Acid Base Electrolytes Balance and Alterations Fluid Compartments

Acid, Base, Electrolytes Balance and Alterations

Fluid Compartments

Fluid Compartments: 20 – 40 – 60 Rule

Fluid Movement

Water and Electrolyte Balance l l Input = output Hormones • • • Na+ / K+ • • • Renin Aldosterone ANP Reproductive Hormones GCC Ca++ / Mg++ • • Calcitonin PTH H 2 O • ADH l Anions follows passively • • • Cl. HCO 3 PO 4=

Water l l l Intake Loss • • Normal Abnormal Osmosis Hormonal control Capillary Dynamics • • CHP COP IHP IOP

Osmosis

Capillary Dynamics

Capillary Pressures

Fluid Shift to third space l l Edema Effusion Transudate • • Low cell Low protein Exudate • • Types: Nonseptic, Septic Contents • • High cell High protein

Edema l l l Causes • • Obstruction Overload Inflammation hypoalbuminemia • • Angioedema Lymphedema • Localized • Generalized Vessels Types • • • Pitting Weeping Dependent

Pulmonary Edema

Pleural Effusion

Terminology l l l Isotonic • • Hypovolemia Hypertonic • Hyperosmolar Hypotonic • Hypo-osmolar

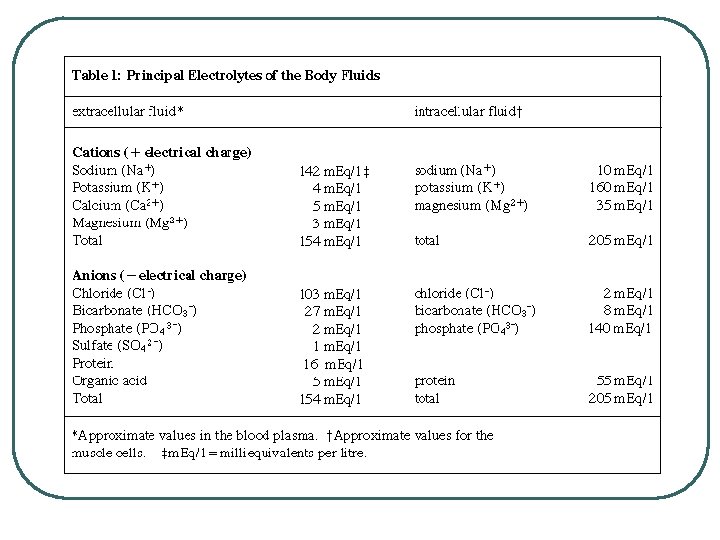
Functions of electrolytes

Electrolyte Fluid Composition

Hormones that regulate Electrolytes l l l Aldosterone ANP PTH Cacitriol Calcitonin

Cations l l l + charge Location Function Hormonal Controls Alterations • • Hypo. Hyper-
 Increased")
Hyponatremia l l < 135 m. Eq/L Etiology • • Decreased Na+ (diet) Increased H 20 Diuretics Hiridosis Addison’s Disease DM Diarrhea CRF l Clinical Signs • • • H 20 shift to ICF Cells swell CNS sensitive • Muscle weakness • V/D • Lethargy • Confusion • Seizures

Hyponatremia

Hypernatremia l l > 147 m. Eq/l Etiology • • Excessive intake Hyperaldosteronism Drowning (salt water) H 20 loss • • • DI Renal Fever / Sweat Burns Diarrhea l Clinical Signs • • • Osmotic shrinkage CNS sensitive • • • Lethargy Irritability Hemorrhage Seizures Coma Muscle weakness

Hypokalemia l l < 3. 5 m. Eq/l Etiology • • Decreased intake ANS V/D Diuretic Sweating Digitalis Insulin excess l Clinical Signs • Decreased RMP • Heart dysrhythmia • • Bradycardia AV blocks PVCs • Sphincter weakness Delayed cardiac repolarization • ST segment depression • T decreased/inverted

Hyperkalemia l l > 5. 5 m. Eq/l Etiology • • Increased intake Insulin deficiency Hemolysis Hypoxia CRF Diuretics Burns Extensive surgeries l Clinical Signs • • Inactivate Na+ channels • Muscle weakness • Muscle paralysis • paralysis Cardiac dysrhythmia • Peaked T wave • Widened QRS

Hypocalcemia l l < 8. 5 mg/d. L Etiology • • • Nutritional deficiency Osteoblastic metastasis PTH deficiency Hyperphosphatemia Increased protein binding Chelation therapy l Clinical Signs • NMJ irritability • Cardiac Dysrhythmia • Muscle Spasm • Dyspnea • Seizures • Colic • Tetany

Hypercalcemia l l > 10. 5 mg/d. L Etiology • • Cancer Hyperparathyroidism Bone remodeling Increased reanal filtering l Clinical Signs • NMJ decreased • • Bone loss Urolithiasis • Fatigue • Lethargy • Weakness • Cardiac dysrhythmia

Hypomagnesemia l l l < 1. 5 m. Eq/l Seen with hypokalemia and hypocalcemia Etiology • • • Decreased dietary intake GI loss • • • Malabsorption Maldigestion Diarrhea CRF l Clinical Signs • • • Decreased threshold • • • Tetany Vertigo Nystagmus Muscle spasms • • hyperreflexia Seizures Cardiac Dysrhythmia
")
Hypermagnesemia l l > 2. 5 m. Eq/l Etiology • • Excess intake (antacids) Decreased renal excretion • CRF • Adrenal insufficiency l Clinical Signs • • Increased threshold for depolarization • Muscle weakness • Decreased reflexes • Hypotension Decrease Na+ current • Cardiac dysrhythmia • Bradycardia

Anions l l l Chloride ECF Alterations • • Hypochloremia • • < 95 m. Eq/L Accompanies hyponatremia Severe vomiting Diuretics Hyperchloremia • • > 103 m. Eq/L Accompanies hypernatremia l l l Phosphate ICF, stored in bones Alterations • • Hypophosphatemia • • • < 2. 7 mg/d. L Antacid use Prolonged decrease cam cause Rickets/’Osteomalacia Hyperphosphatemia • • > 4. 5 mg/d. L Renal failure Overuse of laxatives Hypoxia

Acid Base Terms l Define • • p. H Acid • Base • • Salt Buffer • Strong • Weak • Volatile : CO 2 from CH 20 and Fat Metabolism • Nonvolatile: H 2 SO 4, H 2 PO 4 from protein metabolism • Strong • Weak

Acid Sources
![p. H l l l Define • • p. H = log (1/[H+]) p.](http://slidetodoc.com/presentation_image_h2/7188db4cb3db3199444f8573d484756b/image-33.jpg "p. H l l l Define • • p. H = log (1/[H+]) p.")
p. H l l l Define • • p. H = log (1/[H+]) p. H = -log [H 3 O+] • H 2 O + H 2 O H 3 O+ + OH- Water Dissociation Scale Blood values • • Venous Arterial • • Acidemia Alkalemia Abnormal Values

p. H formula and scale

Acid Base Chart

p. H of Solutions

Acid Base Regulation for Balance l l Systems • • • Chemical Buffer Systems Respiratory System Renal • • • Seconds to Minutes to Hours to Days / Weeks • • • + / - 0. 1 changes result in respiratory rate changes + / - 0. 2 to 0. 3 changes result in CV and Nervous changes + / - 0. 4 to 0. 5 changes result in death Time Strength Problems (reference 7. 4 as normal average):

Chemical Buffer Systems l l Define 3 types • Name of System • Buffer formula or name of chemical • Location • Effectiveness [p. Ka buffer = p. H location] • Why important

p. H changes with/without buffers

Bicarbonate Chemical Buffer l l H 2 CO 3, HCO 3 Plasma buffer p. K = 6. 1 Important: • Can measure components • Can adjust concentration / ratio of components • Recalculate p. H of buffer system in ECF using Henderson-Hasselbach • • p. CO 2 = 40 mm. Hg HCO 3 - = 24 m. M • • HCO 3 - @ kidneys CO 2 @ lungs • p. H = 6. 1 + log(24 / 0. 03 x 40) • p. H = 6. 1 + log (20/1) • p. H = 7. 4

Bicarbonate Buffer System

Phosphate Chemical Buffer l l H 2 PO 4 -, HPO 4= ICF, Urine p. K = 6. 8 Important • Intracellular buffer • ICF p. H = ~ 6. 5 – 6. 8 • Renal Tubular Fluids • Urine p. H ranges 6. 0 – 7. 0

Protein Chemical Buffer l l Proteins • • • With Histadine: AA contain imidazole ring, p. Ka = 7. 0 R-COOH R-COO- + H+ R-NH 2 R-NH 3+ ICF (hemoglobin), ECF p. K = 7. 4 Important • • Most numerous chemicals Most powerful chemical buffer

Proteins in acid base

Hemoglobin

CO 2 transport and RBC buffer

Respiratory for A/B Balance l l l Occurs in minutes CO 2 only Rate changes

Respiratory Controls for Acid /Base balance l l Volatile Acid: CO 2 p. H changes in CSF Respiratory Rate • • Pons Medulla Oblongata Chemoreceptors • • p. CO 2 p. O 2

CO 2 and p. H l l Increase CO 2 • Increase H+ • Decrease p. H Decrease CO 2 • Decrease H+ • Increase p. H

Renal Control for Long Term Acid / Base Balance

Renal processes in A/B balance

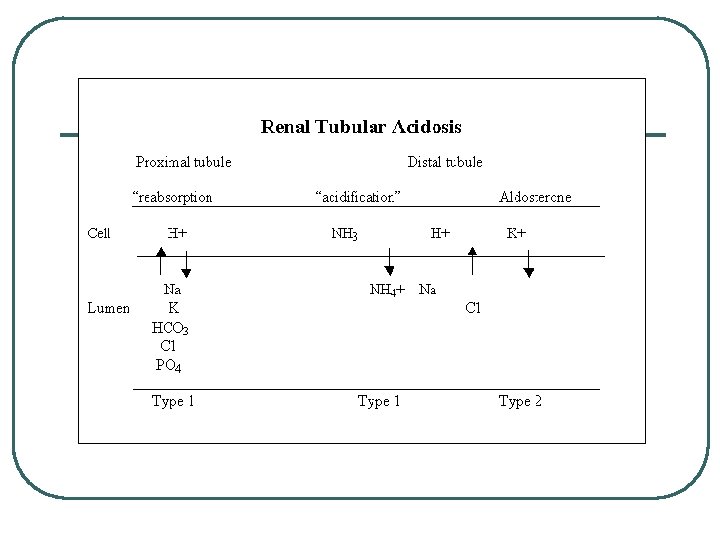
Renal Physiology l l l Filtration • • Remove metabolic acids: Ketones, Uric acid Filter Base [HCO 3 -] @ Renal Filtration Membrane Reabsorption • • Base @ PCT Reverse CO 2 equation to create HCO 3 - Secretion • • H+ @ PCT, late DCT and Cortical CD CO 2 equation to create H+ for secretion

Renal Mechanisms for A/B

Renal Ion Exchanges l l l Na+ / K+ antiporter Na+ / HCO 3 - cotrans H+ / K+ ATPase H+ ATPase Cl- / HCO 3 exchanger

Renal Buffer Mechanisms

Normal Acid Base Values

Respiratory and Renal Balance

Acid-Base Problems l l Acidosis • State of excess H+ Acidemia • Blood p. H < 7. 35 Alkalosis • State of excess HCO 3 - Alkalemia • Blood p. H >7. 45
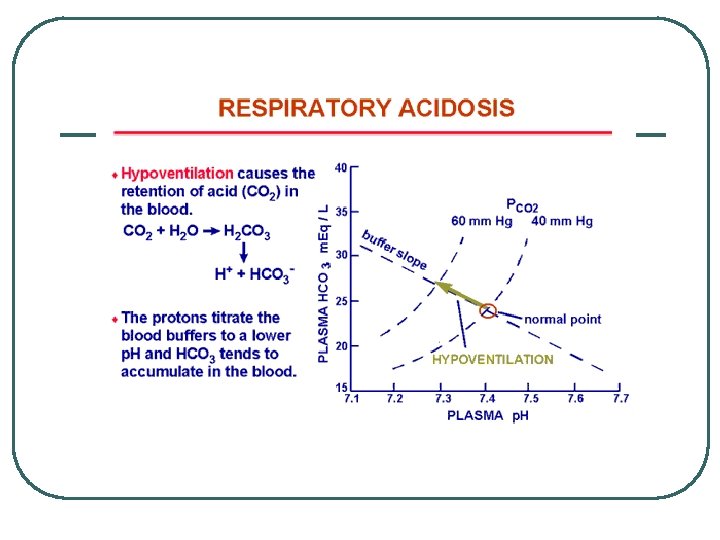
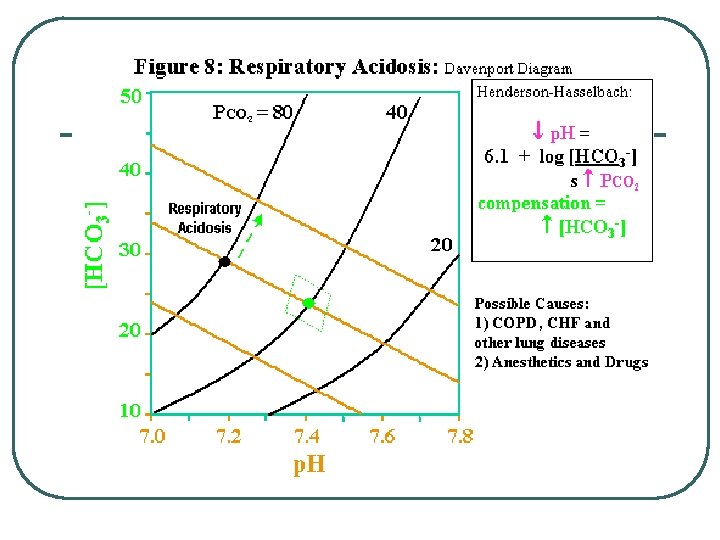
 l l Respiratory Acidosis •")
Classifying Respiratory Acid Base Problems (p. CO 2 changes) l l Respiratory Acidosis • • Respiratory Rate Decreases Any Respiratory Disease • Obstruction • Pneumonia • Gas exchange / transport problems • Respiratory Membrane • RBC / Hemoglobin Respiratory Alkalosis • Respiratory Rate Increases
 l l l Systems")
Classifying Metabolic Acid Base Balance Problems (H+/ HCO 3 -) l l l Systems • • Renal Endocrine GI Cardiovascular / Fluid administration • • Retain Acid Lose Base • • Retain Base Lose Acid Metabolic Acidosis Metabolic Alkalosis

Other System diseases in Metabolic Acid/Base Problems l l l GI • • • Vomiting Diarrhea Medications : Antacids Endocrine • • DM Hyperaldosteronism Metabolism • Increase acid production

Ketones

Compensation

Adjustments for Acid/Base Balance l Imbalance • • Respiratory Acidosis • Compensation • Increase renal acid excretion, Incr HCO 3 - • Decrease renal acid excretion, decr HCO 3 - • Hyperventilate to lower p. CO 2 • Hypoventilate to increase p. CO 2 Incr p. CO 2 Respiratory Alkalosis • l Decr p. CO 2 Metabolic Acidosis • • Decr HCO 3 Incr H+ Metabolic Alkalosis • • Incr HCO 3 Decr H+

Summary for A/B Balance

Questions? Water and electrolytes
- Slides: 70