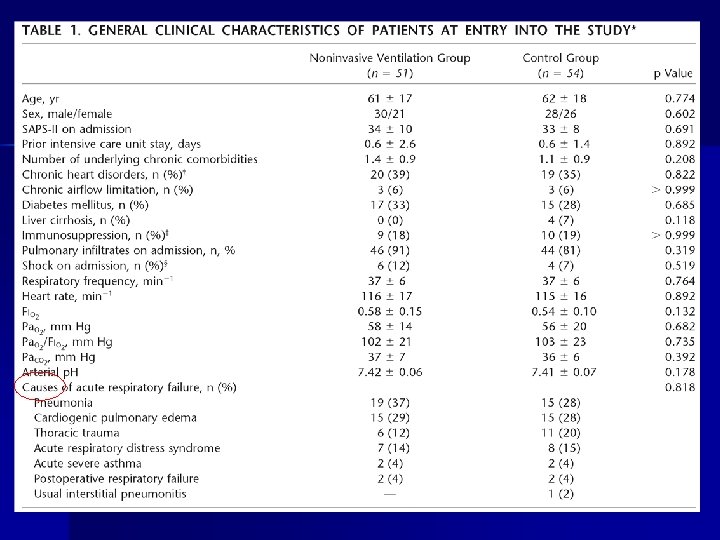
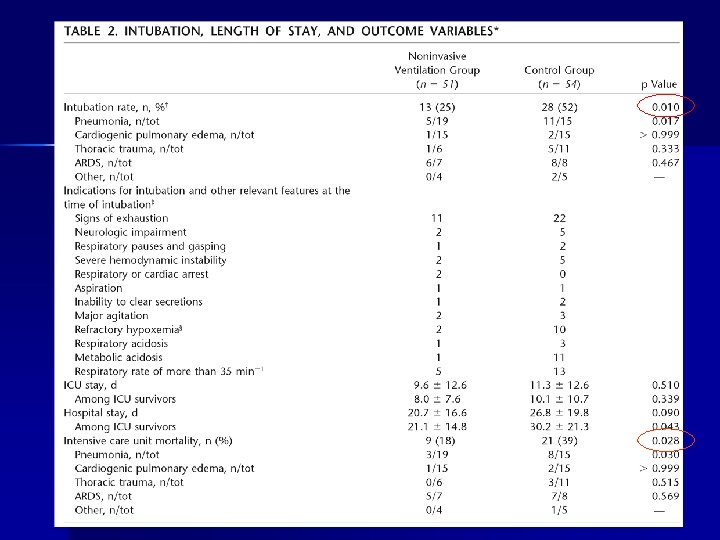
Hypoxemic ARF: RCT 64 patient RCT of NIV vs ETT n NIV group: n – 30% were intubated – Dec ICU stay (9 vs 16 days, p = 0. 04) – Similar hospital mortality – Dec serious complications – Dec pneumonia or sinusitis Antonelli M, et al. NEJM 1998; 339: 429
Antonelli M, et al. NEJM 1998; 339: 429
Hypoxemic ARF: RCT 105 patient RCT of oxygen vs NIV (IPAP 10 – 12 & EPAP 5 – 6) n NIV group had decreased n – Intubation requirement (25% vs 52%, p = 0. 01) – Septic shock (12% vs 31%, p = 0. 03) – ICU mortality (18% vs 39%, p = 0. 03) Ferrer M, et al. AJRCCM 2003; 168: 1438
Ferrer M, et al. AJRCCM 2003; 168: 1438
Hypoxemic ARF: metaanalysis n n MEDLINE (1980 to October 2003) and EMBASE (1990 to October 2003) The addition of NPPV to standard care in the setting of acute hypoxemic respiratory failure – – n n reduced the rate of endotracheal intubation ICU length of stay ICU mortality effect on mortality is less clear Heterogeneity found among studies suggests that effectiveness varies among different populations: Conclusion: the literature does not support the routine use of NPPV in all patients with acute hypoxemic respiratory failure. Keenan S, et al. CCM 2004; 32(12): 2516
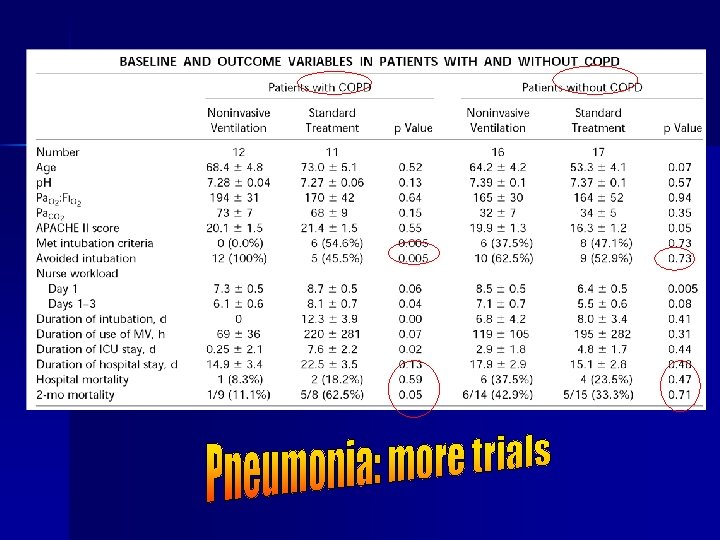
Pneumonia
Pneumonia: RCT n 56 patient RCT of NIV vs standard therapy n NIV patients had n – Severe CPAP – Same antibiotics and O 2 targets – Set criteria for intubation – – Dec intubation rate Dec ICU LOS Hospital stay and mortality similar Nursing workload similar BUT: benefit lost if COPD patients (40% of patients) were excluded Confalonieri M, et al. AJRCCM 1999; 160: 1585
Immunosuppressed ARF n 40 patient RCT of NIV(20) vs standard therapy(20) – Solid organ transplant patients – Respiratory distress – Intermittent NIV n NIV group – – n Inc P/F ratio at 1 hr Dec intubation rate Dec rate of severe sepsis Dec ICU mortality Hospital mortality: same Antonelli M, et al. JAMA 2000; 283: 235
Timing of Endotracheal Intubation in the 2 Groups Changes in the Ratio of Pa. O 2 to Fraction of Inspired Oxygen (FIO 2) and Pa. CO 2 Over Time Antonelli, M. et al. JAMA 2000; 283: 235 -241.