Achieving Health Equity and Providing Quality Care Joseph
























 75% 65%")







, the")








- Slides: 43
Achieving Health Equity and Providing Quality Care Joseph R. Betancourt, M. D. , M. P. H. Director, The Disparities Solutions Center Senior Scientist, Institute for Health Policy Director for Multicultural Education, Massachusetts General Hospital Associate Professor of Medicine, Harvard Medical School
Outline u Disparities, Equity and Quality u Building the Foundation: Data Collection & Monitoring u Moving to Action: Improving Quality & Achieving Equity u Achieving Spread: The Disparities Leadership Program
Disparities, Equity and Quality
Diabetes-Related Death Rate, 2010 Deaths per 100, 000 population
Disparities in Health Care 2002 Racial/Ethnic disparities found across a wide range of health care settings, disease areas, and clinical services, even when various confounders (SES, insurance) controlled for. Many sources contribute to disparities—no one suspect, no one solution • System factors • Provider factors • Patient factors
IOM’s Unequal Treatment www. nap. edu Recommendations u Increase awareness of existence of disparities u Address systems of care – Support race/ethnicity data collection, quality improvement, use of EGB’s, multidisciplinary teams, community outreach – Improve workforce diversity – Facilitate interpretation services u Provider education – Health Disparities, Cultural Competence, Clinical Decisionmaking u Patient education (navigation, activation) u Research – Promising strategies, Barriers to eliminating disparities
Quality Health Care u Health care should be – Safe – Effective – Patient-centered – Timely – Efficient – Equitable
Linking Disparities to Cost, Quality and Safety u Safe – Minorities have more medical errors with greater clinical consequences u Effective – Minorities received less evidence-based care (diabetes) u Patient-centered – Minorities less likely to provide truly informed consent; some have lower satisfaction u Timely – Minorities more likely to wait for same procedure (transplant) u Efficient – Minorities experience more test ordering in ED due to poor communication u Equitable – No variation in outcomes u Also – Minorities have more CHF readmissions, ACS admissions, and longer LOS 8
Cost of Disparities u. Between 2003 and 2006, the combined direct and indirect cost of health disparities in the United States was $1. 24 trillion (in 2008 inflation-adjusted dollars).
Building the Foundation: Data Collection and Monitoring
Achieving Equity v Key Process v. Collect Data v. Identify and Report by R/E v. Implement Solutions v. Evaluate v. Strategic Planning
MGH Disparities Committee 2003 Underlying Principle u While data specific to disparities at MGH important, not necessary to begin to take action given IOM Report documented issue nationally Charge u Identify and address disparities in health and health care wherever they may exist at MGH – Subcommittees: Quality, Pt Experience, Education/Awareness – Present plan and results to Board, Executive Council and other hospital leadership regularly
Data Collection Perceived Challenges u Collection of information is illegal u Patients won’t want to provide information u Registrars won’t want to collect information (have history of just deciding patient info) u Process will take too long, impede registration u Adapting IT systems to collect info costly u Uncertain how information will be used
Data Collection: Timeline Prior to 2003 u Collected R/E data in 5 basic categories and preferred language u Registrars asked basic questions u Little training or quality assurance u No preamble to collection of data u No campaign to inform patients of purpose u Information not linked to quality data
Data Collection: Timeline 2003 u Boston Mayor convenes Hosp CEO’s & Community Leaders – Agree to effort to address disparities in health and health care – Boston hospitals to be required to collect race/ethnicity 2004 u Piloted new method of collection – 3 models among 7000 patients (R/E, subgroup, language, education) – Metrics: Collects key info in timely fashion in way patients could understand u Registrars receive intense training and QA Process – Includes preamble, methods to respond to questions u u City releases PR Poster Campaign MGH passes policy that all Quality Data will be stratified by race/ethnicity and language
Data Collection: Timeline 2006 u MA Health Care Reform requires race/ethnicity, language, and highest level of education to be collected u MGH begins preparation of Disparities Dashboard – – – Poster campaign series and website unveiled Disparities questions incorporated in Quality Rounds Patient Experience Survey Conducted Multicultural Advisory Board Convened Patient Satisfaction stratified by race/ethnicity, and language 2007 u MGH develops first Disparities Dashboard u Disparities found, interventions developed 2008 u MGH begins public reporting via web
Initial Disparities Dashboard u Welcome and Purpose – Definition of Disparities u Focus on disparities in care – Purpose of Dashboard u Annual Report u Embedded into Q and S Reporting – Data and Measurement u How race/ethnicity data collected – Process, categories u Data Sources – IDX, PATCOM, TSI, H-CAHPS survey data, medical record review (Core/NHQM) u Snapshot of diversity of MGH patients – Who they are and where they are seen
Initial Disparities Dashboard u Measures – Clinical quality indicators u Inpatient: National Hospital Core Measures – AMI, CHF, CAP, SCIP u Outpatient: HEDIS Measures – Mammogram, Pap, CRC Screening – Diabetes, Coronary Artery Disease – Physician, Practice Linkage – Patient Experiences with Care u Press-Ganey Inpatient satisfaction by r/e u Results of Quality Rounds u Results of Minority Survey – Communication with LEP patients
Disparities Dashboard Evolution u H-CAHPS Inpatient satisfaction by race/ethnicity u All-cause and ACS Admission by race/ethnicity u CHF Readmissions by race/ethnicity u Sentinel Measures – Mental Health – Pain Mgmt in the ED – Wait time for Renal Transplantation u New Minority Patient Experience Survey u Interpreter Pilot Project u Cross-Cultural Communication Training Report
Disparities Dashboard Executive Summary – Green Light: Areas where care is equitable u National Hospital Quality Measures u HEDIS Outpatient Measures (Main Campus) u Pain Mgmt in the ED – Yellow Light: National disparities, areas to be explored u Mental Health, Renal Transplantation u All cause and ACS Admissions (so far no disparities) u CHF Readmissions (so far no disparities) u Patient Experience (H-CAHPS shows subgroup variation) – Red Light: Disparities found, action being taken u Diabetes at community health centers – Chelsea (Latino), Revere (Cambodian) Diabetes Project u Colonoscopy screening rates – Chelsea CRC Navigator Program (Latinos)
Moving to Action: Improving Quality and Achieving Equity
Culturally Competent Disease Management: The MGH Chelsea Diabetes Program Collaboration of the Disparities Solutions Center, Chelsea Healthcare Center, and the MGPO A quality improvement / disparities reduction program with 3 primary components: • Telephone outreach to increase rate of Hb. A 1 c testing • Individual coaching to address patients’ needs and concerns regarding diabetes self-management to improve Hb. A 1 c • Group education meeting ADA requirements *Also focus on link between mental health, chronic disease management, and prevention
* * Chelsea Diabetes Management Program began in first quarter of 2007; in 2008 received Diabetes Coalition of MA Programs of Excellence Award
Chelsea CRC Navigator Program u CRC Navigator Program – Initiated 2005 – Use of registry to identify individuals, by race/ethnicity, who haven’t been screened for colon cancer – Navigator contacts patient (phone or live) – Determine key issues, assist in process u Education u Exploration of cultural perspectives u Logistical issues (transportation, chaperone) – GI Suite facilitates time/spaces issues
CRC Screening Over Time Chelsea Patients Latino White CRC Screening Completion (%) 75% 65% 55% 45% 35% 2005 2006 2007 2008 Year 2009 2010
Health Care Provider and Staff Training § § § Quality Interactions Cross-Cultural Training offered as option as part of MGPO QI Incentive in Q 3 2009; case-based, evidence-based, interactive e-learning program which allows learners to develop a skill set to provide quality to patients of diverse cultural backgrounds 987 doctors completed; more than 88% said program increased awareness of issues, would improve care they provide to patients, and would recommend to colleagues; average pretest score 51%, posttest score 83% Training 3000 frontline staff with Healthcare Professional Version 1. Available at: http: //www. qualityinteractions. org/prod_overview/clinical_program_features. html.
New Initiative: Patient Experience Survey u Goal: – Gain additional insight into the experiences of diverse patients and harder-to-reach vulnerable populations u Methods: – 800 interviews, stratified by R/E, ambulatory, ED, and inpatient (will include Peds, and possibly mult languages) – Self-administered paper survey and telephone follow-up u Instrument: – MGH 2004 Disparities Survey with modifications – Standard patient experience domains and disparitiesrelated issues, including experiences of perceived discrimination or unfair treatment u Preliminary results expected Fall 2012 *Funded by the MGH Center for Quality and Safety
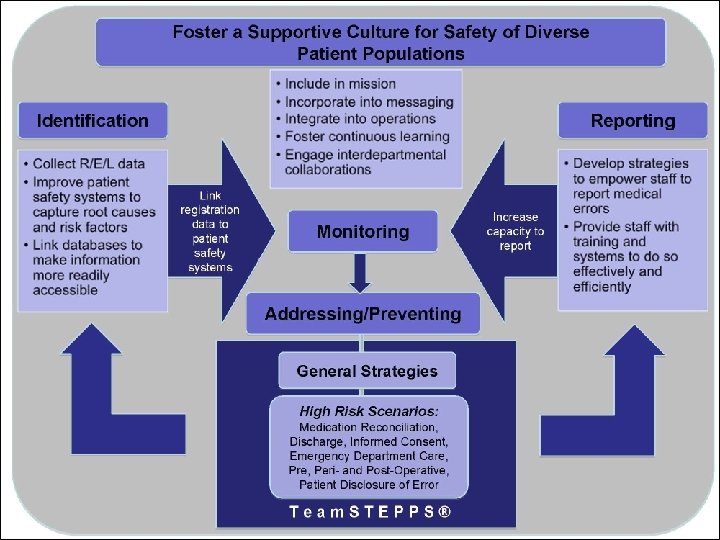
New Initiative: Improving Safety in Patients with Limited-English Proficiency u u u Funded by Agency for Health Care Research and Quality (AHRQ) Disparities Solutions Center in collaboration with Abt Associates, Inc. , Cambridge Project Years: 2009 -2012 Project Goals • A hospital guide on preventing, identifying, and reporting medical errors due to language barriers and cross-cultural communication problems. • A new Team. STEPPS® training module, focused on team behaviors to improve safety in LEP and culturally diverse patient populations
MGH New LEP Safety Initiatives u Interpreter Rounds – Medical interpreters will conduct rounds to assess quality of care and patient experience of LEP patients u Executive Quality and Safety Rounds – Executive rounds will include manager of interpreter services to incorporate focus on role of language and cultural factors u Training – Interpreter Training: Patient Safety 101, Reporting, Communication Tools via Team. STEPPS® LEP Module – Provider Training: E-Learning Program on partnering with interpreter services and tools for working with interpreters
New Initiative: MGH Patient Activation Poster Campaign u Launched: June 2011 u Languages: English and Spanish u Long Term Plans: Expand to other languages, ideally evaluate impact of poster campaign on patientprovider communication and error reduction
Achieving Spread: The Disparities Leadership Program
The Disparities Leadership Program u One year, Exec Q/S, Distance Learning Program u Develop cadre of leaders in health care equipped with – Knowledge of disparities, root causes, research-to-date – Cutting-edge QI strat’s for identifying/addressing disparities – Leadership skills to implement and transform organizations u Assist individuals and organizations to: – Create a strategic plan to address disparities, or – Advance or improve an ongoing project, and – Be prepared to meet new standards and regulations from the JC, NCQA, and health care reform
Our Experience: The Disparities Leadership Program • From 2007 to 2012 (5 Cohorts), the Disparities Leadership Program trained: • 190 participants from 86 organizations • 43 hospitals • 16 health plans • 17 community health centers • 1 hospital trade organization • 1 federal government agency; 1 city government agency • 7 professional organizations • Representation from 28 states, along with the Commonwealth of Puerto Rico and Switzerland
DISPARITIES LEADERSHIP PROGRAM 2012 Project Description AIM Statement We aim to improve the accuracy and collection rate from 81% to 95% for Race, Language, Ethnicity, Hispanic/Non-Hispanic, and Religious Preference (REAL Plus) data collection for UC Davis Health System within the next fiscal year (July 1, 2012 – June 30, 2013) and pre-work to begin in May 2012. Project Scope The DLP Project Team assisted us in “scoping” our project in specifically on developing strategic plans to achieve the below indicated milestones: Development of system-wide curriculum and ongoing training program for all staff with competencies in collection of REAL data Design of efficient infrastructure to measure patient experience outcomes with REAL Data Collection REAL Data using CG CAHPS Cultural Competence Survey Integration Ability to VALIDATE “accuracy” of collection of REAL Data with Coaching and Improvement Plan Implemented Disparities Leadership Program 2012 -2013
Goal The goal of our project is to research and develop a disparities dashboard to identify and strategically address An. Med Health’s most vulnerable, underserved and costly patient populations. The disparities dashboard will be adjunct to our system-wide quality management strategies. Project Objectives • • • Establish dashboard implementation team Establish dashboard framework Establish priority populations System engagement Project Evaluation & Phase II Assessment
Appropriate Care Scores
Measuring Equity: Lessons Learned Annette Johnson, MBA Quality Analyst Alameda County Medical Center “To measure is to know”…“If you cannot measure it, you cannot improve it” Lord Kelvin, William Thompson, 1824 -1907 Alameda County Medical Center
Anatomy of a Dashboard Graph Data for Visual Impact Eliminate Excessive Nuance Highlight Asks and Actions Alameda County Medical Center
Balance What is Measured Dashboard Strategies Aim for quick wins Highlight Bright Spots Alameda County Medical Center
Summary u There is a significant body of evidence that has identified racial/ethnic disparities in health care, and impact on cost, quality and safety u Hospitals can play a major role in their elimination through quality improvement – Essential elements include data collection, monitoring, quality improvement, provider and patient interventions u Efforts to improve quality and achieve equity will improve the care not only of minorities, but of all patients
Thank You Joseph R. Betancourt, MD, MPH jbetancourt@partners. org www. mghdisparitiessolutions. org www. qualityinteractions. org