Acne and Acne related disorders Disorders of sebaceous

Acne and Acne related disorders Disorders of sebaceous glands and Rosacea

ACNE Is a chronic inflammatory disorder of the pilosebaceous unit of certain body area (Face, Trunk ).

Incidence: Acne affects all skin types the male and female ratio is virtually the same but tends to be more severe in males. 85% affects the age group 12 – 24 years 8% affects the age group 25 – 34 years 3% affects the age group 35 – 44 years
. 2. Occupation (Environmental, Mechanical) e. g. exposure")
Etiology: Genetic Aspect, (Acne runs in family). 2. Occupation (Environmental, Mechanical) e. g. exposure to mineral oil. 3. Drugs Oral and topical Hydrocortison (Steroid acne), Lithium, contraceptives 4. Endocrine Factors. 1.

Pathogenesis: 1. Follicular Hyperkeratosis

2. Abnormal production of abnormal sebum is believed to be the response of sebaceous glands to DHEA 3. Colonization of the affected unit with bacteria Propionibacterium acne
 to release irritant free fatty")
Propionobacterium acne lipases act on sebaceous fatty acid (Triglycrides) to release irritant free fatty acid and low-molecular- weight peptide an extra cellular factor that penetrate the follicular wall and stimulate Polymorphs and Lymphocytes initiating inflammation
 1. n Comedones (Open")
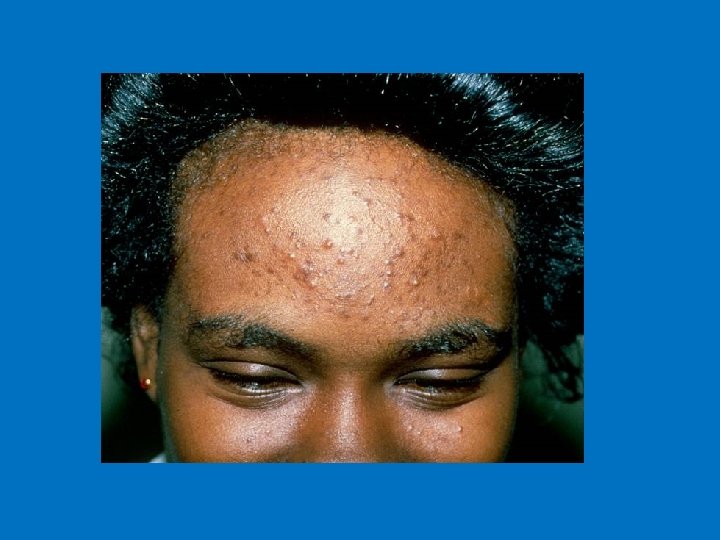
Clinical features: Acne Vulgaris: Papules: (Less than 0. 5 cm) 1. n Comedones (Open “Blackheads” or closed “Whiteheads”)
 Open Comedones")
Open Comedones (Blackheads) Open Comedones
 Closed Comedones")
Closed Comedones (Whitehead) Closed Comedones

n Inflammatory papules

n Pustules : Pustules

n Nodule

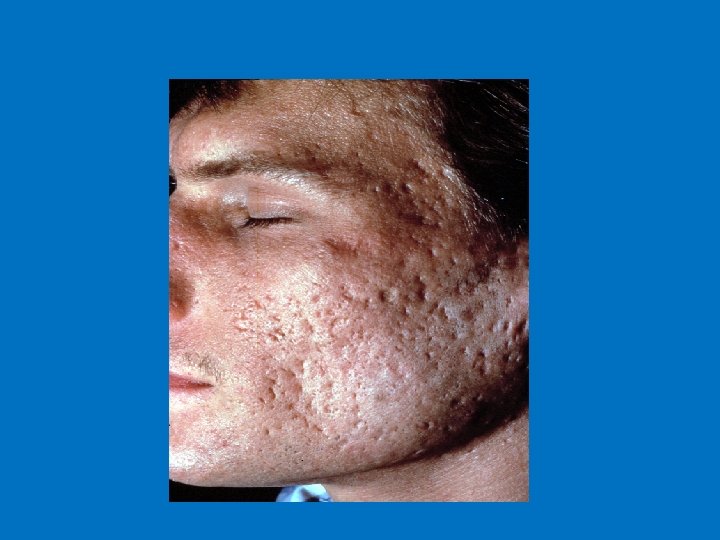
n Cystic acne: the cysts are usually large

Numerous pustules, papules, § open and closed comedones with some scarring Open comedo Closed comedo Pustule Inflamed papule Scarring 15

3. Neonatal Acne and Infantile Acne n Neonatal acne: cause unknown but some believed is due to passing of Transplacental androgen other suggest the role of Mlalassezia furfur and. affect 1 in 5 mainly inflammatory comedones on nose and cheeks affect new born between the 1 st and 6 th week of age


n Infantile Acne: affect males more than females, usually between 3 and 6 months of age, and tend to be severer than the neonatal one and believed to be due to Endogenic androgen from the infant’s gonads.

, very severe")
4. Acne Fulminans Affect young patients (13 – 17 years of age), very severe with ulceration and pus discharge, associated symptoms include (fever, malaise, myalgia, arthritis and bone pain) laboratory investigation shows ESR Can be induced by starting the patient on high dose of isotretinion (Roaccutane).


5. Acne Conglobata Very severe Acne, Nodulocystic form with abscess formation.

Occupational I Environmental Chloracne rare forms of acne affect patients exposed to Halogenated Hydrocarbons or who ingested Chlorinated Phenols (Dioxin) n Oil Folliculitis n

Occupational II mechanical acne Folicullitis Nuchae or so called Acne Keloidalis n Pseudofollicultis barbae n n Acne excoriee as part of Psychodermatosis


TREATMENT 1. Anti comedonal 2. Anti inflammatory 3. Anti microbial

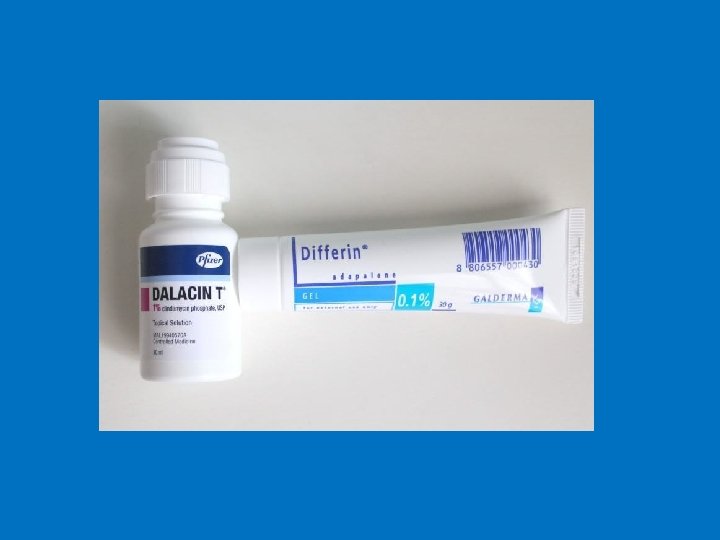
Topical Keratolytic n n n Retinoid ( Retinoic acid 0. 025, 0. 05, 0. 1%) Adapalene (Differin 0. 1%) Salicylic acid Benzoyl peroxide (peeling agent and antimicrobial) Azelaic Acid
 n Erythromycin n")
Topical Antibiotic Topical clindamycin (Dalacin T) n Erythromycin n
 Tetracycline Doxycycline Minocycline")
Systemic therapy n 1. 2. 3. 4. Antibiotic (Macrolides and Tetracylines) Tetracycline Doxycycline Minocycline (blue grey discoloration and drug induced LE) Azithromycin
: 0. 5 – 1 mg/kg")
Systemic Retinoids : § § § Isotretinoin caps (Roaccutane): 0. 5 – 1 mg/kg The most effective drug for acne. Indicated for severe forms (nodulocystic and fulminant). Relapse is minimal with cumulative dose of 120 – 150 mg/kg. Side effects include: cheilitis, dryness, photosensitivity, decreased night vision, keratitis, benign intracranial hypertension photosensitivity, hypertriglyceridemia, hypercholesterolemia, elevated liver enzymes, depression (controversial), skeletal hyperostosis, myalgias.

Systemic Retinoids : Teratogenicity : Retinoid - induced embryopathy. Pregnancy category X. § Pregnancy must be prevented during treatment and for at least 1 month after discontinuing the drug. §
 Spironolactone (Potassium sparing agent) and Metformin")
Other forms of therapy n Hormonal therapy (Anti-androgen) Spironolactone (Potassium sparing agent) and Metformin as (Hypogylcemic agent) in treatment of PCOS (Polycystic Ovary Syndrome) have good results on acne

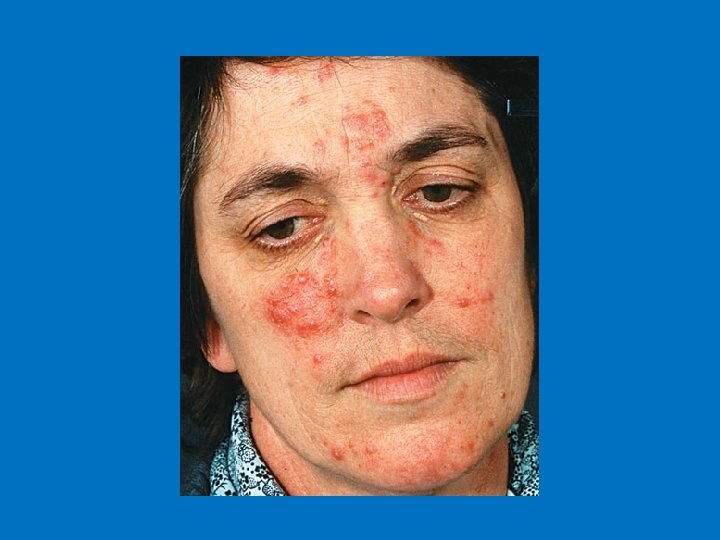
Rosacea Erythema of the central face that has persisted for months or more. - Primary features: flushing, papules pustules and telangiectases. - Secondary features: burning, stinging, edema, plaques, dry appearance, peripheral flushing and ocular manifestations. -


Epidemiology Common in caucasian population n Fair skinned individuals n women>men n Onset typically begins after age 30 n

Etiology and pathogenesis n Vascular reactivity: n Rosacea is induced by chronic repeated triggers of flushing exposure, they include: n 1) Hot or cold temperature 2) Hot drinks 3) Spicy foods 4) Alcohol 5) Certain cosmetics 6) Medications n n n 7) Sunlight 8) Emotional disteress 9 ) Topical irritants

Etiology and pathogenesis n Dermal matrix degeneration and endothelial damage Inherent problems with vessels permeability n Delayed clearance of inflammatory mediators and waste products n Photodamaged connective tissue (solar elastosis is a common background on which rosacea histologic features are superimposed n Demodex folliculorum (mite). n
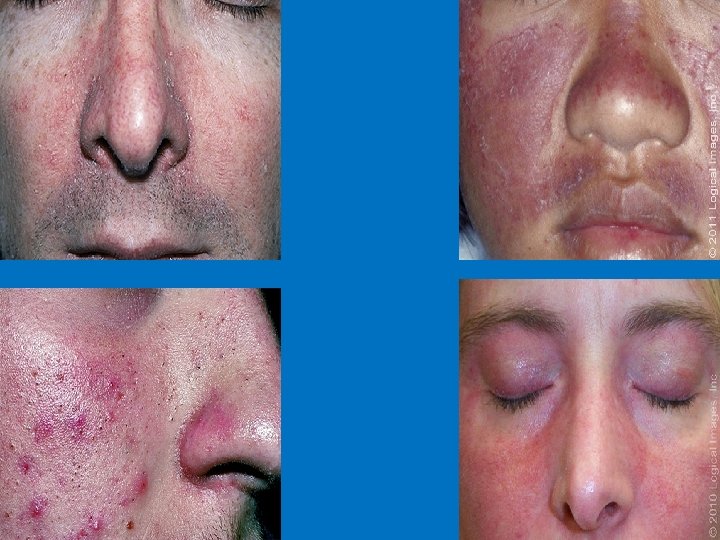
 Erythematotelangiectatic : persistent erythema and telangiectasias on the central face. 2)")
Sub-type classification 1) Erythematotelangiectatic : persistent erythema and telangiectasias on the central face. 2) Papulopustular: papules and pustules predominate on convex areas on a background of persistent erythema 3) Phymatous: follicular orifices, thickened skin and nodularity Most often affect the nose (rhinophyma) Almost exclusively in men 4) Ocular: Blepharitis is the most common feature (mebomian gland dysfunction) Conjuctivitis, iritis, scleritis, keratitis

Erythematotelangiectatic Rosacea

Papulopustular Rosacea


Rhinophyma
is required, Medications that induce flushing include :")
Managment Full and detailed history (including medications)is required, Medications that induce flushing include : all vasodilators, calcium channel blockers , systemic steroids and cyclosporine. Diagnosis is made clinically

Differential diagnosis include: Seborrheic dermatitis Steroid folliculitis/Perioral Dermatitis Acne vulgaris Erythromelanosis faciei and keratosis pilaris rubra Lupus erythematosus

Treatment Sunscreens n Avoidance of aggravating factors. n Topical medications include: n n n Metronidazole Benzoyl peroxide Tretinoin Erythromycin and Clindamycin Ivermectin cream

Oral medications include: n Tetracyclines are the most commonly prescribed oral medications for the treatment of rosacea. n They act by their anti-inflammatory effects n Isotretinoin

Laser and light therapy Laser and Intense Pulsed light IPL is useful in treating persistent erythema and telangiectasias Pulsed dye laser (585 or 595 nm)

Treatment of Phymatous Rosacea § § § Early to moderate Phymatous changes could be treated with Isotretinoin. Advanced phyma is treated with surgery or surgery followed by isotretinoin. Scalpel excision Electrosurgery Laser CO 2 ablation.

Thank You
- Slides: 54