Acute abdomen Acute abdomen sudden severe abdominal pain

Acute abdomen

Acute abdomen- sudden severe abdominal pain • • sudden rapid progress Typically requires timely surgery intervention Causes may result in death, heavy complications, lifelong consequences/complications

ACUTE ABDOMEN Non- injury acute abdomen • Inflammation • Ileus mechanic ileus neurogen ileus vascular ileus • Gastrointestinal bleeding • Gynecological • Perioperative Injury acute abdomen • Gastrointestinal perforation • Hemoperitoneum • Mixed form Perforation + hemoperitoneum

Symptomatology of acute abdomen SUBJECTIVE symptoms OBJECTIVE symptoms • PAIN • Behavior and posture of patient • Face of patient Waring-Griffith sign -visceral- organ, splanchnic, vegetative nerves , colic pain, no exact localization -somatic- irritation of the peritoneum, the exact localization, has a point of maximum intensity • NAUSEA, VOMITING • No passage (flatulence, stool), melena, enterorhagia • Another: hiccups, dysuria, weakness. . . - Halsted sign - Walzelovo sign • Pulse • Temperature - Lennander sign

EXAMINATION • • HISTORY TAKING Clinical examination Blood test X-ray Ultrasound CT, MRI Endoscopic Laparotomy
 Causes:")
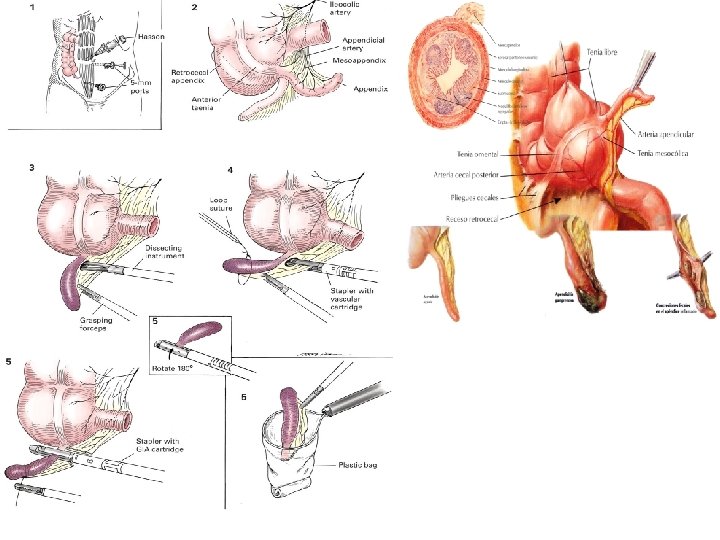
• Appendicitis acuta- 7 -10% of population, (inflamamtion cataral, phlegmonous, gangrenous, perforans) Causes: obstruction of lumen, inflammatory bowel disease, foreign bodies, rarely hematogenous infection Sign and symptoms: abdominal pain, nausea, vomiting, fever, worse pain when walking, movement, cough Appendicitis in children, 90% of acute abdomen in children, DG: anamnesis, physical examination , Lennander sign. Plenies, Blumberg, Rovsing, FW, CRP, leu, USG

• Positio - retrocaecalis 64% pelvina 32% retrolaterocaecalis 2% mediocaecalis preilealis 1% mediocaecalis retroilealis 0. 5% • Complications: Periappendicitis Periappendicular infiltrate Perforation Difusse peritonitis Pylephlebitis • Therapy: surgical therapy, surgical revision is indicated always when appendicitis cannot be safely ruled out

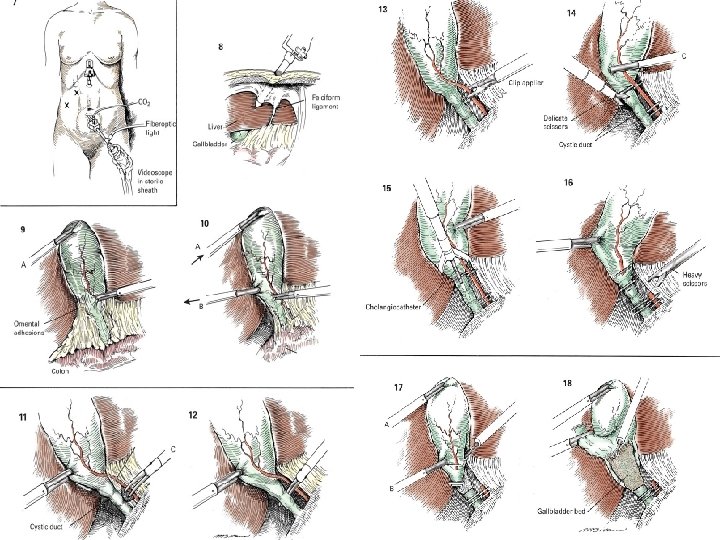
Cholecystitis acuta • Sign and symptoms: 75% previous biliary colic, fever, nausea, vomiting, 10% subicteric, Murpyho sign, leucocytosis, elevation Bil, ALP, GMT, X-ray can detect lithiasis in 20% people, USG, • Complications: empyema, gangrene, perforation, pancreatitis. . … • Treatment: Disunity, in 60 -70% cases spontaneously cure managment based on observation, wait, plan elective cholecystectomy, urgent surgery intervention when there are some complipations of conservative treatment, patient signs and symptoms. . • Conservative tretment: NPO, spasmolytics, analgetics, compress… • Acute cholechystectomy: It is recommended to 72 h from the onset of the first symptoms , in the beginning of illness are not anatomic -Urgent cholecystectomy- risk of perforation

Peptic ulcer perforation • Anamnesis, severe initial pain, tachycardia, symptomatology: 1, severe initial pain (2 -4 h) 2, relative improvement of patient – feels better (2 -6 h) 3, peritonitis signs • E: HCl, insufficient mucosal protection, h. pylori Peptic Ulcer (G+D, esophagus, GEA, Meckel diverticulum. ) Perforation – 0. 5% people with peptic ulcer 10 x more men than women. Perforation is usually on the front site of stomach, on rear wall is tendency to penetrate and bleed

• S +DG: 80% of patients have positive history of ulcer, sudden pain in epigastrium, nausea, vomiting, hematemesis, preventing to movement, severe pain is reaction – chemical irritation of peritoneum ( gastric acid, pancreatic, bile…) , tachycardia, defense, percussion pain, leucocytosis… X-ray (pneumoperitoneum- may be not detected in 20 -30%, particularly in duodenal perforation) Treatment: covered perforation - conservative (parenteral nutrition, nasogastric intubation, compression, antagonist H 2 Rc. , PPI, antacid), surgical intervention

Diverticulitis acuta • About 60% of population in aduldhood have diverticulosis. They usually do not know about it, they often come to hospital with first attack of disease. • Sign and symptoms: sudden pain in left lower abdomen, beginning- colic pain, enterorhagia, fever, leucocytosis, CRP, X- ray, CT • Diff Dg: adnexitis, metritis, perforated tumor • Treatment: observance, full parenteral nutrition, rifaximine, draining, resection, Hartman op. ,

Pancreatitis acuta • Acute inflamation of pancreas, sudden pain in epigastrium, nausea, vomiting, elevation AMS, LPS, Leu, CRP, History - diet mistake alcoholol (60%) Biliary tract disease(30%) • Men 30 -50 yr. , increasing in young - 80% edematosus inflammation - 20% heavy inflammation form - necrosis • Treatment depends on the presence of infection

• Sign and symptoms: sudden pain in epig. , cyanotic, cold sweat, tachycardia, hypotension, subicterus- can be History (diet, alcohol, cholecystopathy, ), nausea, vomiting (no relief), no gas and after 48 hours (Cullen sign, Grey Turner sign ), pain in midle or left upper abdomen, in next days diffuse pain, maximum of pain is still in epigastrium, sometimes resistance can be palpable. LPS, AMS, Br, ALP, GMT, AST, LDH, l eu, CRP, Ca, disorder of glucose toleration , USG, Bathazar scale -A normal -B focal of diffuse expansion of pancreas -C and D inflammatory changes of pancreas and neighbouring structures -E large collections of fluids around pancreas, and absceses

• DIFFERENTIAL DIAGNOSIS: ulcer perforation, ileus, mesenterial thrombosis/embolisation, myocardial infarct • Complication: pancreatic pseudocyst, peritonitis pancreatic absces, DM • Treatment: - conservative - NPO, treatment of shock, hypoxy, substitution of fluids, iont, watch average fluid intake/output, ERCP, (gabexymelisat), In severe courses ATB, creatinin over 400 umol/lhemodialysis, where is hyperglycemy over 11 mmol/l - insulinotherapy, DIC- heparin, vit K, frozen plasma, puncture, operation – revision…
- Slides: 16