Achieving NCQA PCMH Recognition A Step by Step

Achieving NCQA PCMH Recognition: A Step by Step Workshop Friday October 29, 2010 FMEC, Hershey, PA Lee Radosh, MD Associate Director Family Medicine Residency The Reading Hospital &Medical Center Reading, PA Radosh. L@readinghospital. org

Goals & Objectives n n Identify key components of the NCQA recognition application process; Recognize financial models for sustainability of these processes; Identify resources to assist in the process; Delineate key steps in the recognition n process you need to do. Not core goals q q q Teach what a PCMH is Pros/cons of the PCMH Debate about NCQA and the criteria Transformed, NDP Chronic Care Model

Agenda n n n n Intro and needs assessment Brief review of NCQA standards, elements, and scoring Brief review of financial models Demonstrate team/resource development with regard to the application process Examples of materials we submitted Summary Questions/comments/discussion

Needs Assessment n n Who are you? Where are you? How many: q q q Know what a PCMH is? Are familiar with NCQA criteria? Are in the process of applying? Have applied? Have achieved some level of recognition?

My Background n Medical Director, Family Health Care Center q q n n Family Medicine Residency, The Reading Hospital and Medical Center, Reading, PA 13, 000 visits/year Full scope family medicine 7 FT faculty, 6/6/6 residents, 2 sites (in same building) South Central PA Region, PA’s Governor’s Office of Healthcare Reform’s Chronic Care Initiative Faculty, PAFP Residency Collaborative q Assisting 20 programs to “transform” their
 q")
Thanks! n The Reading Hospital and Medical Center Family Health Care Center (FHCC) q q q n n Staff Nurses Residents/Faculty TRHMC Administrative Support GOHCR
 AAFP, AAP, ACP, AOA:")
The Joint Principles of the Patient Centered Medical Home (PC-MH) AAFP, AAP, ACP, AOA: March, 2007 n n n n Personal physician Physician directed medical practice Whole person orientation Care - coordinated and/or integrated Quality of care / culture of patient safety Enhanced access to care Payment reform

“But. . . aren’t we doing that now? ” Are you doing it systematically, AND are you getting paid for it?
 n n n n Currently, the most used")
National Committee for Quality Assurance (NCQA) n n n n Currently, the most used “stamp” of approval Practices can apply for and achieve “recognition” (not certification. . ) Three levels possible Long application Fees involved Can re-apply/get level changed NCQA: PPC (physician practice connection)-PCMH
-PCMH: What it IS n n n Provides valid, reliable and")
Physician Practice Connections (PPC)-PCMH: What it IS n n n Provides valid, reliable and “auditable” means for incentivizing investment in quality infrastructure and processes Encourages practices to adopt proven systems for improving care Complements evaluation of clinical effectiveness, patient experiences, and efficiency

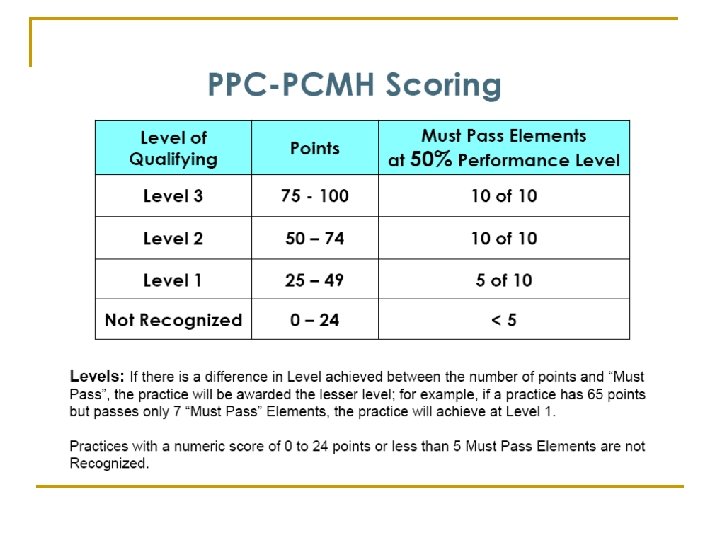
PPC-PCMH: What it’s NOT n The definition of a PCMH q n A tool to “certify” practices as medical homes q n The joint principles (and others as well) “define” the PCMH It qualifies a practice as having met the basic standards that COULD be a PCMH Permanent in content and scoring q Was designed to evolve by January 2011…see: “Planned Evolution of PPC-PCMH Requirements”, NCQA, 8/09

Physician Practice Connections/PCMH January, 2008

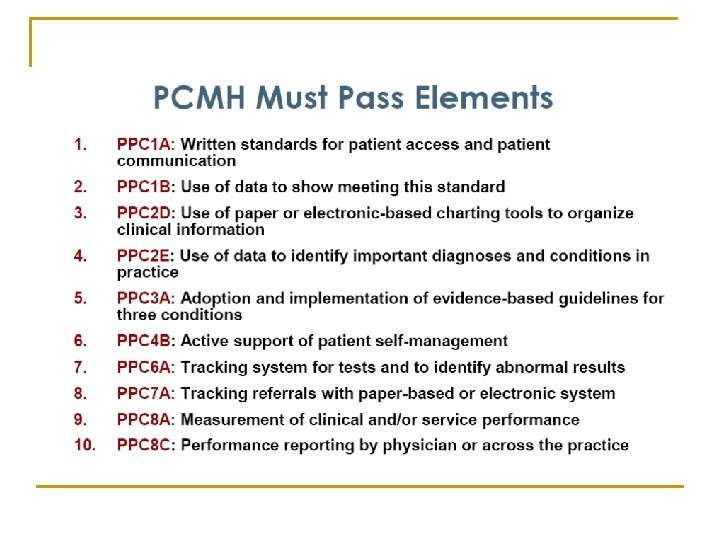
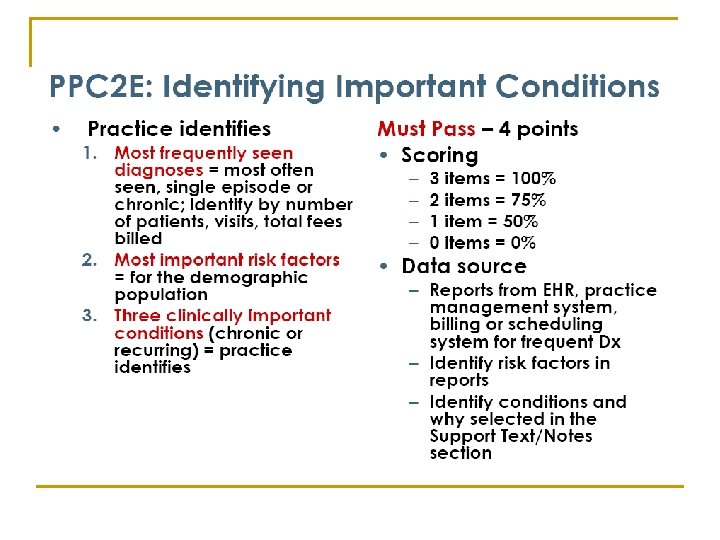
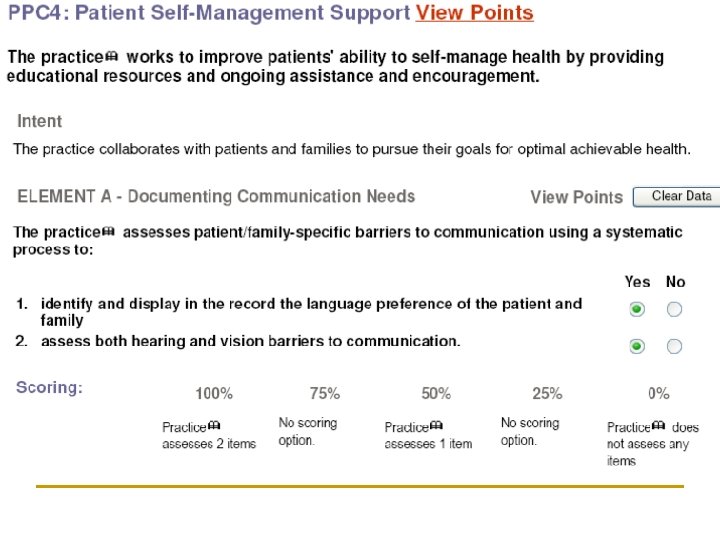
PPC-PCMH Content and Scoring Standard 1: Access and Communication A. Has written standards for patient access and patient communication** B. Uses data to show it meets its standards for patient access and communication** Pt 4 5 9 Standard 2: Patient Tracking and Registry Functions A. Uses data system for basic patient information (mostly nonclinical data) B. Has clinical data system with clinical data in searchable data fields C. Uses the clinical data system D. Uses paper or electronic-based charting tools to organize clinical information** E. Uses data to identify important diagnoses and conditions in practice** F. Generates lists of patients and reminds patients and clinicians of services needed (population management) Pt 2 6 4 3 Pt 3 4 3 5 5 20 Standard 4: Patient Self-Management Support A. Assesses language preference and other communication barriers B. Actively supports patient self-management** Pt 2 4 6 Pt 3 3 2 8 Standard 6: Test Tracking A. Tracks tests and identifies abnormal results systematically** B. Uses electronic systems to order and retrieve tests and flag duplicate tests 3 3 21 Standard 3: Care Management A. Adopts and implements evidence-based guidelines for three conditions ** B. Generates reminders about preventive services for clinicians C. Uses non-physician staff to manage patient care D. Conducts care management, including care plans, assessing progress, addressing barriers E. Coordinates care//follow-up for patients who receive care in inpatient and outpatient facilities Standard 5: Electronic Prescribing A. Uses electronic system to write prescriptions B. Has electronic prescription writer with safety checks C. Has electronic prescription writer with cost checks Pt 7 6 13 Standard 7: Referral Tracking A. Tracks referrals using paper-based or electronic system** Pt 4 4 Standard 8: Performance Reporting and Improvement A. Measures clinical and/or service performance by physician or across the practice** B. Survey of patients’ care experience C. Reports performance across the practice or by physician ** D. Sets goals and takes action to improve performance E. Produces reports using standardized measures F. Transmits reports with standardized measures electronically to external entities Pt 3 3 2 1 15 Standard 9: Advanced Electronic Communications A. Availability of Interactive Website B. Electronic Patient Identification C. Electronic Care Management Support Pt 1 2 1 4 **Must Pass Elements

Does the Medical Home Work… Will the PCMH improve Quality AND Save $$

PA Chronic Care Initiative: How Is It Funded? Somewhat novel pilot project n NOT tax dollars n Private insurers n

Right State Right Place Right Now

A 1 C Levels SEPA Collaborative Results Presented May 2009 R. Gabbay, MD, Ph. D. , Faculty Chair

Blood Pressure Control SEPA Collaborative Results Presented May 2009 R. Gabbay, MD, Ph. D. , Faculty Chair

Cholesterol Control SEPA Collaborative Results Presented May 2009 R. Gabbay, MD, Ph. D. , Faculty Chair

Annual Foot Exam SEPA Collaborative Results Presented May 2009 R. Gabbay, MD, Ph. D. , Faculty Chair

Annual Eye Exam SEPA Collaborative Results Presented May 2009 R. Gabbay, MD, Ph. D. , Faculty Chair

Self Management Goals SEPA Collaborative Results Presented May 2009 R. Gabbay, MD, Ph. D. , Faculty Chair

Community Care of North Carolina • Since 1999, the state has invested in many MH components through disease management payments to practices with Medicaid pts. • Emphasis on • physician led team approach • disease tracking • care managers within practices • Significant improvements in • cost, utilization, and quality measures • SAVINGS of $230 -$260 million in 2004.

Geisinger Medical Home Sites and Hospital Admissions Hospital admissions per 1, 000 Medicare patients Source: Geisinger Health System, 2008.

Marillac Integrated Care Network Grand Junction, Colorado

Independence Blue Cross

Independence Blue Cross

How Will You Get PAID in the Future? n Probably a hybrid: q Traditional visits n q Care/population management n q Per member, per month? Quality outcomes n q E&M, face to face Pay for performance Payments from hospital n Reduce re-admissions

Any Recent “Political” Changes Affecting This? n n Yes! Medicare changes – no reimbursements for: q q n Hospital-acquired infections Readmissions CMS leadership

Who Is This Man?

Resources: Get To Work!

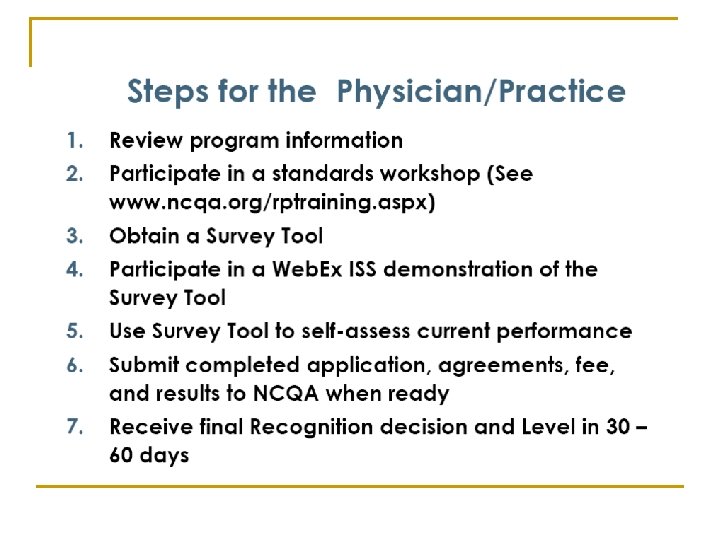
SOME KEY STEPS n n n n Delineate team members KNOW NCQA standards, elements, processes Assign tasks Develop rough timelines Meet regularly Use workbooks (or something!) for tracking Don’t re-invent the wheel! q Use resources, webinars, Power. Points, etc.

Supporting Processes n “What was your exact office process? ” q q n NCQA team Nurse manager, office manager CRITICAL here Who, what, where, when, how, and how often? q Team, divided tasks, met about every 2 -3 weeks

n n n Sample FHCC: We used this as a guide Early one-hour meeting q q q Went through all standards/elements Divided items. . At the element level! Even the question level Re-assigned as needed
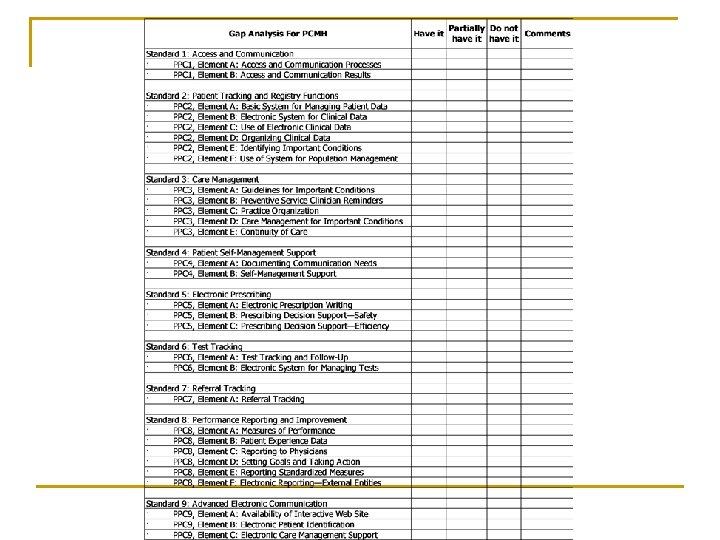

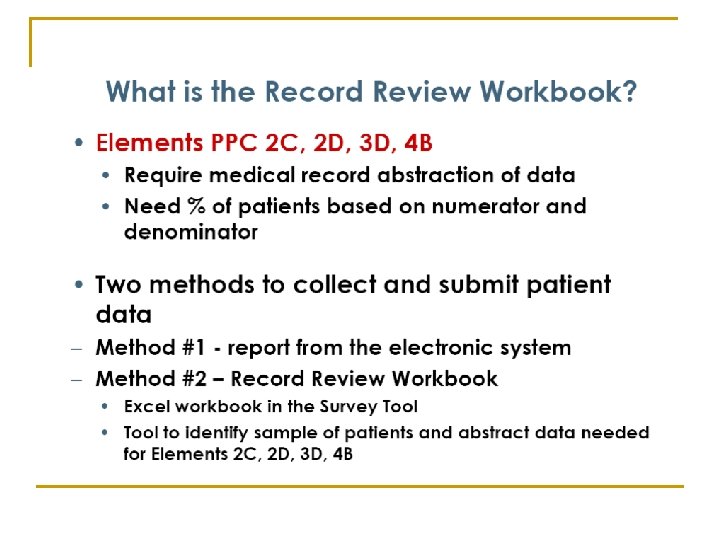
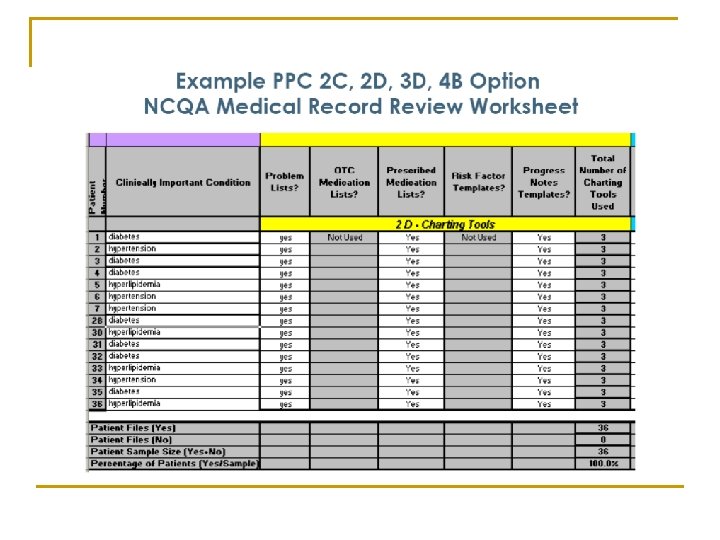
Project Management Workbooks
 for NCQA’s")
© Colorado Clinical Guidelines Collaborative Revised November 2009 CCGC’s Workbook (Version 3) for NCQA’s Physician Practice Connections®―Patient-Centered Medical Home™ (PPC®-PCMH™)

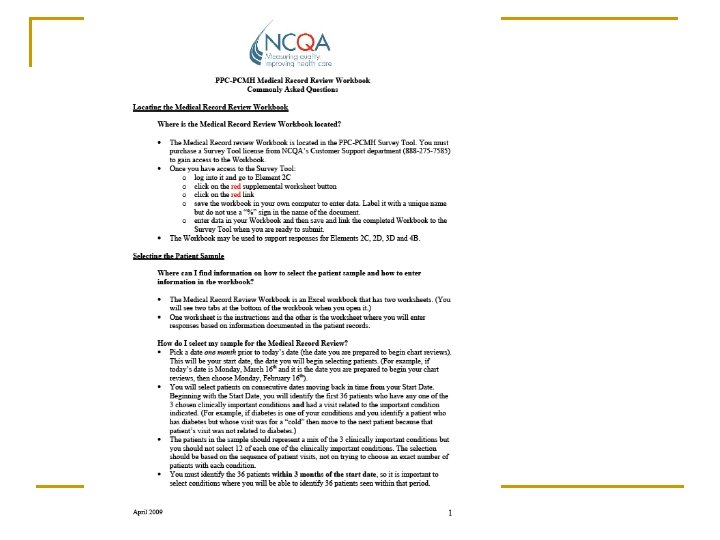
Use NCQA’s FAQ’s for each standard!

Three Conditions n n Choose wisely Include DM q Low-hanging fruit n n q n n Objective data available EBM guidelines P 4 P (used for every insurer!) Must be able to meet other elements’ requirements with these conditions Consider lipids, HT, CHF

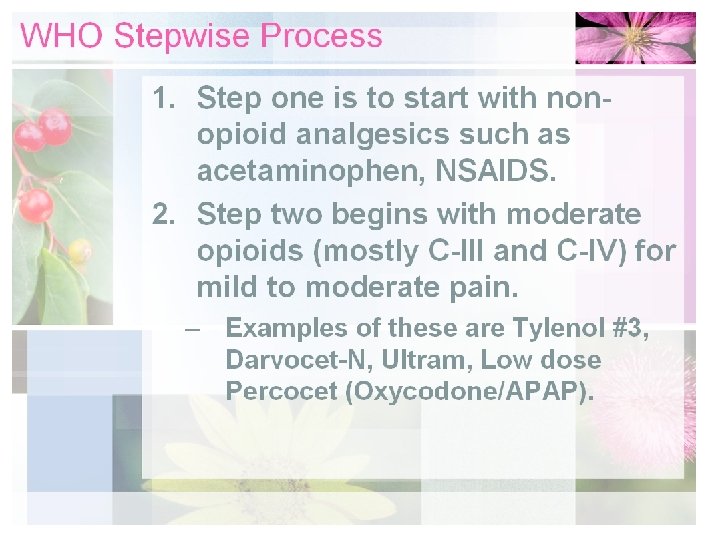
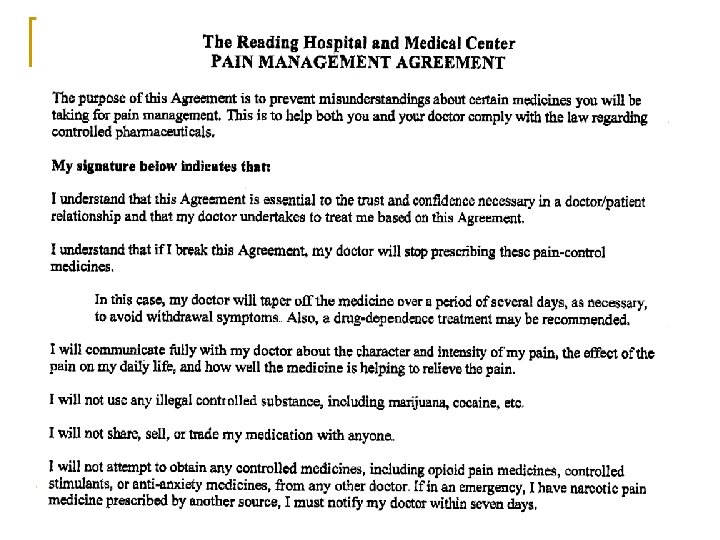
What We Chose n n I list these to make you think about your local environment, resources Our three q q q n n DM Prenatal Care Chronic Pain I checked with NCQA first Why? q q q Already had been doing PCMH type stuff for these We hadn’t routinely done this for lipids, HT Buy-in. .
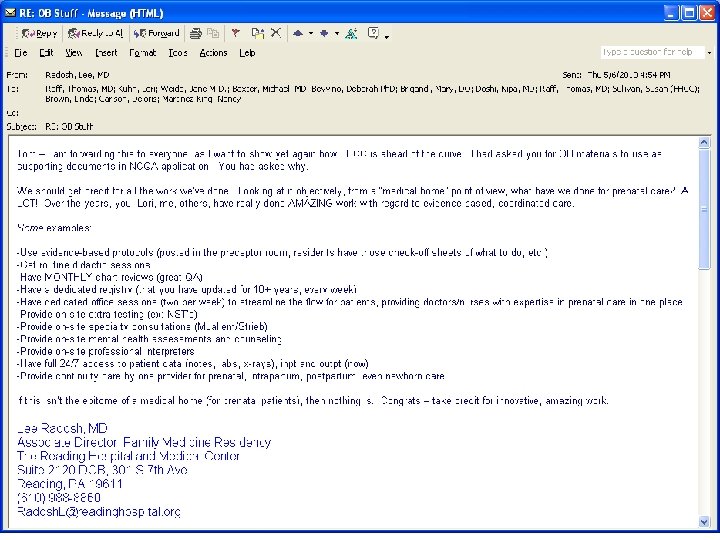

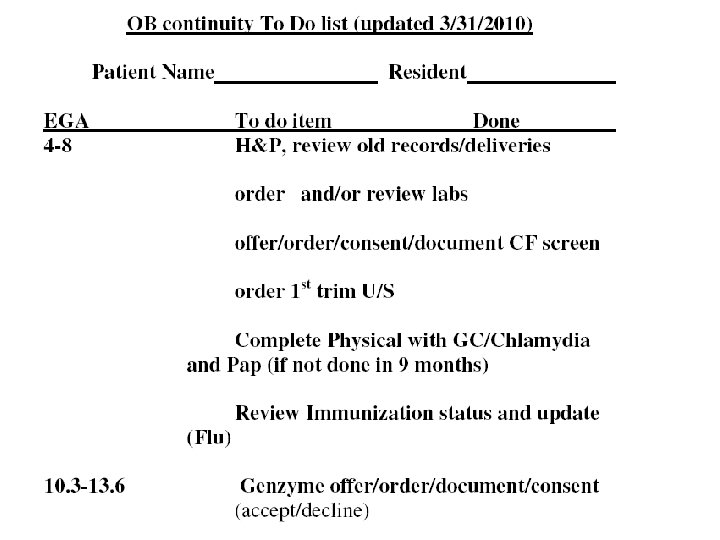
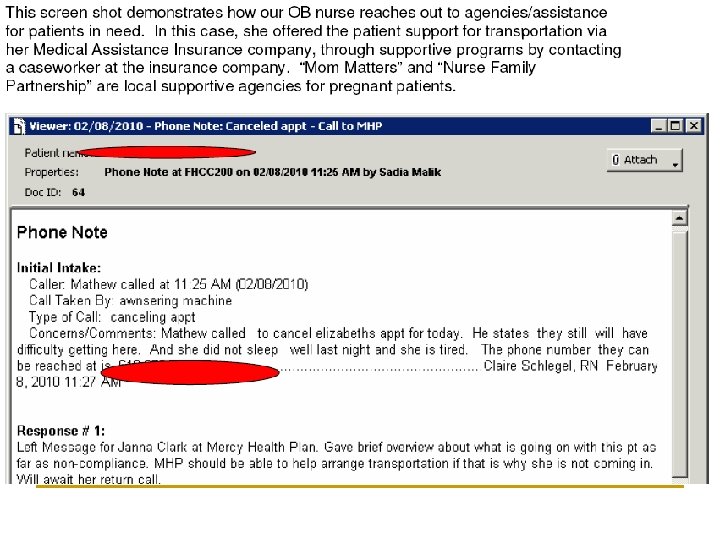
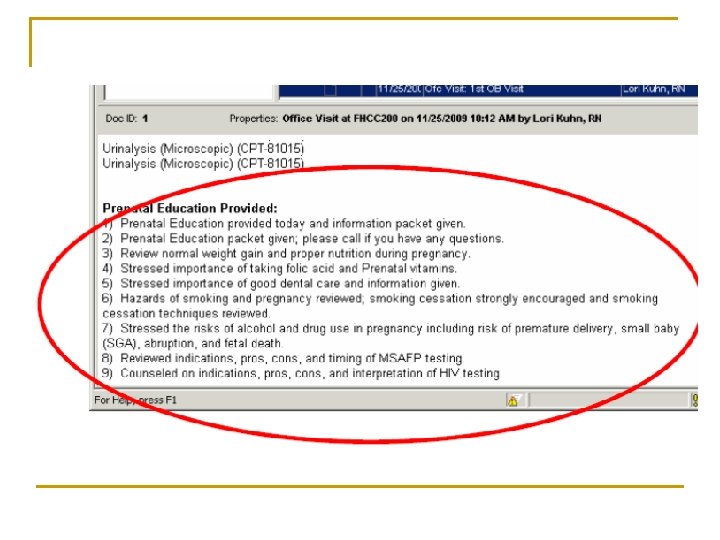
Motivator! n n Using prenatal care as a chronic condition: a source of pride We had already done this – for years q q q Prenatal registry Regular chart reviews EBM guidelines followed On-site high-risk consults Coordination with multiple agencies n One-stop shopping q q q Primary physician visit OB consult when indicated Nurse/social support Psychologist Testing (NST) This demonstrated to everyone we could do this!

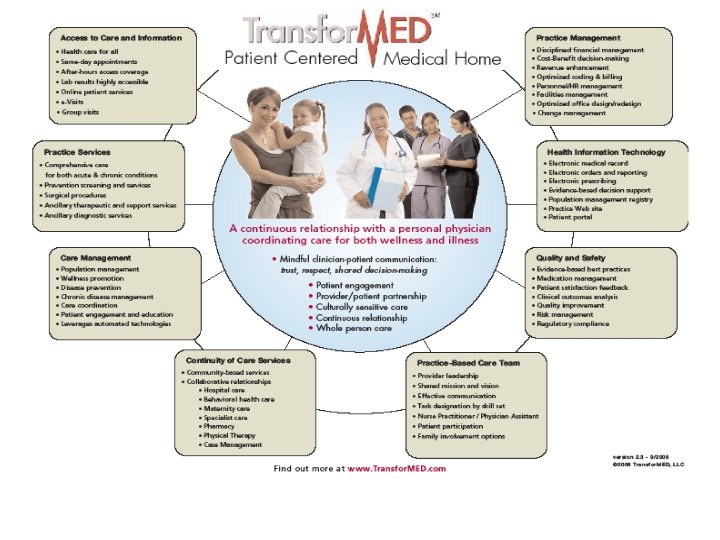
Transformed
 approach this? For")
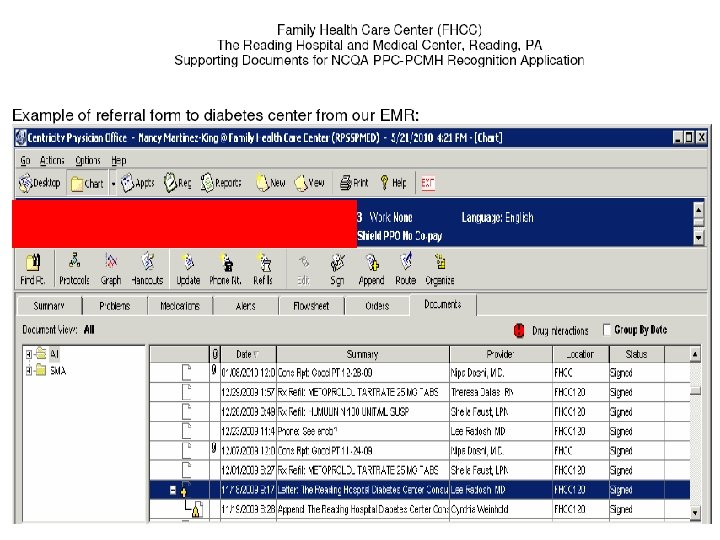
Formatting n n n How did FHCC (Family Health Care Center) approach this? For each element, we never used the “Support text/notes” box We always used: q q n The “documents” box An MS-Word Template with standard formatting Why? q q Team consistency Polished, organized appearance

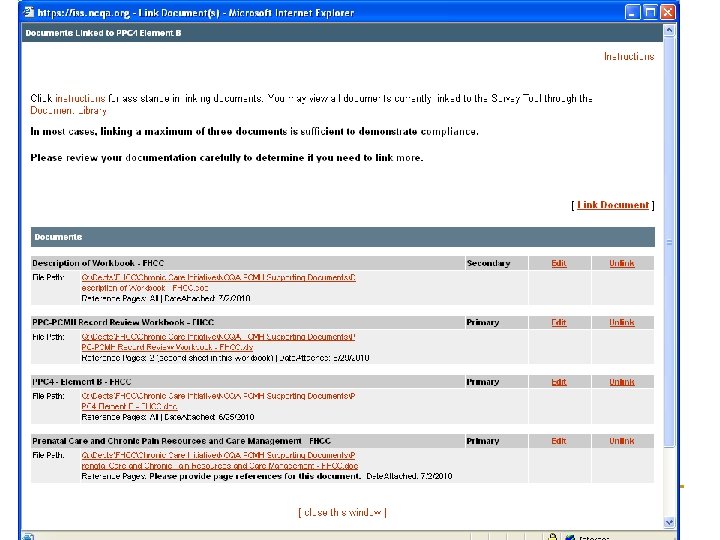
Linked our standard Word document description here Link to the Workbook

Sample FHCC document
 on EVERY page Standardized titles/format of each document")
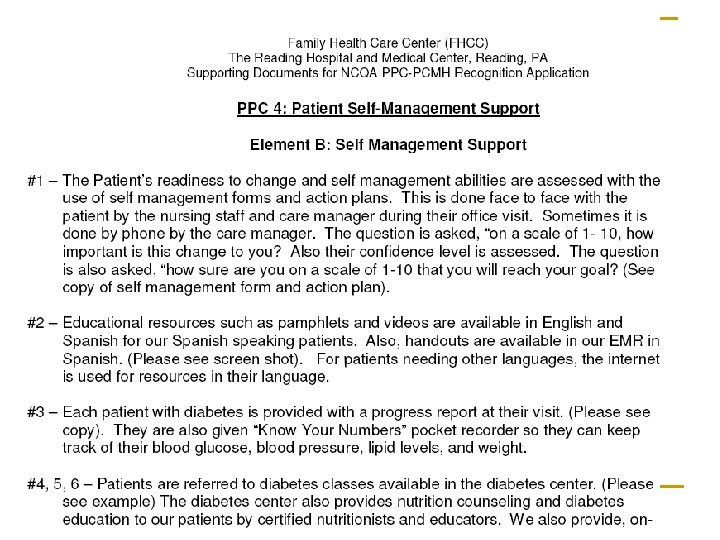
Same header (using headers and footers) on EVERY page Standardized titles/format of each document Clearly delineated elements/answers in the text

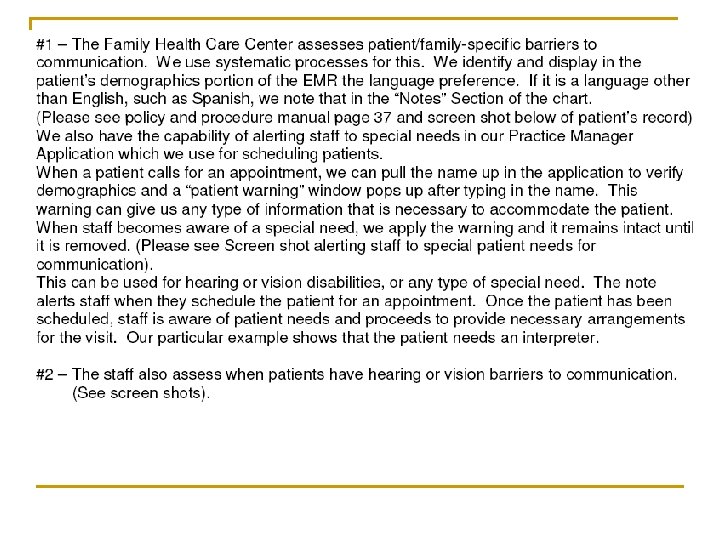
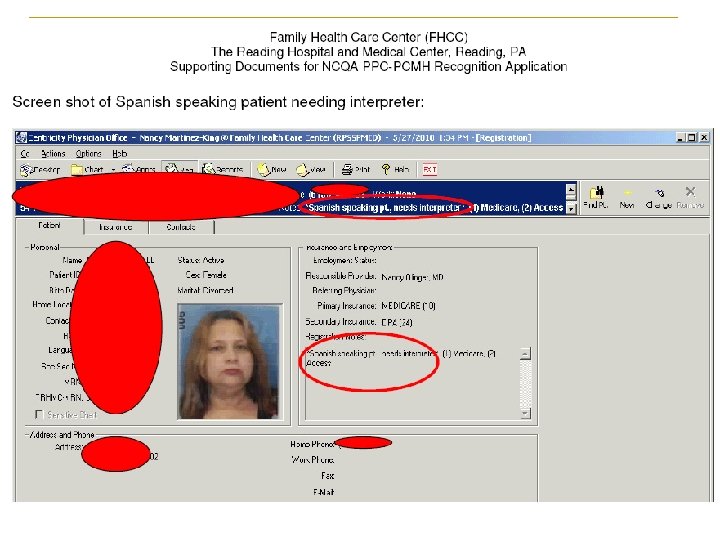
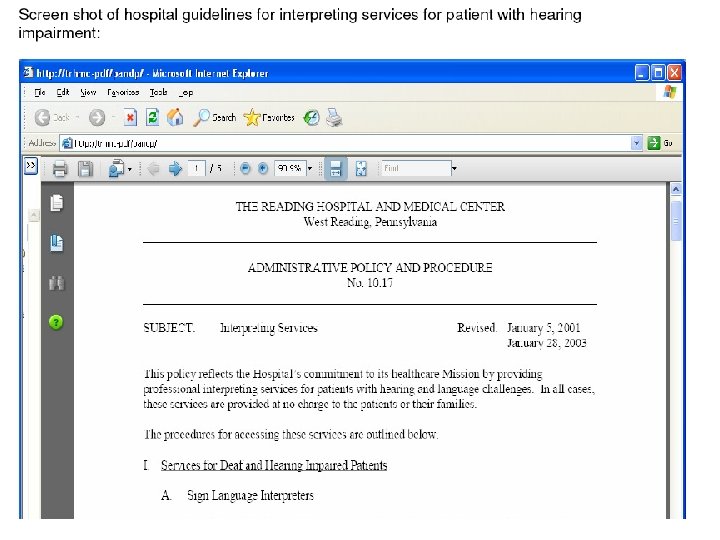
Supporting Documents for Element A

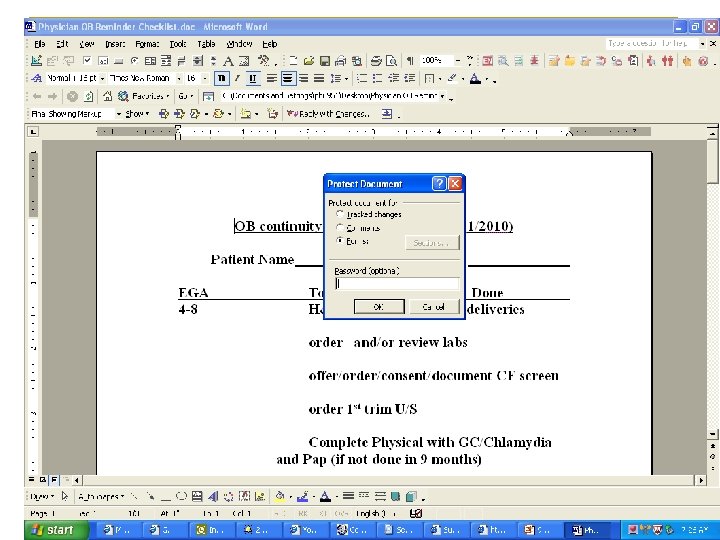
Confidentiality? n n Maybe this was overkill, but we: Blocked any patient identifying information “Protected” the document Can someone receiving your document “Save as” or unblock the confidential info? q n Then, do something else How? q q MS Word Tools menu Protect document Choose password

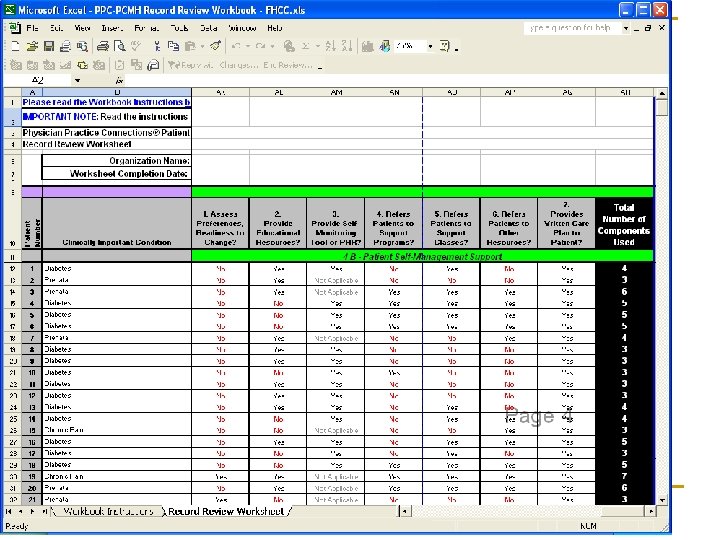
PPC 4: Self-management Support Must pass element!
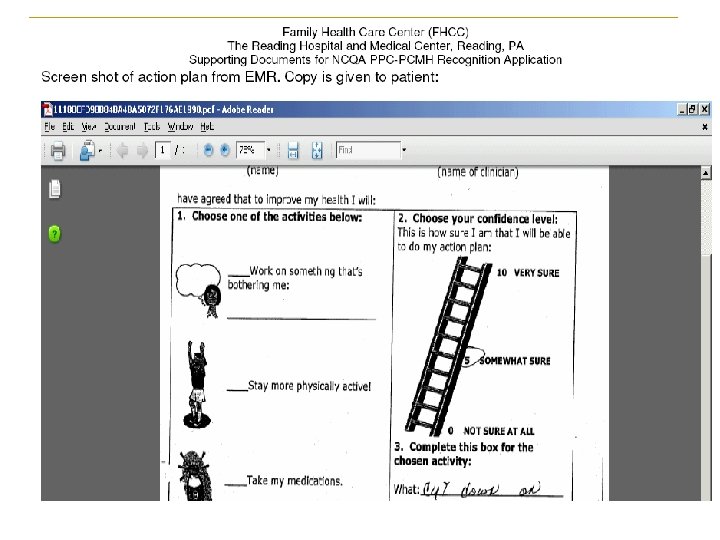
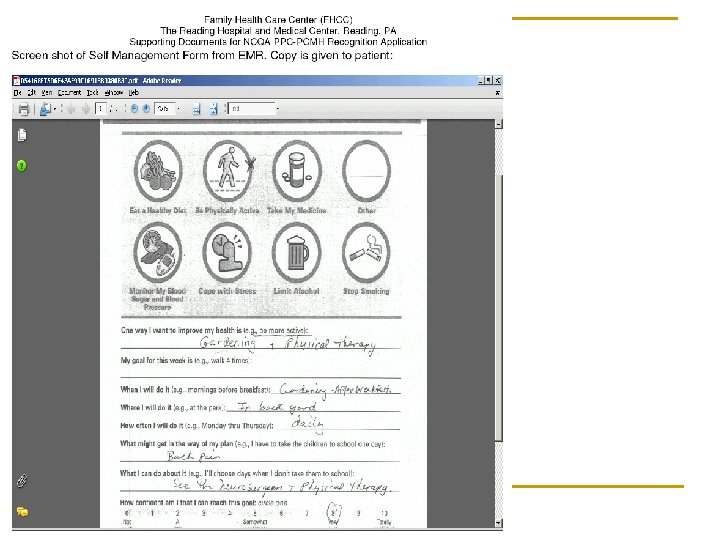
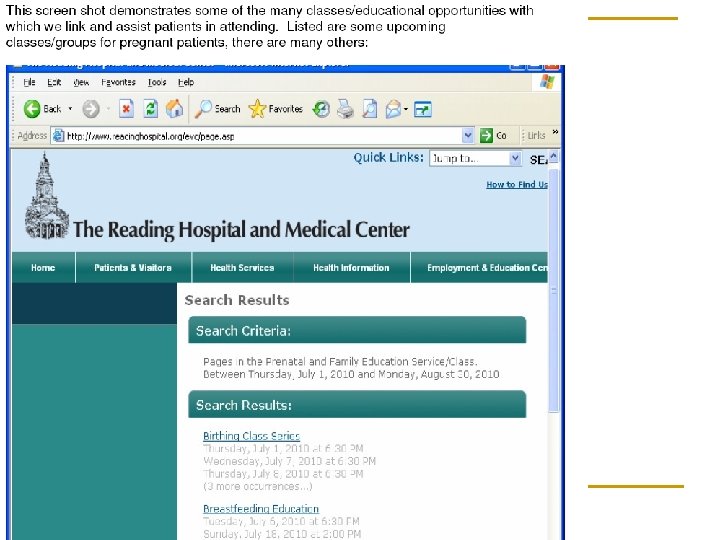

Supporting Tools or Resources n Cute PDF Writer q q q n n n Snagit What tools did you use? Policies and procedure examples q q n n Free, easy download Print ANY document & convert to PDF Great for screen shots, etc. Look within (program, hospital, departments) Don’t re-invent the wheel Staff training (ex: SMS / motivational interviewing) Outside resources q q Community resources (and screen shots) Websites (maybe pt ed you use, SMS sheets)

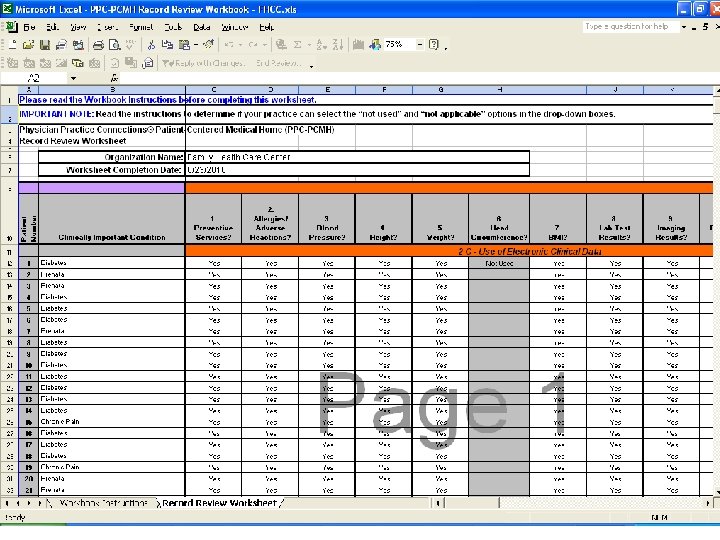
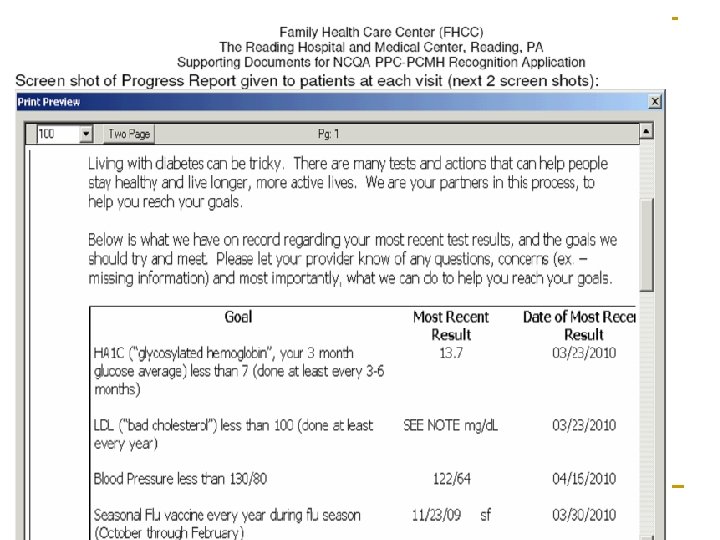
Documentation and Tracking n How did you capture /document your efforts? q n n q Used consistent forms/formatting q What reports did you use/ create to view your performance across your population? q q Excel (from our collaborative) Registries (that already existed!) Screen shots we used/captured q q n EMR FHCC Policies & Procedures Manual Hospital policies Patient ed materials Educational Power. Points Emails Be CREATIVE! q Think: what do you have/do and take for granted

Documentation and Tracking: Pearl What is “obvious” / taken for granted on your end, is DOCUMENTATION on NCQA end!

n SUMMARY POINTS: KEY Decide why you are. STEPS doing this q n n n n If no buy-in, you CAN’T do it Delineate team members KNOW NCQA standards, elements, processes Envision viability (financial “rewards”? ) Assign tasks Develop rough timelines Meet regularly Use workbooks (or something!) for tracking Don’t re-invent the wheel! q Use resources, webinars, Power. Points, etc.

“Not everything that can be counted counts, and not everything that counts can be counted. ” ~Albert Einstein


THANK YOU!
- Slides: 91