Active Learning in PBL Why and How Mariam

Active Learning in PBL Why and How Mariam Shalaby and Ashley Wong, MS 2 s

Why active learning? - Reinforces important material, concepts, and skills Immediate feedback Opportunity to think, discuss, and process Information synthesized and processed with difficulty is retained longer

Barriers to active learning - No tablet/i. Pad for drawing*** Communicating over Zoom difficult Unsure what to do/would like to learn techniques

Principles - Co-create a learning product - - Slow down! - - Even a list of risk factors can be co-created Explaining and typing is better than copy+paste and reading Annotating an image is better than simply talking about it Ask curious questions Summarize!! Use brief and debrief periods wisely - Each group is unique There is plenty of time to experiment

Examples:

Zoom whiteboard Venn diagram: - Appendicitis - Ovarian cyst - Pelvic inflammatory disease

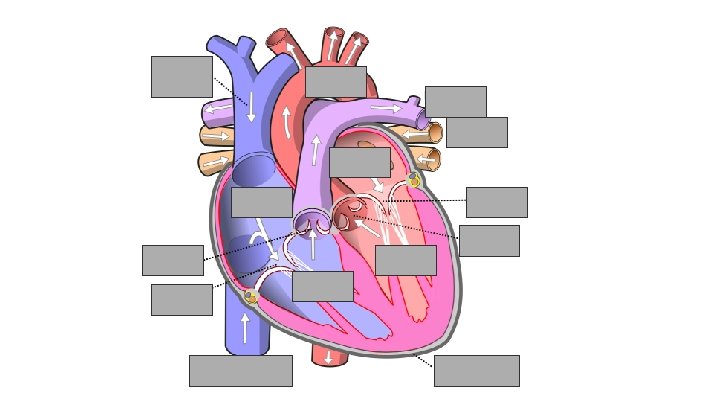
ARF Na+ ions in RRF K+ ions out threshold Resting membrane pot Hyperpolarization
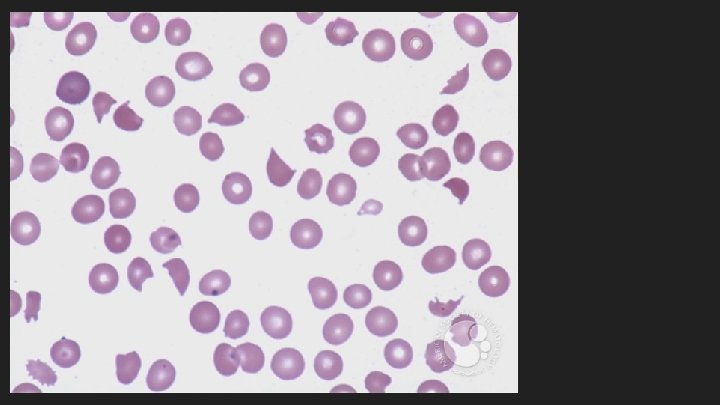

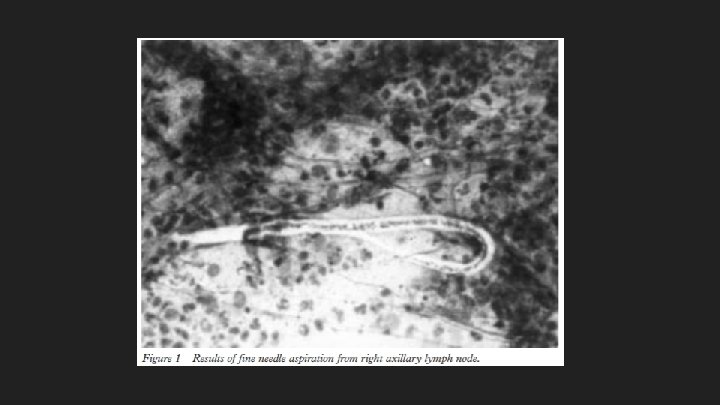
Differential: axillary mass Ddx: - Infection → lymphadenopathy Arm/hand wound Breast cancer Lymphoma Sebaceous cyst Fibroadenoma Axillary aneurysm A 60 year old women, a resident of Delhi, presented to the medical outpatient clinic with complaints of recurrent fever accompanied by chills, rigor, headache, and malaise. She had no complaints suggestive of respiratory or urinary tract involvement. She had been treated with antimalarials (chloroquine and sulfadoxinepyrimethamine), however, she continued to be febrile. Subsequently, the patient reported a painful lump in the right axilla accompanied by pain in the right upper limb. There was no history of nipple discharge or breast lump, local injury to the limb, insect bite, haemoptysis, or chest pain, loss of weight, bleeding diathesis, any skin rash, and urinary or bowel complaints. Past and family history were non-contributory. Physical examination revealed a conscious middle aged women, with normal pulse rate (80 beats/min) and blood pressure (140/80 mm Hg). Respiratory rate was 26 breaths/min and her body temperature was 39°C. She was anaemic; however, there was no jaundice, cyanosis, clubbing, and oedema. Bilateral axillary lymph nodes were enlarged, measuring 2 × 2 cm, firm, tender, and mobile. There was no lymph node enlargement elsewhere on the body. There was a tender, reddish streak on the medial aspect of right arm. Examination of breast and other systems was normal. With provisional diagnoses of streptococcal lymphangitis, tubercular lymphadenitis, secondaries from internal malignancy and primary lymphoma, the patient was subject to further investigations. Investigations revealed a haemoglobin of 128 g/l, total lymphocyte count of 7800/mm 3 , erythrocyte sedimentation rate of 30 mm/hour with eosinophilia (22% with an absolute count of 900/mm 3 ). Peripheral smear revealed no haemoparasites. All other investigations including chest radiography, a sonographic study of the abdomen, Mantoux test, and urinary and blood cultures were normal. Serum Ig. E concentrations were not measured as the investigation was not available to us when the patient presented. The results of a fine needle aspiration from one of the right axillary lymph nodes are shown in fig 1. Aspiration from the left axillary nodes revealed only non-specific lymphadenitis.

Summary of Examples - - Venn diagram - Ddx, compare and contrast, collaborative learning Fill-in-the-blank - Self-testing, fact recall, challenges your assumptions of understanding Annotated image - Slow down, make points clear, use >1 sense (listen, see, draw) Adjusting the differential - “Doctor thinking” via critical, dynamic analysis of a case

Conclusions - Active learning requires creativity online Research shows it improves learning and retention Many ways to overcome barriers to active learning Good luck!
- Slides: 13