Acne Vulgaris Mandy Jones Pharm D PAC BCPS

Acne Vulgaris Mandy Jones, Pharm. D, PA-C, BCPS Spring 2014

Clinical Types • Noninflammatory – Open & closed comedones, papules, few pustules • Inflammatory – Erythematous papules, pustules, possible scarring Mild→ Moderate→ Severe

Post-inflammatory hyperpigmentation

Pharmacologic Treatment: Patient Considerations • • • Clinical type of acne (comedonal, inflammatory, nodular, etc) Severity of acne Skin type (Dry, Oily) Presence of scarring or post-inflammatory hyperpigmentation Menstrual history and signs of hyperandrogenism in women History of prior successful and failed treatments Allergies Medication adherence patterns History of acne promoting medications Pyschological impact of acne on the patient Patient preference and cost concerns

General Self Care Measures and Non. Pharmacologic Treatment • Covered in OTC and listed in notes

General Treatment Pearls • 8 weeks for microcomedo to mature • Mild-Moderate→ Topical • Moderate-Severe→ Systemic • Topical therapy: – Consider skin type and dosage form

TOPICAL THERAPY
 Benzoyl Peroxide (BPO) Azelaic acid 20%")
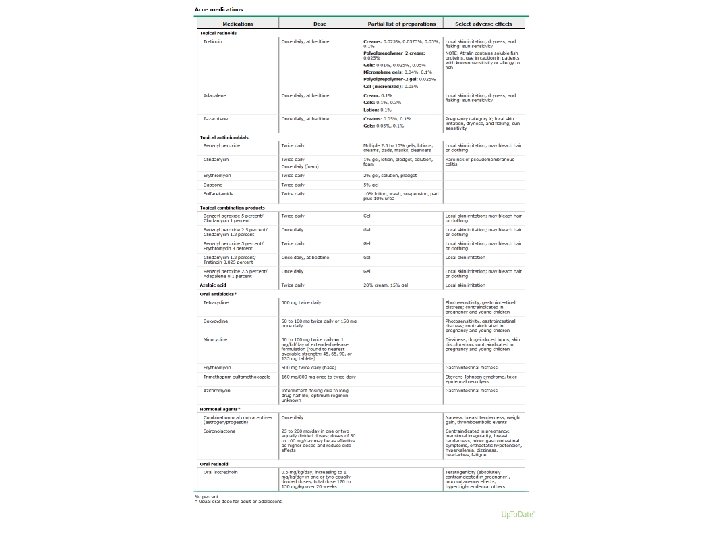
TOPICAL THERAPY • • • Topical Retinoids (TRs) Benzoyl Peroxide (BPO) Azelaic acid 20% Cream Dapsone 5% Gel Salicylic acid Topical antibiotics
 • adapalene (Differin®")
Topical Retinoids • tretinoin (Atralin™; Avita®; Renova®; Retin-A® Micro; Retin-A®; Tretin-X™) • adapalene (Differin® XP; Differin®) • tazarotene (Avage™; Tazorac®) • MOA: Vitamin A derivatives----directly targets genes implicated in acne pathogenesis – Decreases comedogenesis by: binding to Retinoic acid receptors (RARs) and Retinoid X Receptors inside keratinocytes→ activation of regulatory DNA sequencing called retinoid hormone response elements→ transcription of target genes responsible for keratinization→ normalization of follicular keratinization and decreases cohesiveness of keratinocytes – Decreases inflammation : Retinoid receptor complexes compete for AP-1 (a key transcription factor in inflammation) and down regulates expression of toll-like receptor (TLR-2), which is responsible for the inflammatory mechanism in acne

Topical Retinoids Some specifics……. .

Fact or Fiction? It doesn’t matter which TR to recommend…. they’re all the same

Eh---it depends on the parameter • Efficacy: – ? ? Tazarotene >> Tretinoin & Adapalene? ? – Head-to-head trials do not definitely support one TR over another in terms of efficacy • Safety: – In order of INCREASING skin irritation: • Adapalene << Tretinoin << Tazarotene • And other nuances: – Atralin®- made with soluble fish proteins – avoid in fish allergy – Tretinoin and tazarotene are deactivated by sunlight and oxidized by BPO (can’t use together at same time) – Adapalene is stable in sunlight & in presence of BPO …. . Epiduo® is combo product of adapalene and BPO
 Benzoyl Peroxide (BPO) Azelaic acid 20%")
TOPICAL THERAPY • • • Topical Retinoids (TRs) Benzoyl Peroxide (BPO) Azelaic acid 20% Cream Dapsone 5% Gel Salicylic acid Topical antibiotics

Systemic Therapy • For moderate to severe acne – Oral Abx • Minocycline, doxycycline (1 st line) • Erythromycin, clindamycin (2 nd line) • Sulfamethoxazole-trimethoprin (rarely) – Isotretinoin

Oral Abx • Some specifics……………. .

Fact or Fiction? Using antibiotics for acne increases the risk of being infected with resistant bacteria.

Somewhat true…. but not terrible • Oral AND topical→ resistant P. acnes & CNS & colonization with Strep. pyogenes • Increased risk of strep throat and impetigo…. but treatment is no different • Resistant p. acnes more difficult to treat

Oral Abx: Recommendations • Limit use to 12 -18 weeks • Never use as monotherapy…. . combine with BPO to prevent resistance, or with TR to decrease duration of Abx use • Once lesions clear, d/c Abx and use TR +/- BPO for maintenance • Rec. Doxy over Mino – Mino higher cost, no definitive studies indicating Mino superiority, Mino assoc. with more concerning ADRs – If no response with Doxy, can switch to Mino (pts may respond to one tetracycline but not the other)

But what about the Doxy shortage? • If you only have one salt form on your shelves, suggest using what you have – Hyclate and monohydrate equally effective, but hyclate associated with more GI upset • Use TR plus BPO or topical Abx instead • If oral Abx is needed, suggest – Minocycline $$ or macrolide (erythro or clinda)

Isotretinoin • Reserved for severe recalcitrant acne, nodulocystic acne, or significant physical or psychological scarring • Only acne agent that works on all 4 mechanisms of acne pathogenesis • Exact MOA not known, but it: – Shrinks sebaceous glands, decreases sebum secretion thus reducing p. acnes growth – Fosters keratinocyte differentiation and normalizes desquamation

Isotretinoin, i. PLEDGE, and other specifics

Acne Vulgaris Otherapies Special populations/situations • Oral contraceptives • Spironolactone • Oral corticosteroids • Post-inflammatory hyperpigmentation • Pregnancy • Pediatrics and adolescents

Oral Contraceptives TYPO in notes • Preference/Pearls----should say: – AVOID 2 nd generation progestins in patients with acne (i. e. levonorgestrel; norgestrel) – 2 nd generation progestions: • High affinity for androgen receptor→ most androgenic • 1 st, 3 rd, 4 th generation OK to use
- Slides: 24