Acid base balance 3 Dr S Parthasarathy MD
,")
Acid base balance 3 Dr. S. Parthasarathy MD. , DA. , DNB, MD (Acu), Dip. Diabetes, Diploma in Software based statistics, Ph. D ( physiology), IDRA , FICA , Certifícate in USGRA

Blood • • Normal p. H is 7. 36 – 7. 44 < 7. 35 - acidosis > 7. 45 - alkalosis Actually the process is called acidosis The result is called acidemia DKA – process Blood becomes acidemic

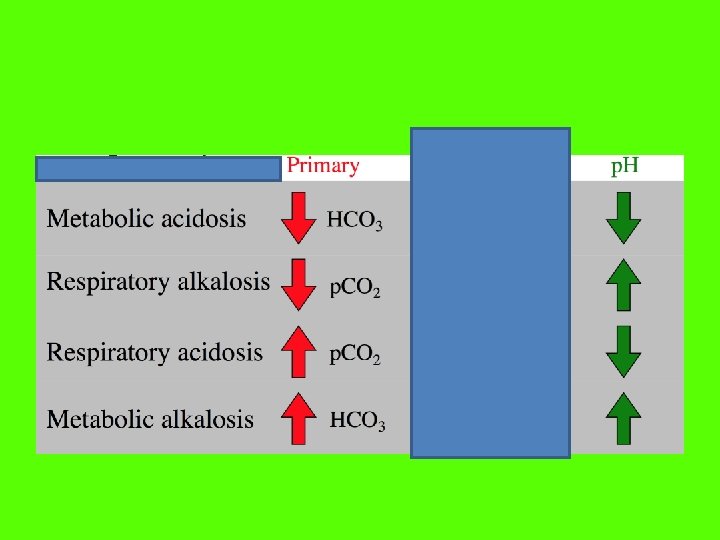
Basic types • Acidosis and alkalosis • Metabolic and respiratory • Acute and chronic

What is metabolic and what is respiratory acidosis • Acidosis that occurs when the lungs fail to remove excess carbon dioxide from our bloodstream during the process of respiration is respiratory acidosis. • Acidosis that occurs when the digestive and urinary systems fail to breakdown and maintain the proper level of acids in the blood is known as metabolic acidosis.

• Respiratory alkalosis is a disturbance in acid and base balance due to alveolar hyperventilation. • Alveolar hyperventilation leads to a decreased partial pressure of arterial carbon dioxide (Pa. CO 2) • Metabolic alkalosis – non respiratory acid exit • Example if a patient vomits and throws acid out

Acute Respiratory acidosis • • CNS lesions Sedatives opioids Pulmonary edema Obstruction FBs Hemopneumothorax Collapse Compensations come last

Chronic Respiratory acidosis • • • Fibrosis COPD Asthma Bronchiectasis Kyphoscoliosis
 Other 'supra-tentorial' causes (pain,")
Respiratory alkalosis • • Head Injury, Stroke Anxiety-hyperventilation syndrome (psychogenic) Other 'supra-tentorial' causes (pain, fear, stress, voluntary) Various drugs (eg analeptics, propanidid, ) Hypoxemia , hyperthyroidism Pulmonary edema – sometimes Compensatory
, Alcoholic Ketoacidosis or")
MUD pilers • Methanol, Metformin • Uremia • Diabetic Ketoacidosis (DKA), Alcoholic Ketoacidosis or starvation ketosis • Paraldehyde, Phenformin (neither used in U. S. now) , Isoniazid (due to Seizures) • Lactic Acidosis • Ethylene Glycol, Ethyl Alcohol Acute Metabolic acidosis • Rhabdomyolysis • Salicylates

Metabolic alkalosis • • • Vomiting Hypokalemia Diuretics Hyperaldosteronism Nasogastric suction

Important clinical terms

Base excess !! Base deficit !! • Base excess as the amount of strong acid (in mmol/L) that needs to be added in vitro to 1 liter of fully oxygenated blood in order to return the sample to standard (normal) conditions (p. H 7. 40, p. CO 2 40 mm. Hg and temperature 37 °C. ) Base excess – alkalosis Base deficit – acidosis

Of course, as the author ? ? Sigaard anderson points out, if blood already has a p. H of 7. 40, a p. CO 2 of 40 mm. Hg and a temperature of 37 °C, then base excess is by definition 0 mmol/L.

Base excess or deficit • A base deficit (i. e. , a negative base excess) can be correspondingly defined in terms of the amount of strong base that must be added. • A further distinction can be made between actual and standard base excess: • actual base excess is that present in the blood, while standard base excess is the value when the hemoglobin is at 5 g/dl. • The latter gives a better view of the base excess of the entire extracellular fluid.
− 24. 8 + [16. 2 ×")
• SBE = HCO 3 (act )− 24. 8 + [16. 2 × (p. H − 7. 40)] • Base excess ( alkalosis ) or deficit ( acidosis) • Indicates a metabolic problem

Standard bicarbonate • Standard bicarbonate is the concentration of bicarbonate in the plasma from blood which is equilibrated with a normal Pa. CO 2 (40 mm. Hg) and a normal p. O 2 (over 100 mm. Hg) at a normal temperature (37°C) Bicarb is 18 and standard bicarb is also 18 Then - metabolic component

Previous Problems • Pitfalls of interpreting acid-base problems by use of standard bicarbonate and base excess can be: • 1. Inaccurate identification of the severity of an underlying acid-base disturbance, • 2. Inadequate estimation of the time course of adaptation to an acid-base disorder (acute versus chronic) • 3. Failure to identify mixed acid-base disorders.

• So came many more terms !!

Anion gap • The anion gap is the difference between primary measured cations (sodium Na+ and potassium K+) and the primary measured anions (chloride Cl- and bicarbonate HCO 3 -) in serum. • {Na+ + K+ } - {Cl- + HCO 3 - } = 8 - 11 • 140 – 130 = 10 • Normal is 8 – 11 • We are electrically neutral !!

Unmeasured anions Minimal unmeasured cations also

Two types • Metabolic acidosis • Normal anion gap • Increased anion gap
 • Oxoproline")
Gold mark – increased anion gap • Glycols (ethylene glycol, propylene glycol) • Oxoproline (pyroglutamic acid, the toxic metabolite of excessive acetaminophen or paracetamol) • L-Lactate (standard lactic acid seen in lactic acidosis) • D-Lactate (exogenous lactic acid produced by gut bacteria) • Methanol (this is inclusive of alcohols in general) • Aspirin (salicylic acid) • Renal Failure (uremic acidosis) • Ketones (diabetic, alcoholic and starvation ketosis)

See the unmeasured anions
 – ( HCO")
Increased anion gap • Anion gap = (Na+ + K+ ) – ( HCO 3 - + Cl-) • There is no increase in Cl • Gap widens • Usually above 22 meq
. A =")
NAGMA – HARDUP • H = hyperalimentation (e. g. , starting TPN). A = acetazolamide use. R = renal tubular acidosis (Type I = distal; Type II = proximal; Type IV = hyporeninemic hypoaldosteronism. D = diarrhea U = uretosigmoid fistula (because the colon will waste bicarbonate). P = pancreatic fistula (because of alkali loss– the pancreas secretes a bicarbonate-rich fluid).

Normal anion gap metabolic acidosis • NAGMA

HCO 3 decreases but Cl increases i. e. the retention or excess of hydrochloric acid • Anion gap = (Na+ + K+ ) – ( HCO 3 - + Cl-)

• Ammonium chloride ingestion • NH 4 → NH 3 + H+ ion • But chloride remains • Anion gap = (Na+ + K+ ) – ( HCO 3 - + Cl-) • NAGMA

RTA • loss of bicarbonate, along with its counterbalancing cation sodium, produces volume contraction, thereby stimulating the renal tubule to retain sodium chloride. • The consequences of these events are the replacement of sodium bicarbonate by sodium chloride. • Anion gap = (Na+ + K+ ) – ( HCO 3 - + Cl-)
 ↓ • Na. HCO 3 excreted ↓")
Examples • Nacl administration (150 + 150) ↓ • Na. HCO 3 excreted ↓ retention of Hydrogen ions and chloride ions NAGMA
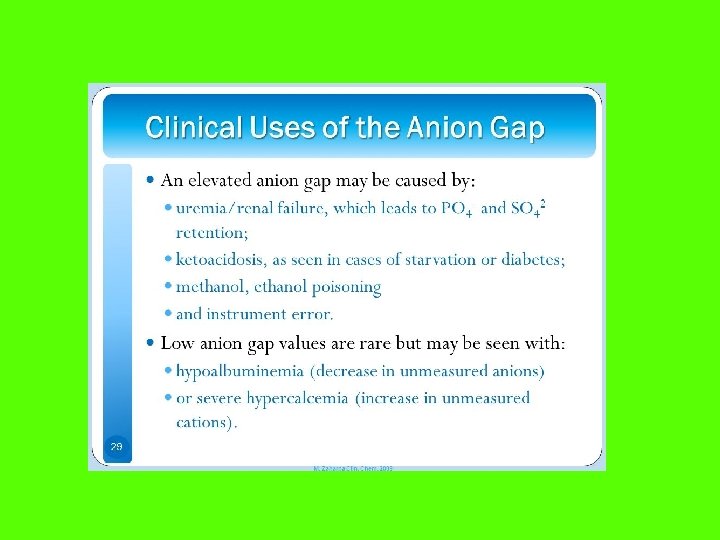

Gaps in anion gap • Serum chloride concentration was raised by approximately 3 m. Eq/L for every 1 -m. Eq/L increase in the concentration of bromide • lithium is a cation, it can lower the serum anion gap when present in sufficient concentration • Hypercalcemia as a result of primary hyperparathyroidism, the serum anion gap was reduced by approximately 2. 4 m. Eq/L

Don’t worry – only two more terms !!
 is the difference between the positively- and")
SID • The Strong Ion Difference (SID) is the difference between the positively- and negatively-charged strong ions in plasma. • Is it simply Na – Cl • Or adding ca, mg this side --- with lactate on the other side • 35 -40

What is delta gap ? ?

Delta gap • • Na = 145 K=4 Cl = 101 HCO 3 = 15 ? acidosis Anion gap = ( 145 + 4) – (105 +15) = 29 Delta gap = anion gap(29) – 12 = 17 17 + 15 ( HCO 3) = 32 Additional metabolic alkalosis

Winters' Formula for Metabolic Acidosis Compensation • expected Pa. CO 2 = [1. 5 x (serum HCO 3)] + 8 [± 2] • if Pa. CO 2 lower, there is a concomitant primary respiratory alkalosis • if Pa. CO 2 higher, there is a concomitant primary respiratory acidosis

Another metabolic acidosis situation • 1. 5 * 15 = 22. 5 + 8 = 30. 5 ± 2 • Pa. CO 2 = 32 • No primary respiratory problem
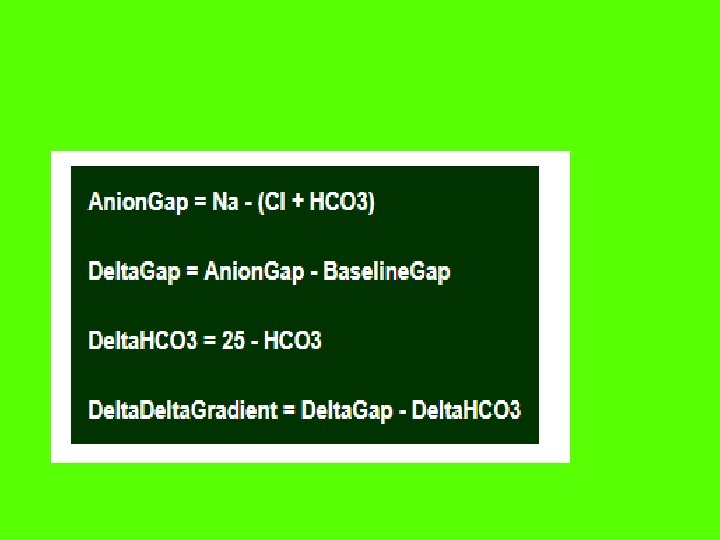

Delta ratio • AG – 12 / 25 – HCO 3 • • < 0. 4 due to a pure NAGMA 0. 4 – 0. 8 due to a mixed NAGMA + HAGMA 0. 8 – 2. 0 due to a pure HAGMA >2. 0 due to a mixed HAGMA + metabolic alkalosis

Summary • • Acidosis and acidemia Types Causes of metabolic and respiratory acidosis Causes of metabolic and respiratory alkalosis Compensations Anion gap, delta gap Base excess Standard bicarbonate
- Slides: 44