ACTINOMYCETES NOCARDIA Dr Sathya Anandam ACTINOMYCETES Gram positve





















- Slides: 24
ACTINOMYCETES & NOCARDIA Dr Sathya Anandam
ACTINOMYCETES Gram positve, non motile, non sporing, non capsulated filamentous bacteria Thin bacteria with muramic acid cell wall. Superficial resemblance to fungi due to branching filaments. Related to Corynebacteria and mycobacteria
Includes genera: - Actinomyces, Arachnia, Bifidobacterium - Nocardia, Actinomadura, Streptomyces
ACTINOMYCES Soil saprophytes & commensals of oral cavity Cause actinomycosis - a chronic granulomatous disease Indurated swelling, suppuration and discharging of sulfur granules from sinuses. Later stage leads to fibrosis & tissue destruction Infection usually endogenous. A. israelli is the MC cause.
� The name refers to ray – like appearance of the organism in the granules( Actinomyces, meaning ray fungus) � Mode of infection: mostly endogenous & trauma e. g. dental extraction
Worldwide in distribution More common in rural areas and agricultural workers Young males 10 -30 yrs age group more common. Pelvic infection seen in women using intrauterine devices. Organism occurs as commensal in mouth, URT and female genital tract. Have low virulence
Pathogenesis � Enters the tissue, and bridges the mucosal or epithelial surface � Creates an anaerobic environment � Induces mixed inflammatory response � Forms painless indurated swelling with sinuses which may drain pus containing granules to the skin surface � Infection spreads to neighbouring organs with bone destruction
Clinical manifestations 4 clinical forms; 1. cervicofacial- lumpy jaw 2. Thoracic 3. Abdominal 4. Pelvic � Disseminated form- hematogenous spread Also associated with inflammatory disease of gums. Can also present as mycetoma The disease is characterised by presence of Sulfur granules in the exudate
Laboratory diagnosis Specimen- pus, sputum, BAL, biopsy Gross examination of granules Microscopy: pus discharge is washed thoroughly in saline in a test tube Sediment is collected which is crushed between two slides and smears are made
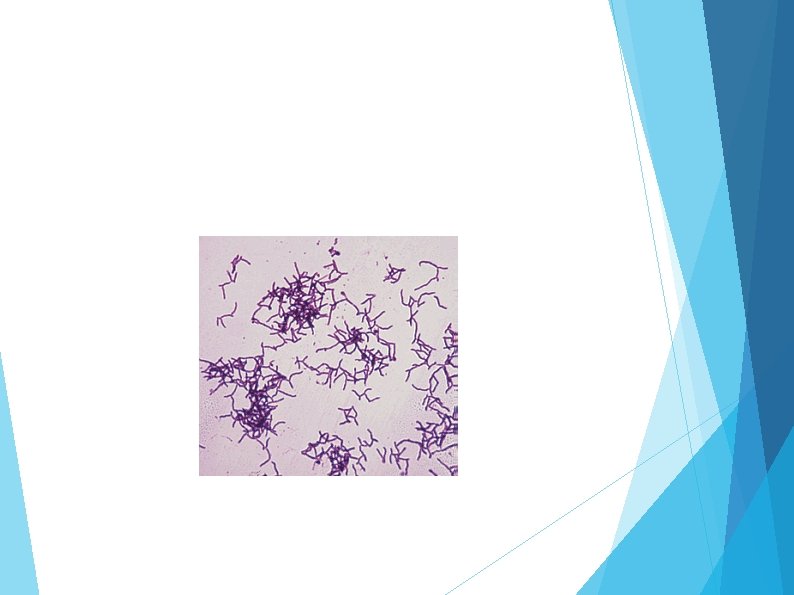
� Gram’s staining: shows a central mass of Gram positive filamentous bacilli, radiating peripherally with hyaline, club- shaped ends � Granules are hard and non emulsifiable � Fluorescent antibody techniques � Fluorescent in situ hybridization
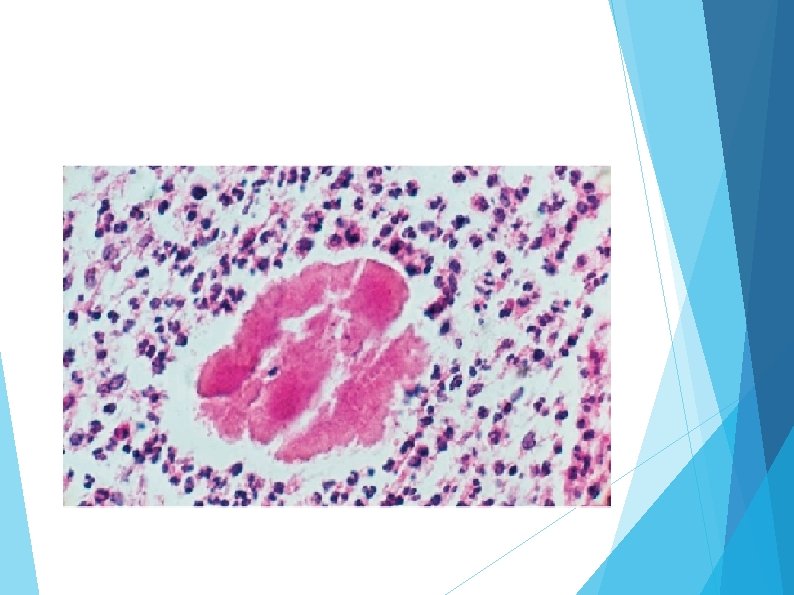
� Histopathological staining: H & E stain/ Gomori’s stain on tissue sections reveal � Granules composed of eosinophilic clubs surrounding basophilic filaments and inflammatory cells such as neutrophils & macrophages- sun ray appearance
Sulfur granules are white to yellow with siz ranging from minute specks to about 5 mm and are found only in tissue.
Isolation in culture- granules are washed and cultured anaerobically at 370 C on BHIA and Thioglycollate broth. A. israelli- small spidery colonies which become heaped up, white irregular or smooth and large in 10 days, on thioglycollate btoth fluffy balls at the bottom of tube Species identification
TREATMENT MEDICAL TREATMENT- prolonged treatment with penicillin or tetracycline for 6 -12 months to prevent relapse SURGICAL TREATMENT- drainage or excision
NOCARDIA � Gram positive branching filamentous bacilli � Aerobic and acid fast � PRESENT IN SOIL � Infection exogenous � Species associated N. asteroides, N. Brasiliensis and N. caviae
Pathogenesis � Worldwide, common in adult males � Inhalation of fragmented bacterial myceliapulmonary nocardia � Transcutaneous inoculation of bacteria- cutaneous/ sub cutaneous e. g mycetoma � Characteristic histological feature is an abscess with extensive neutrophilic infiltration & necrosis surrounded by granulation tissue
Risk factors � Opportunistic pathogen In immunocompromised host
NOCARDIA May be cutaneous, subcutaneous or systemic lesions in humans Pulmonary form is MC Occurs by inhalation of bacilli Common cause of pneumonia in immunocompromised hosts Disseminated nocardiosis- brain abscess Actinomycetoma: chronic granulomatous subcutaneous infection
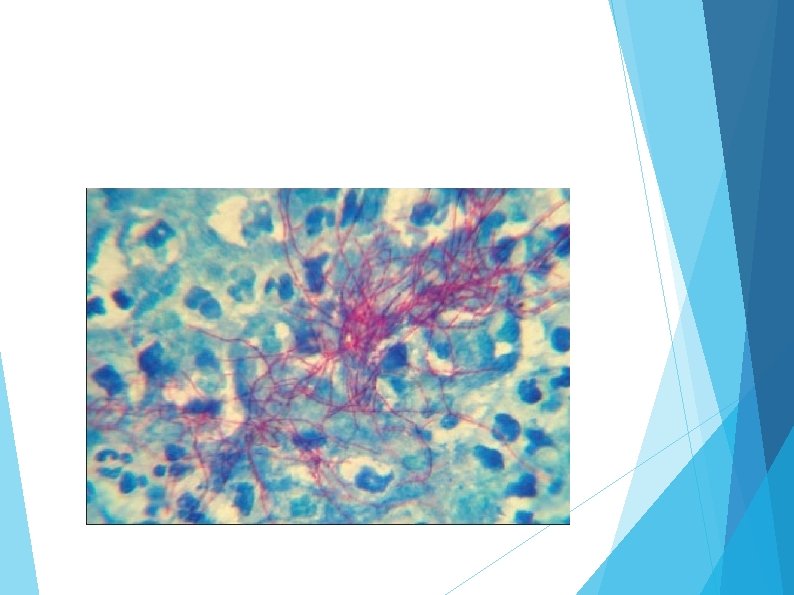
LABORATORY DIAGNOSIS • Specimen: sputum, pus • Macroscopic examination of pus • Granules are soft • Microscopy by Gram and ZN stain(1% H 2 SO 4) • Isolation done on routine media. • Colonies are dry to chalky, yellowish.
� Histopathological examination shows multilobulated with sun ray appearance
TREATMENT • MEDICAL Rx- sulfa drugs like TMP-SMX • SURGICAL Rx- drainage of abscess