Acetylcholine v Has little therapeutic value v Has













 v Urinary retention (Bethanechol) v Glaucoma")





 v Treatment of MG (Pyridostigmine)")
 v Autoimmune (autoantibodies to NM in NMJ) v Reduction in receptor")

")
 v")

")



 v OP compound v Irreversibly inhibits CE v Insecticide v Toxicity: excessive")
")



 b) Anti-muscarinic drug: Atropine-like drugs, Hyoscine (Scopolamine) Anti-nicotinic drugs Ganglion")

 • Alkaloids obtained from Atropa Belladona, Considered as prototype for")



 Some may produce sedation (Hyoscine) Hyoscine blocks M receptors")
 §Cycloplegia (relaxation of the ciliary muscle) cause: blurred vision")

 inhalation: ◦")



 produce mydriasis and cycloplegia In iritis")
 Bronchial asthma:")






 blockers The first drug known to block the skeletal")

- Slides: 67
Acetylcholine v Has little therapeutic value v Has multiple actions v Has short t ½ v Activates muscarinic & nicotinic receptors 3/3/2021 1
Pharmacodynamics of Ach q Muscarinic stimulation: v On the CVS: Ø-ve chronotropic & inotropic effects ØDecrease stroke volume & cardiac output ØDecrease ABP: Ø Stimulation of vascular M 3 receptors Ø Increase NO release from endothelium 3/3/2021 2
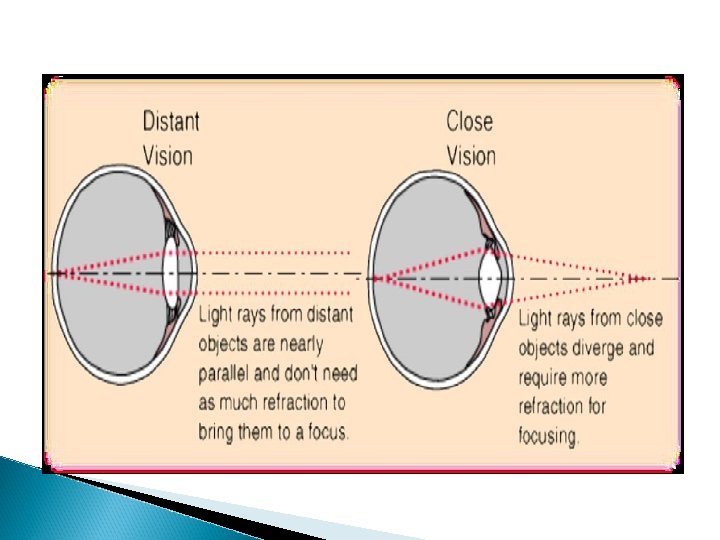
Pharmacodynamics of Ach v. Eye: ØMiosis: ØContraction of circular muscle of iris ØAccommodation to near vision: ØContraction of ciliary muscle of the eye ØDecrease IOP( intra-occular pressure) 3/3/2021 3
Pharmacodynamics of Ach v Exocrine glands & GI secretion: ØIncrease secretion v Contraction sphincters: of intestinal wall & relaxation of ØDefecation v Contraction of bladder wall & relaxation of sphincter: ØUrination 3/3/2021 4
Pharmacodynamics of Ach v Bronchi: ØBronchoconstriction ØIncrease mucosal secretion v Penile erection: ØIncrease release of nitric oxide 3/3/2021 5
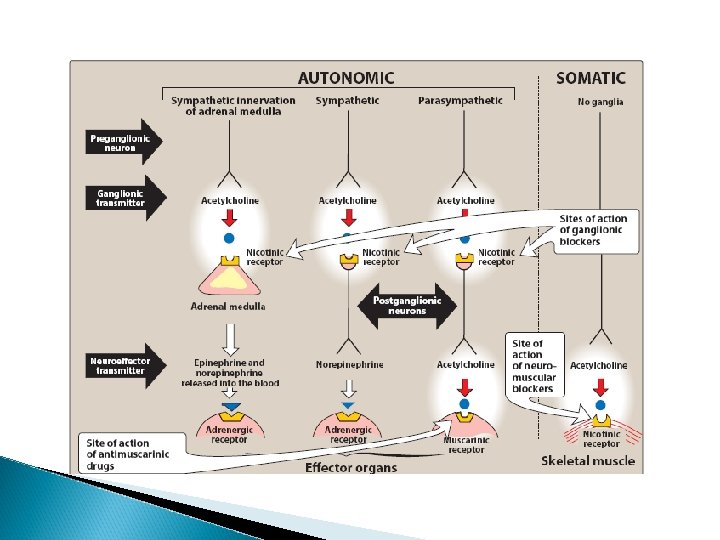
Pharmacodynamics of Ach q Nicotinic receptor stimulation: v Autonomic ganglia: ØStimulation v Adrenal medulla: ØIncrease noradrenaline & adrenaline secretion v NM Junction transmission: ØMuscle contraction 3/3/2021 6
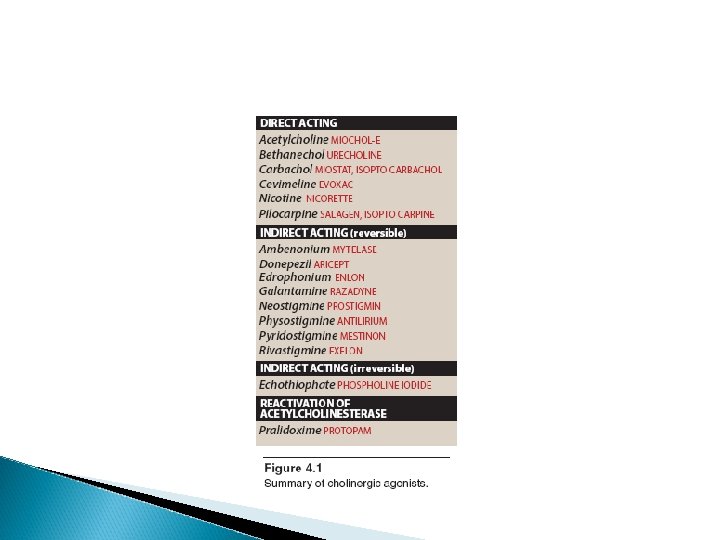
Cholinomimetics q. Mimic or simulate actions of Ach: v. Direct-acting v. Indirect-acting 3/3/2021 7
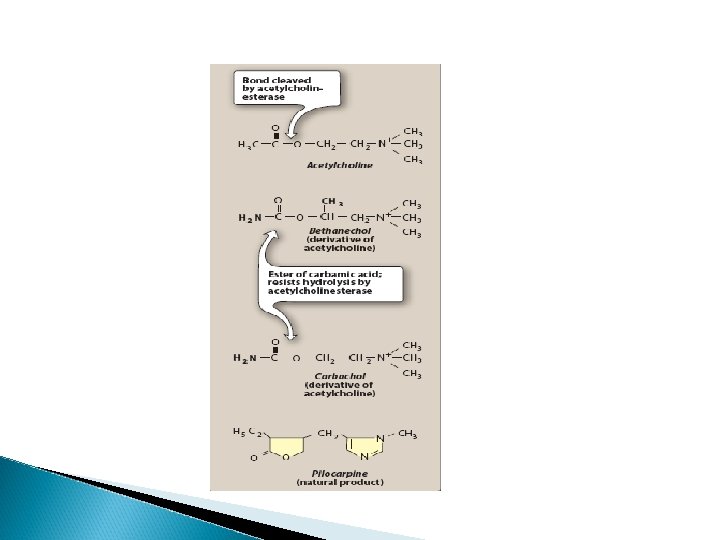
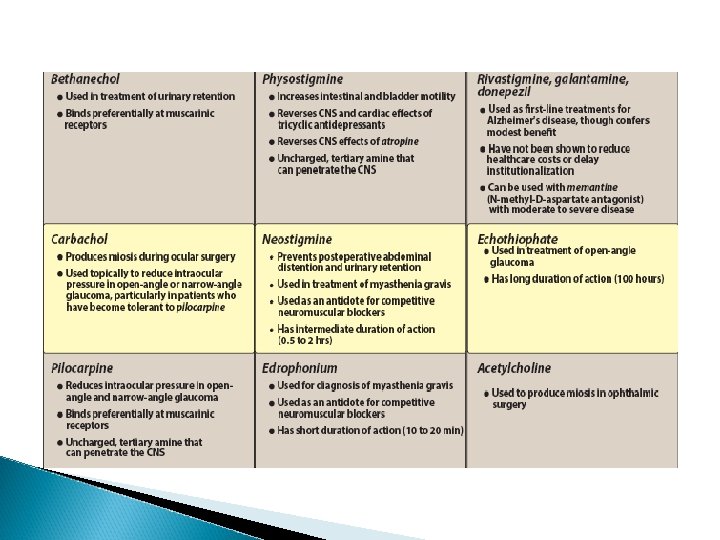
Direct acting cholinomimetics v. Activate directly cholinergic receptors: v. Choline esters: ØBethanechol, Carbachol, Methacholine ØResist degradation by cholinesterases ØHave longer duration of action than Ach v. Natural alkaloid: ØPilocarpine ØActs directly on end organs like the eye 3/3/2021 9
Bethanechol v Derivative of Ach v Has: ØLittle nicotinic effects ØGood muscarinic effects on bladder & GIT v Leads to easy urination & defecation v Used to treat post-operative or post-labour: ØUrinary retention or paralytic ileus: the weakness of intestine to or push its content causing constipation because of weak peristaltic activity 3/3/2021 13
Carbachol v Derivative of Ach v Has muscarinic & nicotinic actions v Limited use: ØBecause of nicotinic effects on ganglia & adrenal medulla v Used mainly topically as miotic in glaucoma to decrease high intraocular pressure (IOP) 3/3/2021 14
Pilocarpine v. Natural plant alkaloid v. Resistant to CE enzyme v. It produces: ØMiosis (contraction of circular muscle of iris) ØContraction of ciliary muscle of the eye ØReduction of IOP v. Used topically in glaucoma 3/3/2021 15
Pilocarpine v Lowers high IOP in close-angle & open angle chronic glaucoma v Improves outflow of aqueous humour: ØOpens fluid pathway ØIncrease aqueous flow through canal of Schlemm ØSecondary to contraction of circular muscle of the iris & ciliary muscle v Stimulates sweating, lacrimation, salivation 3/3/2021 16
3/3/2021 17
Indications of direct cholinomimetics v Paralytic ileus (Bethanechol) v Urinary retention (Bethanechol) v Glaucoma (Pilocarpine & Carbachol topically v Xerostomia (dry mouth) of Sjogren’s syndrome (oral pilocarpine) 3/3/2021 19
Adverse effects of direct cholinomimetics v Excessive sweating, salivation v Flushing, hypotension v Abdominal colic & diarrhoea v Bronchospasm v Pilocarpine: ØImpaired accommodation to far vision & darkness 3/3/2021 21
Contraindications of cholinomimetics v Bronchial asthma v Peptic ulcer 3/3/2021 22
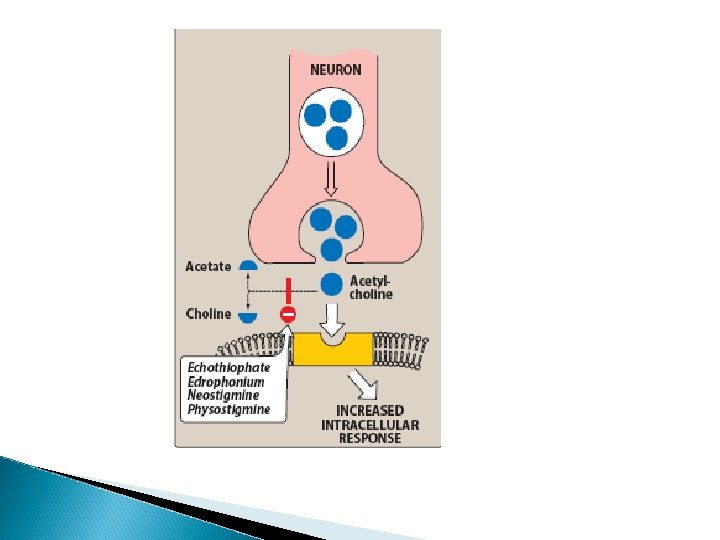
Cholinesterase enzymes v CE is a protein ØIn cholinergic synapses & RBC ØMetabolizes Ach into choline & acetate ØSpecific for Ach in cholinergic synapses v Pseudocholinesterase in plasma & liver ØNot specific to Ach ØMetabolizes other drugs (suxamethonium, procaine) 23
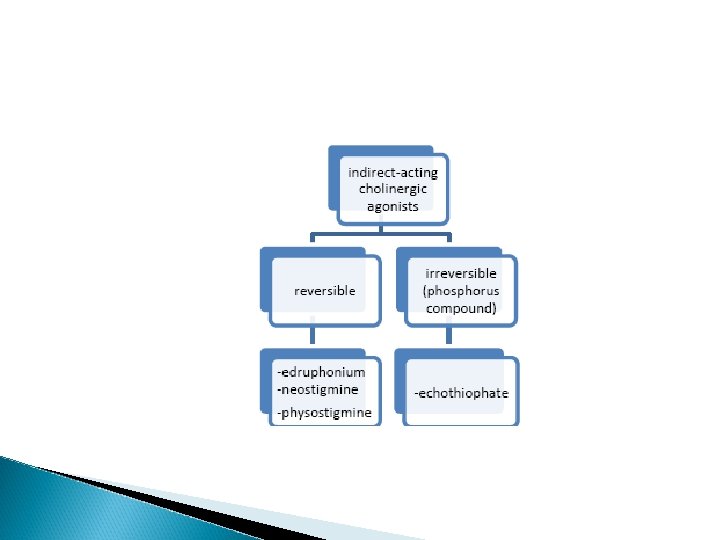
Classification of indirect-acting cholinomimetics Classified into: v Reversible cholinesterase inhibitors v Irreversible cholinesterase inhibitors 24
Uses of indirect-acting cholinomimetics v Diagnosis of MG (Edrophonium) v Treatment of MG (Pyridostigmine) v Reversible NMB intoxication (Neostigmine) v Alzheimer’s disease (Donepezil) v Irreversible CEI: insecticides 25
Myasthenia gravis (MG) v Autoimmune (autoantibodies to NM in NMJ) v Reduction in receptor number v Muscle weakness, fatigability, , difficult speaking & swallowing v Treatment: ØReversible CEI ØThymectomy ØImmunosuppressant 26
Reversible Ch. E inhibitors v Inhibit reversibly CE enzyme v Accumulation of Ach v Electrostatic bonds v Stimulate nicotinic & muscarinic receptors v Useful in myasthenia gravis 27
Neostigmine v Synthetic CEI, does not cross BBB v Duration of action (4 hrs) v Mainly in MG & also in: ØAntidote to competitive NM blocker tubocurarine poisoning ØParalytic ileus, urinary retention v Given orally, SC 28
Pyridostigmine v Similar to neostigmine v Has longer duration of action (6 hrs) v Useful orally in myasthenia gravis 29
Cholinergic Crisis: Over-stimulating of nicotinic receptors can cause muscle weakness and paralysis by the excessive intake of. Anticholinesterases which are (indirect drugs) Over-stimulation of nicotinic receptors will lead to its blockage instead of further activation. Cholinergic crisis can happen to myasthenia gravis patients who are overdosing on anticholinesterases drugs.
Edrophonium v Similar to neostigmine v IV, short duration of action (10 -20 min) v Useful in diagnosis of MG v To differentiate between weakness due to myasthenic crisis or cholinergic crisis: ØMyasthenic crisis improvement ØCholinergic crisis aggravated 31
Adverse effects of CEI v Excessive salivation v Flushing and hypotension v Abdominal colic and diarrhoea v Bronchospasm 32
CEI useful in Alzheimer’s disease v Tacrine q. Reversible CEI used in treatment of Alzheimer’s disease; qhepatotoxic v Donepezil ØNew selective CEI ØOnce daily ØLacks hepatoxicity of tacrine ØUseful in Alzheimer’s disease 33
Irreversible CE Inhibitors v Organophosphorous compounds v Irreversibly inhibit CE v Covalent bond in Enzyme-inhibitor complex v Used as insecticides: ØParathion, malathion v As nerve gases in chemical warfare: ØTabun, Sarin, Soman 34
Isoflurophate (DFP) v OP compound v Irreversibly inhibits CE v Insecticide v Toxicity: excessive cholinergic stimulation v May be used topically in glaucoma v Duration of action about a week 35
Echothiophate v New agent v Similar to isoflurophate v Long duration of action (week) 36
Differences between direct & indirect-acting cholinomimrtics v Actions on receptors: ØDirect ØIndirect v Pharmacodynamic effects: ØSimilar v Central effects with indirect: ØCross BBB 37
Organophosphorous Insecticide Poisoning v. Agricultural or industrial accidents v. Excessive cholinergic manifestations v. GIT (diarrhoea, colic) v. Respiratory (dyspnoea, bronchospam) v. CV (bradycardia, hypotension) v. Micturition, excessive sweating, M. paralysis v. Miosis (pin-point pupil), convulsions & death 38
Treatment of OPI Poisoning v General measures v High doses atropine IV or IM v Mechanical ventilation v Diazepam for convulsions v Enzyme reactivation by pralidoxime IM 39
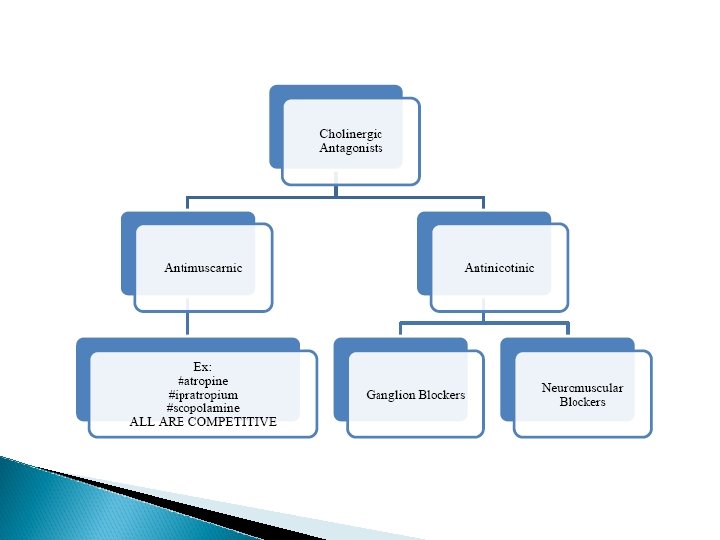
Cholinergic Antagonist Drugs a) b) Anti-muscarinic drug: Atropine-like drugs, Hyoscine (Scopolamine) Anti-nicotinic drugs Ganglion blockers: Used in experimental pharmacology. E. g. Nicotine, Trimethapan. Neuro-muscular blockers: Used in surgery to produce complete muscle relaxation.
Anti-muscarinic anti-cholinergic drugs q • q • Natural agents: Atropine, Hyoscine Semi-synthetic Homatropine Synthetic Ipratropium, Pirenzepine, Propantheline
Anti-muscarinic q Atropine (Hyoscyamine) • Alkaloids obtained from Atropa Belladona, Considered as prototype for parasympatolytics q Hyoscine (Scopolamine) • • Obtained from Hyocyamus niger plant (Datura Stramonium) Note: Antihistamines, phenothiazides and some antidepressants have antimuscarinic effects
Clinical pharmacology of antimuscarinic drugs Mechanism of action: Reversible blockade of M receptors Exocrine glands are most sensitive Gastric secretion is the least affected Heart is intermediate Note: Atropine blocks all 3 subtypes receptors (M 1, M 2, M 3)
Pharmacokinetics Absorption: § Natural and most tertiary amines: good § Wide distribution and cross BBB § Quaternary amines: poorly absorbed and poor crossing BBB (Ipratropium) q Atropine t½: 2 hrs q Partly metabolized and partly excreted unchanged q
Pharmacodynamics q Exocrine • • • glands: at low doses reduced secretions Salivary Bronchial Sweet glands
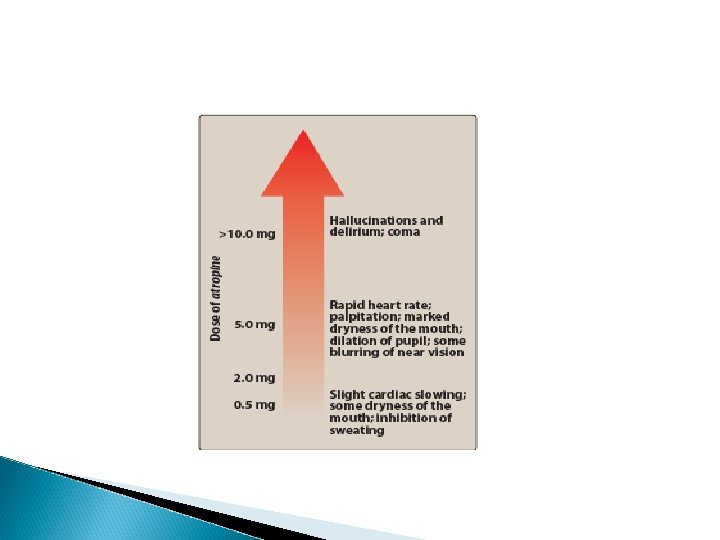
CNS Central stimulant effects (Atropine) Some may produce sedation (Hyoscine) Hyoscine blocks M receptors in vomiting centre and has anti-emetic effect Toxic doses: hallucination, convulsion, coma
Eye §Mydriasis (dilatation of pupil) §Cycloplegia (relaxation of the ciliary muscle) cause: blurred vision and impaired accommodation to near vision §Decreased lacrimation §Increase IOP
CVS Depending in the doses Central effect: § Decrease heart rate Peripheral effect: § Blockade of vagus nerve and increase heart rate ABP: § No change
Respiratory system Bronchodilatation Reduced bronchial secretion Ipratropium (quaternary amine derivate of Atropine) inhalation: ◦ Useful in asthma and chronic obstructive pulmonary disease (COPD), also in patient who are unable to take adrenergic agonists.
GIT Decrease salivation Decrease acid secretion Decrease motility Delay gastric emptying Prolong intestinal transit time Anti-diarrhoeal and anti-spasmodic effects
GUT Relaxation of bladder wall Useful in inflammatory spasm and pains of the urinary tract Risky in patients with BPH (Benign Prostatic Hypertrophy)
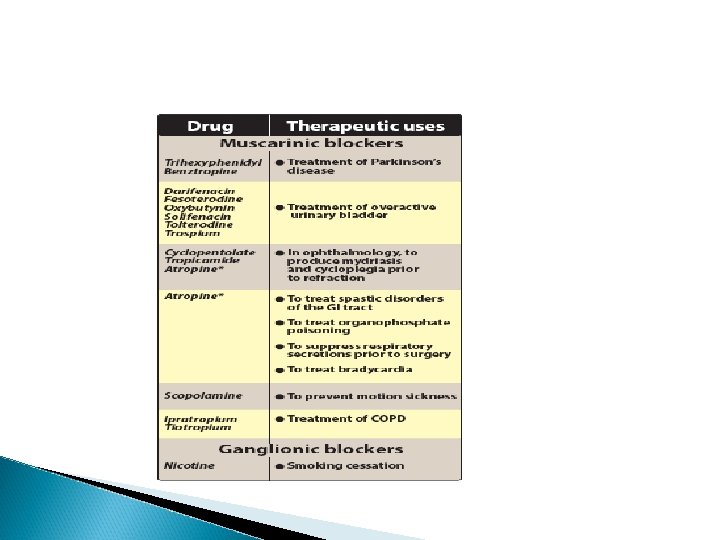
Therapeutic uses CNS disorders: Parkinson’s disease Drug-induced parkinsonism as Phenothiazine (induced acute dystonias: sustained contraction of muscles leading to twisting, distorted postures) Benztropine, Benzhexol: useful Motion sickness: Hyoscine oral, injection, transdermal patches
Therapeutic uses Ocular uses: In eye examination (Tropicamide) produce mydriasis and cycloplegia In iritis (Atropine eye drop) prevent synechia (adhesion of the iris to the lens) Note: Atropine eye drops effects: 7 days Tropicamide eye drops effects: 4 -12 hrs
Therapeutic uses Premedication: Hyoscine and Atropine (use as adjunct in anaesthetic procedure) Bronchial asthma: Ipratropium inh. (produce bronchodilatation) Cardiovascular: Bradycardia and heart block Atropine following AMI:
Therapeutic uses GI disorders: Anti-diarrhoeal • Lomotil= atropine + diphenoxylate Anti-spasmodics (in intestinal colic, irritable bowel syndrome) • Atropine, hyoscine, clidinium, prifinium. Urinary disorders: Urinary urgency with UTI Renal colic
Therapeutic uses Cholinergic poisoning as: • Irreversible CEI insecticide poisoning • Chemical warfare intoxication. To counteract muscarinic effects (nicotinic effects can not be reversed) Atropine IV
Adverse effects of antimuscarinic agents Dry mouth Blurred vision Tachycardia Constipation Hot flushed dry skin & hyperthermia may occur with high doses
Contraindications q Glaucoma • Increase IOP q BPH • Bladder wall relaxation & sphincter contraction
Atropine poisoning Hot flushed dry skin & hyperthermia, Agitation, delirium, hallucination, Convulsions & coma Treatment is symptomatic
Individual drugs Atropine Hyoscine • Buscopan Clidinium • Libraxam Prifinium • Riabal
Neuromuscular blockers q Nondepolarizing (competitive) blockers The first drug known to block the skeletal NMJ was curare. Neuromuscular blockers are clinically useful during surgery to facilitate tracheal intubation and provide complete muscle relaxation at lower anesthetic doses, allowing for more rapid recovery from anesthesia and reducing postoperative respiratory depression.
Neuromuscular blockers Depolarizing agents Depolarizing blocking agents work by depolarizing the plasma membrane of the muscle fiber, similar to the action of ACh.