ACROMIOCLAVICULAR JOINT Diarthrodial joint between medial facet of
 clavicle.")
ACROMIOCLAVICULAR JOINT Diarthrodial joint between medial facet of acromion and the lateral (distal) clavicle. Width 1 -3 mm younger, it narrows to 0, 5 mm >60 yrs Contains intra-articular disk of variable size. Thin capsule stabilized by ligaments on all sides: AC ligaments control horizontal (anteroposterior ) displacement Superior AC ligament most important

Distal Clavicle Coracoclavicular ligaments – “Suspensory ligaments of the upper extremity” – Two components: Trapezoid Conoid – Stronger than AC ligaments – Provide vertical stability to AC joint

Mechanism of Injury Moderate or high-energy traumatic impacts to the shoulder 1. 2. 3. 4. Fall from height Motor vehicle accident Sports injury Blow to the point of the shoulder 5. Rarely a direct injury to the clavicle

Epidemiology Male > Female 5: 1 <35 yrs 12% Shoulder dislocation involving effect AC joint 41% of collegiate American football players had suffered an AC injury Brett D Owens, 2014 Kaplan LD, Am J Sport Med: 2005

Physical Examination Inspection – Evaluate deformity and/or displacement – Compare to opposite side. Palpation Evaluate pain Look for instability with stress Neurovascular examination Evaluate upper extremity motor and sensation Measure shoulder range-of-motion

Radiographic Evaluation of the Acromioclavicular Joint Proper exposure of the AC joint requires one-third to one-half the x -ray penetration of routine shoulder views Initial Views: – Anteroposterior view – Zanca view (15 degree cephalic tilt) Other views: – Axillary: demonstrates anteriorposterior displacement – Stress views: not generally relevant for treatment decisions – C/T

MRI F. Alyas, 2008

Classification For Acromioclavicular Joint Injuries Initially classified by both Allman and Tossy et al. into three types (I, II, and III). Rockwood later added types IV, V, and VI, so that now six types are recognized. Classified depending on the degree and direction of displacement of the distal clavicle. Allman FL Jr. Fractures and ligamentous injuries of the clavicle and its articulation. JBJS: 1967. Rockwood CA Jr and Young DC. Disorders of the acromioclavicular joint, In Rockwood CA, Matsen FA III: The Shoulder, Philadelphia, WB Saunders, 1990
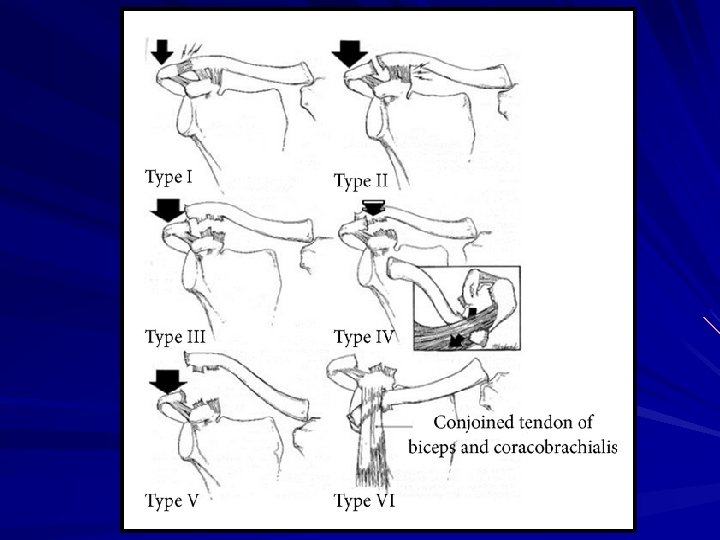

Type III From Nuber GW and Bowen MK, JAAOS, 5: 11, 1997 Sprain of acromioclavicular ligament AC joint intact Coracoclavicular ligaments intact Deltoid and trapezius muscles intact AC joint disrupted < 50% Vertical displacement Sprain of the coracoclavicular ligaments CC ligaments intact Deltoid and trapezius muscles intact AC ligaments and CC ligaments all disrupted AC joint dislocated and the shoulder complex displaced inferiorly CC interspace greater than the normal shoulder(25 -100%) Deltoid and trapezius muscles usually detached from the distal clavicle Type III

Type IV Type VI AC and CC ligaments disrupted AC joint dislocated and clavicle displaced posteriorly into or through the trapezius muscle Deltoid and trapezius muscles detached from the distal clavicle Type IV AC ligaments disrupted CC ligaments disrupted AC joint dislocated and gross disparity between the clavicle and the scapula (100 -300%) Deltoid and trapezius muscles detached from the distal half of clavicle Type VI Type V AC joint dislocated and clavicle displaced inferior to the acromion or the coracoid process AC and CC ligaments disrupted Deltoid and trapezius muscles detached from the distal clavicle

TREATMENT AC JOINT DISLOCATION CONSERVATIVE 32 Methods of Non-operative treatment Urist MR, Am J Surg: 1959 SURGICAL TREATMENT >30 different operative procedures been descrided Smith MJ, Am J Sports Med: 1979

Treatment Options For Types I - II Acromioclavicular Joint Injuries Nonoperative: Ice and protection until pain subsides (7 to 10 days). Return to sports as pain allows (1 -2 weeks) No apparent benefit to the use of specialized braces Type II operative treatment Generally reserved only for the patient with chronic pain. Treatment is resection of the distal clavicle and reconstruction of the coracoclavicular ligaments.

Treatment Options For Type III-VI Acromioclavicular Joint Injuries Type III Injuries: Need for acute surgical treatment remains very controversial. Most surgeons recommend conservative treatment except in the throwing athlete or overhead worker. Repair generally avoided in contact athletes because of the risk of reinjury. Nonoperative treatment Closed reduction and application of a sling and harness to maintain reduction of the clavicle Short-term sling and early range of motion

SURGICAL TREATMENT FOR TYPE III-VI AC JOINT INJURIES 1800 s - 1900 s Procedures included: A/C repairs Coracoclaviculars repairs Combined: A/C repairs & Coracoclaviculars repairs Coracoclavicular Fusion Dynamic muscle tranfers

Treatment Options For Type III-VI Acromioclavicular Joint Injuries Operative treatment – Primary AC joint fixation – Primary CC ligament fixation – Excision of the distal clavicle – Dynamic muscle transfers

L. Galatz, 2001

Intra-articular AC joint fix. 1, 8 mm Kirschner percutaneus
![Intra-articular AC joint fix. Hook plate [Removable] Habernet H, 1993 Simm E, Clin Orthop:](http://slidetodoc.com/presentation_image_h2/399cabec460253baeee4bdbc336820a0/image-20.jpg "Intra-articular AC joint fix. Hook plate [Removable] Habernet H, 1993 Simm E, Clin Orthop:")
Intra-articular AC joint fix. Hook plate [Removable] Habernet H, 1993 Simm E, Clin Orthop: 1995
![Extra-articular Coracoclavicular Repairs Bosworth screw [1941] Tsou, 1989 Cannulated [Removable 8 W Post-Op]](http://slidetodoc.com/presentation_image_h2/399cabec460253baeee4bdbc336820a0/image-21.jpg "Extra-articular Coracoclavicular Repairs Bosworth screw [1941] Tsou, 1989 Cannulated [Removable 8 W Post-Op]")
Extra-articular Coracoclavicular Repairs Bosworth screw [1941] Tsou, 1989 Cannulated [Removable 8 W Post-Op]

Extra-articular Coracoclavicular Repairs Cerclage techiques Kiefer H, 1986 Hessman M, 1995

Ligament Reconstruction Weaver-Dunn, JBJS Am: 1972


32 yrs ♂ 6 mon Post-Op


4 mon Post-Op

Arthroscopic Reconstruction of C/C Ligament Boileau P, 2008 Spotili M, 2015

Complications Wound infection-Osteomylitis ~ 1% Fracture through the drill hole Failure Int. Fix , Migration Failure of Soft tissue Repair Complications Related to Nonabsorbable tape or suture Acromioclavicular arthritis Decrease shoulder range of motion/upper extremity strength

- Slides: 32