Acid Base Physiology DEFINITIONS Acid any chemical substance

Acid – Base Physiology
. Base")
DEFINITIONS: Acid = any chemical substance that can donate a hydrogen ion (H+). Base = any CHEMICAL substance that can accept a hydrogen ion. p. H = minus log of the power of 10 of the hydrogen ion concentration = -log 10 [H+] If the concentration of H cations is 10 -7 M, the p. H is 7. The higher the p. H number, the lower the number of H+, and the less acidic. 10 -3 M would have a p. H of 3, and be very acidic, while 10 -11 M would have a p. H of 11, and be very alkaline. Thus, a decrease of p. H from 6 to 5 represents a 10 fold increase in the number of H+ ions.

In the body, the number of hydrogen ions in the body must be closely regulated at low levels. For instance, Na in extracellular fluid is 142 m. Eq/L, but the H+ concentration is 0. 00004 m. Eq/L. (3. 5 million X difference) A hydrogen ion (H+) is a single free proton released from a hydrogen atom. Any molecule which can release H+ is an acid. Bases are often alkalis, formed by the combination of alkaline metals (Na, K, Li) with a strong basic ion (OH-) The OH- in the alkali molecule reacts quickly with H+ to remove it from solution. The term “alkalosis” refers to the excessive removal of H+ from body fluids, and conversely “acidosis” refers to the excess addition of H+

Strong Acids quickly dissociate to release H+, while weak acids do not readily release their H+. A strong base is a base that quickly binds H+ to remove it from solution, while a weak base does not bind H+ very strongly (can dissociate easier). The normal p. H of arterial blood is 7. 4, while interstitial fluid and venous blood are 7. 35 due to the increase in CO 2 released due to cellular metabolism in exchange for O 2. Intracellular p. H is about slightly lower than 7. 4 (67. 4) due to acid formation in metabolism. The ranges for existence of a human are between p. H 6. 8 and 8. 0.

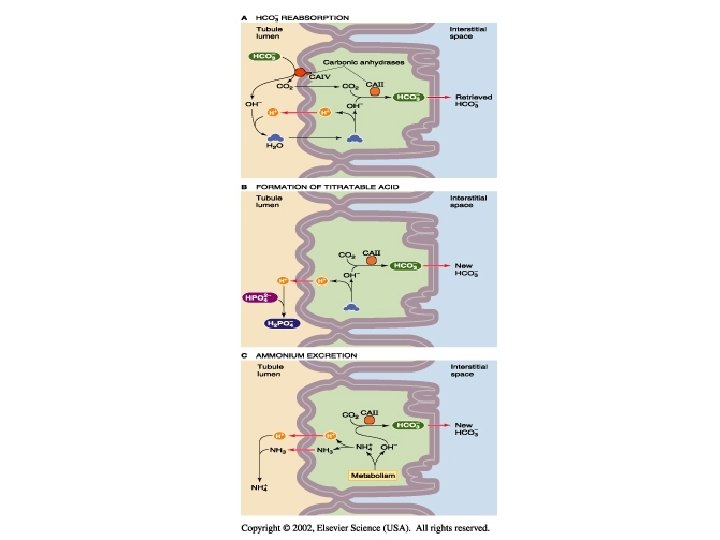
The p. H of the body is controlled by three systems: 1. The chemical acid-base buffering by the body fluids that immediately combine with acids or base to prevent excessive changes in p. H. 2. The respiratory center which regulates the removal of volatile CO 2 as a gas in the expired air from the plasma and therefore also regulates bicarbonate (HCO 3 -) from the body fluids via the pulmonary circulation. This response occurs in minutes. 3. The kidneys which can excrete either acid or alkaline urine, thereby adjusting the p. H of the blood. This response takes place over hours or even days, but represent a more powerful regulatory system.

Phosphate buffering: While the phosphate buffering system is not important in buffering the extracellular fluid, it is very important in buffering intracellular p. H and also in buffering renal tubular fluid. The system is composed of H 2 PO 4 - and HPO 4 -2 For example, addition of a strong acid like HCL leads to HCl + Na 2 HPO 4 Na. H 2 PO 4 + Na. Cl Replacing the strong acid with a weak acid minimizing the change in p. H. The p. K of this buffer system is 6. 8, so it operates near its maximum buffering power at normal p. H.

Other buffering systems: There is slight diffusion of H+ and HCO 3 into cells, but CO 2 can diffuse rapidly through cell membranes. Proteins are important buffers especially within cells, and accounts for 60 -70% of the total intracellular buffering capacity. Hemoglobin in RBC’s is a particularly important protein buffer.

Since most biologic compounds are weak acids or bases, even small changes in the p. H (availabiltiuy of the hydrogen ion) may result in them donating or accepting H+, thus changing their net electrical charge, valance , and possibly the molecular configuration and even its biologic activity. ie; a base accepts a H+; R-NH 2 + H+ R-NH 3+ or, an acid donates a H+; R-COOH R-COO- + H+

The “normal” p. H of the body is 7. 4 (or 4 x 10 -8 M H+) Molecules that are sensitive to p. H include; Enzymes, receptors, ion channels, pumps, membrane transporters, proteins. A molecules p. H optimum may exist at normal p. H (7. 4) and its biologic activity be changed when the p. H varies, or it may exist at a p. H away from normal and be activated as p. H shifts from normal p. H toward this optimum. A variety of systems regulate and buffer p. H in the body.

Buffer: any substance which reversibly consumes or releases H+. Buffers minimize or attenuate changes in p. H by consuming or adding H+ in such a way to minimize discrete changes. Valence does not matter, ie for buffer “B” Protonated form in equilibrium with deporotonated form Weak acid HB (n+1) Weak base = B (n) + H (+) The buffers distribute themselves via their dissociation constant (K) defined as the ratio [B(n)] [H+] = K [HB(n=1)]

If we add a strong acid to a buffer, the buffer consumes most of the H and thereby buffers the p. H , minimizing the H+ in solution. HCl + B H+ + Cl- + B(n) HB (n+1) + Cl- The same happens adding a strong base (Na. OH) Na. OH + B Na+ + OH- + B (n+1) Na++ B(n) + H 2 O Buffering Power: Moles of a strong base (Na. OH) that must be added to a liter of solution to increase p. H by 1 p. H unit.
 and HCO 3 -")
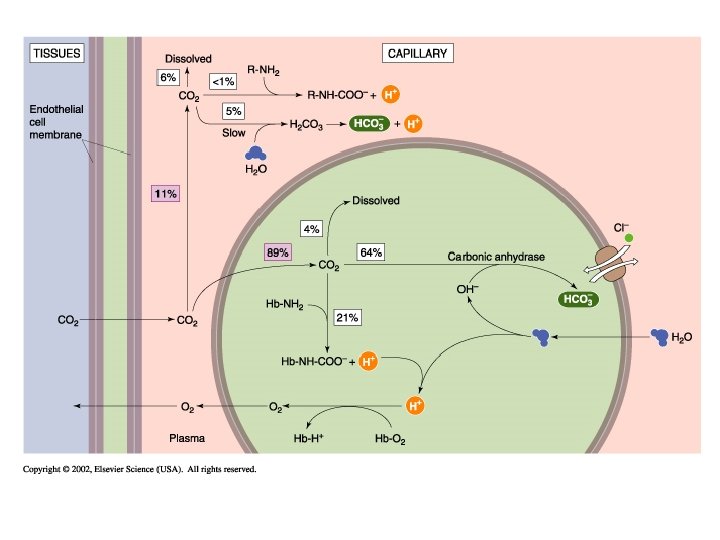
Most important physiological buffer pair is CO 2 (carbon dioxide) and HCO 3 - (bicarbonate). Since the lung can expire volatile CO 2, it can regulate and stablize the balance of CO 2. If CO 2 is in solution, it can dissociate to carbonic acid (a slow reaction) CO 2 + H 2 O H 2 CO 3 Formed carbonic acid can quickly dissociate to hydrogen ions and bicarbonate: H 2 CO 3 H+ + HCO 3 Note that the formation of H+ will decrease p. H. The net reaction is CO 2 + H 2 O H+ + HCO 3 -

CO 2 + H 2 O H+ + HCO 3 For this reaction, the dissociation constant K will be K = [H+] + [HCO 3 -] [CO 2] in log form this equation becomes p. H = p. K + log [HCO 3 -] [CO 2] The concentration of CO 2 is governed by its solubility in ionic solution, and in plasma its partial pressure (40 mm. Hg) which predicts a normal p. H of 7. 4 (see page 636). Note that the equilibrium is driven by the ability to pull CO 2 out of solution and drive the reaction away from H+

The buffering power of a weak acid-base pair depends upon: 1. The total concentration of the buffer pair (the buffering capacity (B) is proportional to the total concentration (TB)) 2. The p. H of the solution 3. Whether the system is “open” or “closed. ” (in this case, the ability of CO 2 to be released out of solution in the lung, means it is an open system. Otherwise, it would be a closed system).
 is fixed")
In a closed system, the total concentration of the buffer pair (TB) is fixed and the distribution is only the movement between associated and dissociated forms of the buffer pair, and the maximum buffering capacity is at a given p. H defined by the dissociation of the buffer and H+. BH(n+1) B + H+ An example of a closed system buffer pair is the titeratable charge on a protein in plasma, including hemoglobin in RBC’s. In plasma, there actually many different buffering systems that all contribute to the buffering capacity of the system, so that

Buffering capacity of a single closed buffer pair and the net effect of the combination of a number of buffer systems on the buffering capacity of the net solution. Note on the right (B) that the 9 different buffers each have a different maximum buffering capacity at different p. H’s yielding range of capacity to buffer changes in p. H.
 in which the total CO")
In contrast, in an OPEN buffer system (CO 2) in which the total CO 2 can vary widely. Thus, the addition of H+ can drive the reaction to the left to the formation of CO 2 which is then lost from the reaction, pulling more H+ out of solution and buffering p. H CO 2 + H 2 O H+ + HCO 3 -

If the p. H rises above 7. 4, the buffering power of the open system increases exponentially because of the increasing partial pressure of CO 2 (p. CO 2) facillitating the removal of it from solution and expiring it into the environment.

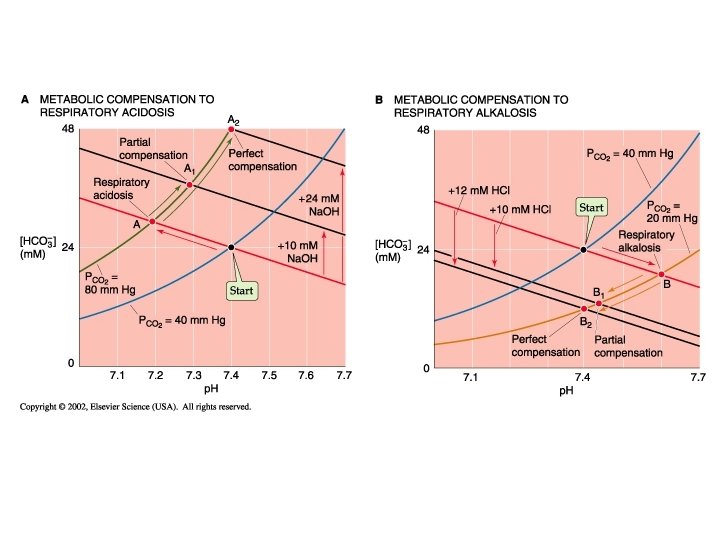
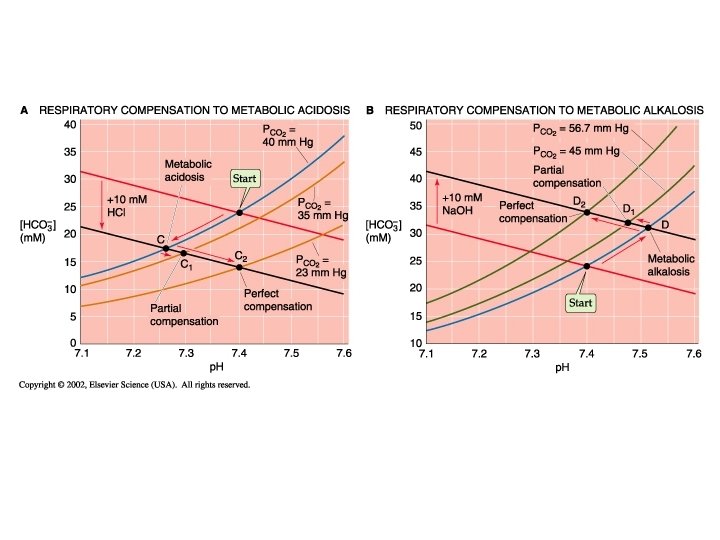
Acid-base Distrubances in the p. H The abnormal loss of acid (as in vomiting gastric HCl) or addition of a weak base can lead to the condition of Metabolic Alkalosis: increasing p. H above 7. 4. In contrast, abnormal removal of HCO 3 - or another alkali or addition of acids other than CO 2 or H 2 CO 3 (as can happen in renal failure) can lead to Metabolic Acidosis: decreasing p. H below 7. 4. Since the p. H of a CO 2/HCO 3 - solution depends upon the ratio of these tow buffer pairs, and because the lung control CO 2 but the kidney controls HCO 3, the overall description of their interaction might be described as p. H = k + KIDNEY / LUNG (Not a real reaction equation, but rather a descriptive relationship between the regulating components of ph in the body)

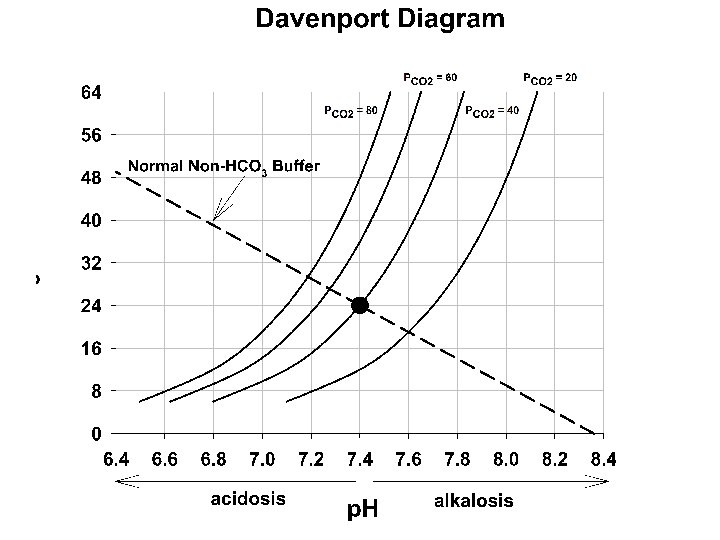
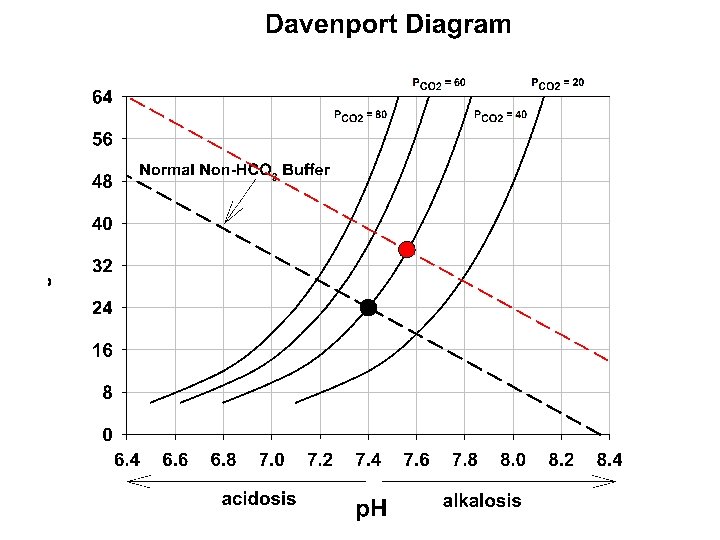
In biological systems, the total buffering of p. H and the effects of acid-base distrubances is due to a complex interaction of many buffering systems, open and closed, with differing buffering capacities. all HB (n+1) H+ + all B (n) Predictions of the effects of these disturbances is done using a “Davenport Diagram. ” Combining with CO 2/HCO 3 such that CO 2 + H 2 O HCO 3 - + H+ + B(n) HB(n+1) Now, the final p. H depends on two buffering pathways that affect the [H+] with two different equilbria equations.
 represents the")
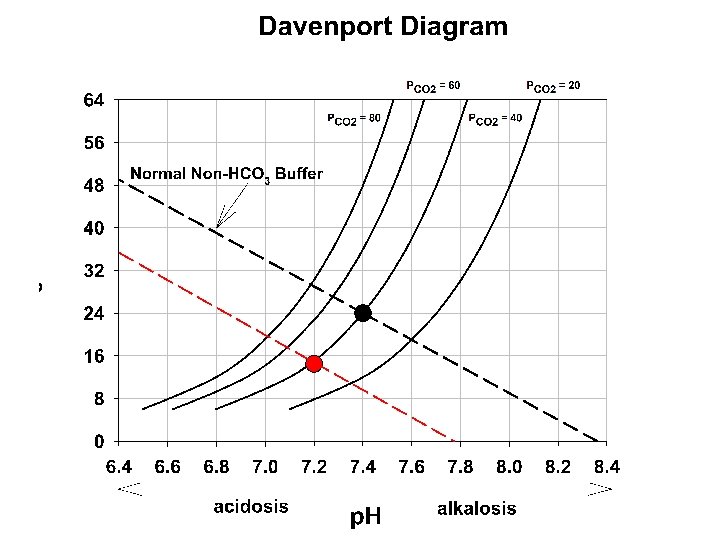
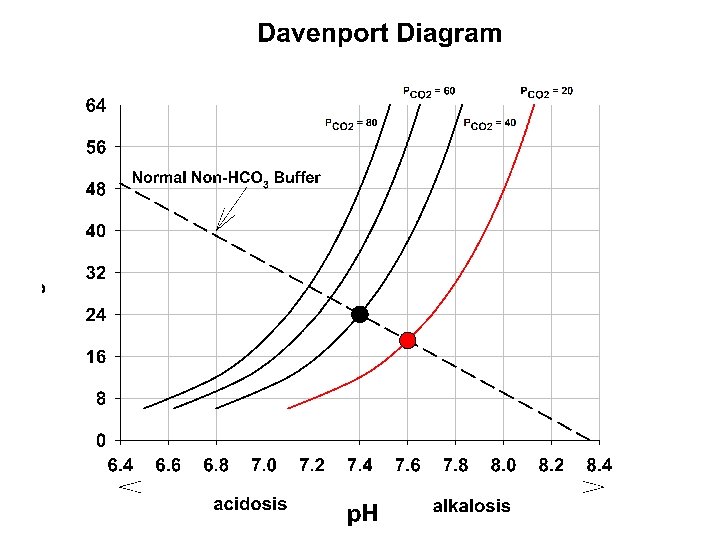
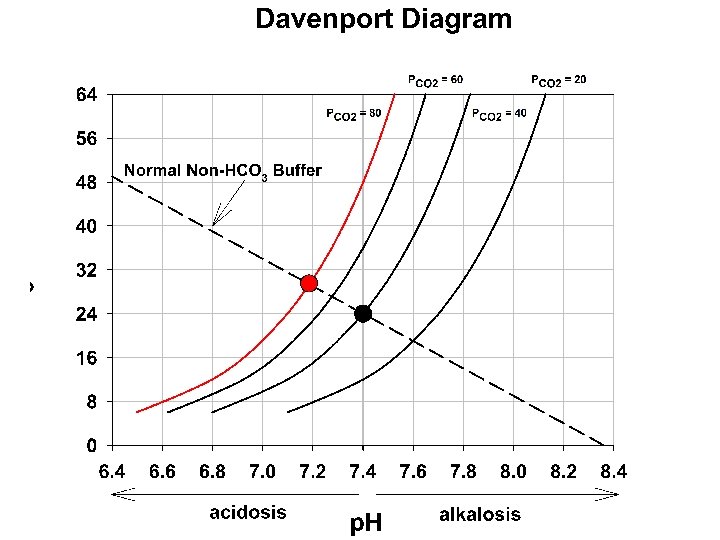
Davenport diagram: the blue curve is the p. CO 2 isobar (isopleth) represents the relationship between p. H and HCO 3 at a p. CO 2 of 40 mm. Hg. Orange line is in respiratory alkalosis (p. CO 2 = 20). The green line is respiratory acidosis. These occur due to the changing p. CO 2 via altered respiratory functon

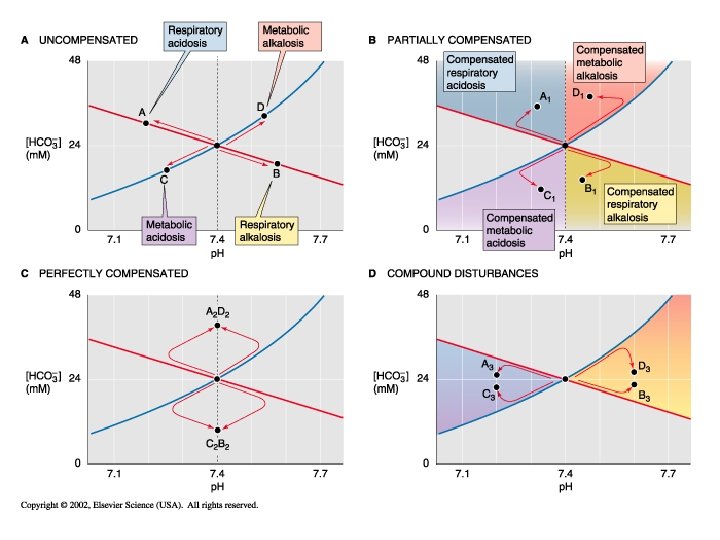
In the right panel. The red lines represent the influence of non CO 2/HCO 3 buffering systems. Point A 1 would occur if these did not exist. Point A if these exist at 25 m. M/p. H (normal for whole blood) , and A 2 if these buffering systems were infinite. Note that this red line to point A is shown in panel A and describes the changing buffer capacity of the non CO 2/HCO 3 systems during each respiratory disturbance.

stop • I’ve had enough
- Slides: 33