Abnormal uterine bleeding Characteristics of normal and abnormal

Abnormal uterine bleeding

Characteristics of normal and abnormal menstruation: Normally the menstrual cycle occurs at each 28 days (the normal range is 21 to 35 days) and lasting for average 5 days (the normal range is 2 to 8 days) and the average loss of blood in each cycle is 40 ml (the normal range 20 -80 ml).
 this AUB")
�So any alteration in this normal pattern will be regard as (AUB) this AUB is a symptom, not a disease and it occur in various forms:

Menorrhagia: is a cyclic bleeding at normal interval, but it is excessive in amount (>80 ml) and /or duration (>8 days). (excessive bleeding at regular interval over several consecutive cycle ).
 is cyclic bleeding which is normal in amount but occurs at")
Polymenorrhea: (frequent cycle) is cyclic bleeding which is normal in amount but occurs at too frequent interval (<21 days).
. is a regular cycle but occur at intervals of >35")
Oligomenorrhea: ( infrequent cycle). is a regular cycle but occur at intervals of >35 days

Metorrhagia: uterine bleeding occurring at completely irregular but frequent intervals, the amount being variable. Menometorrhagia: uterine bleeding that is prolonged AND occurs at completely irregular intervals(heavy loss). .

Intermenstrual bleeding: bleeding of variable amounts occurring between regular menstrual periods.

22 years old female � presented to you with history of iregular vaginal bleeding for 3 month ago

What are the causes � What are the point in history you should ask about it
Organic cause local systemic pregnancy related Complications.")
A)Organic cause local systemic pregnancy related Complications.
")
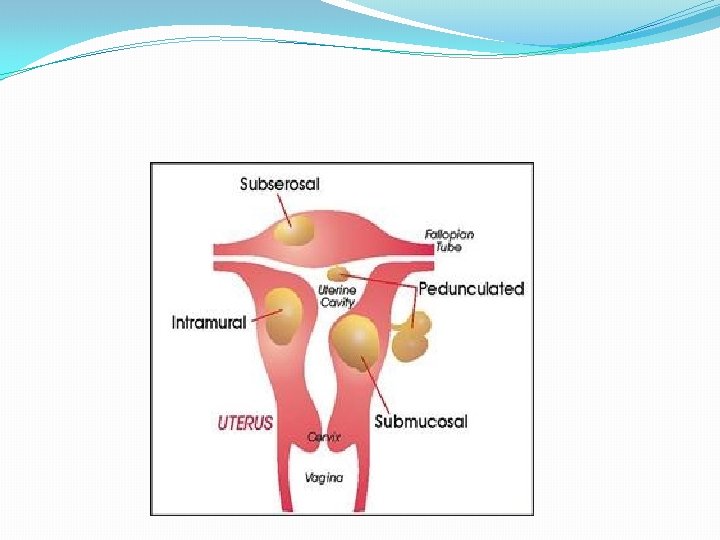
Benign pelvic lesions Leiomyomata Endometrial or endocervical polyps Adenomyosis and endometriosis Pelvic infections (PID) Intrauterine contraceptive device (IUCD) Trauma Foreign bodies (IUD, sanitary products)

Malignant pelvic lesions Endometrial hyperplasia Endometrial cancer Cervical cancer Less frequently: vaginal, vulvar, fallopian tube cancers estrogen secreting ovarian tumors granulosatheca cell tumors

Systemic disorder Endocrine disorder: include hypothyroidism, hyperthyroidism, , DM, adrenal disease and prolactine disorders. These may interfere with the normal feed back mechanism of the hypothalamic – pituitary –ovarian axis.
 e. g von willebrand s disease and")
Hematological disorders : ( especially in teenagers) e. g von willebrand s disease and idiopathic thrombocytopenic purpura, leukemia. Liver disorders: may interfere with metabolism of estrogen. Also they decrease coagulation factors production by liver.

Renal disease: may alter the excretion of estrogen and progesterone. Medications: such as steroid hormones, neuroleptics, anticoagulants and cytotoxic agents. Emotional stress and psychological upset: these may affect the hypothalamus and the higher centers.

pregnancy complications These are the most common cause of AUB in females of 20 -40 years age. These include ectopic pregnancy, miscarriage and gestational trophoblastic disease.

How many type of clinical presentation that pt may present to you (according to the age) � The incidence of organic disease & the prognosis of DUB vary with the amount &type of bleeding & the patient age.
 F. B vulvovagintis rarely")
By age group. Pre-menarche Always abnormal: most common trauma(sexual abuse) F. B vulvovagintis rarely precocious pueperty neoplasm.

Adolescents&teenager AUB in adolescent girls is almost always dysfunctional(80% have an-ovulatory cycle in the first few years), rarely organic diseases like pregnancy, infection, hematological problem need to be exclude before considered an-ovulation. malignancy is very rare.

In severe & persistent abnormal bleeding, bleeding disorders must be excluded. The treatment is always medical& conservative.

Adult AUB between the ages 20 -39 years is most commonly due to benign disease of the genital tract like PID, fibroid, or some complications of pregnancy. Though DUB is also common. Organic disease must therefore always be excluded before the diagnosis of DUB is made.

�Conservative therapy is usually indicated, hysterectomy may be indicated if bleeding is severe or recurrent & the patient had completed here family.

Perimenopausal women. AUB in women age 40 years or more is most commonly dysfunctional in origin though organic disease is also common. carcinoma of the cervix. &ca. of the endometrium occur with increasing age so it is important to exclude these conditions in all cases of perimenopausal bleeding.

How you evaluate her History: Age, menstrual pattern, sexual activity, trauma, infection, systemic disease, stress history of bleeding tendency, hormonal therapy or IUD

Examination: General: Hirsutism, acne, galactorrhea, thyroid enlargement, bruising Abdominal: Pelvic&abdominal swelling, liver, spleen Pelvic: infections, lesions, lacerations, polyps, fibroids

TV U/S 6 -Transvaginal ultrasound to detect any pelvic pathology and to assess the thickness of the endometrium especially in postmenopausal women ( < 5 mm, endometrial cancer is unlikely)

What you are the investigation you will send her 1 -CBC(should be send for all the patient) 2 -β-HCG 3 - cervical cultures 4 - PAP smear 5 -Hormonal assay(TSH, prolactin, estradiol, progesterone, D-HEAS, testosterone) are not routinely send , only when there is clinical suspicion of endocrine abnormality.

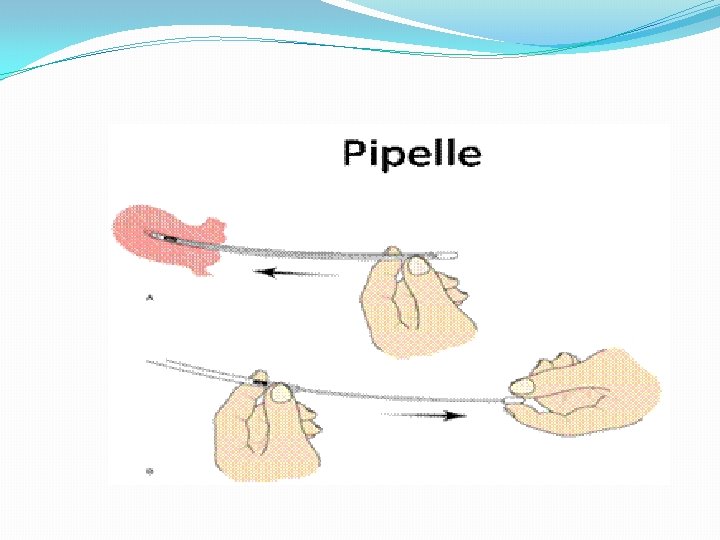
7 -Endometrial sampling It is recommended in the evaluation of AUB in: 1. Woman aged > 40 years 2. Those with high risk for endom. ca (obesity, hypertension, diabetes, chronic an ovulation, nulliparity with history of infertility, family history of colonic& endom. ca & tamoxifen therapy. 3. In younger woman it is indicated when the AUB doesn't resolved with medical treatment or when inter menstrual bleeding persist.
.")
The most common methods for endom. sampling are: 1. Aspiration curettage (pipelle, vabra, sharman). 2. D&C. 3. Hysteroscopy.

hysteroscope

what are line of treatmet : when an organic cause is detected treatment is directed to it, e. g. : Fibroids: Gn. RH agonists, myomectomy or hysterectomy
 Endometrial polyps: curettage Endometrial carcinoma: TAH")
Adenomyosis: Hysterectomy or medical (progestins, Gn. RH analogues) Endometrial polyps: curettage Endometrial carcinoma: TAH + BSO +/- radiation
")
N. B. When an organic cause can not be detected, it is considered (DUB) Medical management of dysfunctional uterine bleeding include: A. NON HORMONAL

First line treatment in primary care. Using either NSAID or antifibrinolytic . both can be used, referral considered if neither the above drugs were effective: after 3 months
: Tablets consistently taken during menses Mefenamic acid 500")
Non steroidal anti‑inflammatory drugs (NSAIDs): Tablets consistently taken during menses Mefenamic acid 500 mg tds, Naproxyn 250 mg tds , Ibuprofen 400 mg 4 times daily Dysmenorrhea and other menstrual symptoms may improve
![3] Antifibrinolytic drugs: (tranexamic Medical treatment of DUB (cont) acid) Taken first 4 days](http://slidetodoc.com/presentation_image_h/3325a7affa8937406625b275089c1d83/image-42.jpg "3] Antifibrinolytic drugs: (tranexamic Medical treatment of DUB (cont) acid) Taken first 4 days")
3] Antifibrinolytic drugs: (tranexamic Medical treatment of DUB (cont) acid) Taken first 4 days of cycle Tranexamic acid 2 -4. 5 g times daily
![6] Hormonal therapy of DUB: a) Progestins: Oral progestogens:](http://slidetodoc.com/presentation_image_h/3325a7affa8937406625b275089c1d83/image-43.jpg "6] Hormonal therapy of DUB: a) Progestins: Oral progestogens:")
6] Hormonal therapy of DUB: a) Progestins: Oral progestogens:
 releasing IUD: The new progestrone medicated IUCD (Mirena) delivers 20 Mg of")
Levonorgestrel (LNG) releasing IUD: The new progestrone medicated IUCD (Mirena) delivers 20 Mg of levonorgesrel over 24 hours for about 5 years. It reduced MBL up to 96 and 20% reported to be amenorrheic after 1 year. It is potential alternative to surgery.

Intramuscular Progestogen: - Depot medroxy progesterone acetate Produces amenorrhea or slight bleeding - Sometimes prolonged bleeding or spotting - Unpredictable delay in return of fertility
 b ) Estrogens: - Given in acute heavy")
Hormonal therapy of DUB (cont. ) b ) Estrogens: - Given in acute heavy bleeding - Conjugated oestrogen – 25 mg IV 4 hourly until bleeding stops (not >6 doses)
: �c) For woman requiring contraception or")
Estrogen + Progestin ( combined oral contraceptive pill): �c) For woman requiring contraception or for whom hormonal agents are acceptable (COCP) are effective in decreasing MBL, cycle regulation, relieving dysmenorrhea. For non smokers, non obese& in the absence of cardiovascular risk no upper limit of age for the treatment of menorrhagia.

Data regarding the use of hormone replacement therapy are scant. Effective if the bleeding is not severe Minor side-effects MBL reduction 50% 70 -80% patients benefit Few minor side-effects
 Androgens: Danazol- Gestrinone - Danazol- Taken continuously - - Dosage: 200 mg daily;")
d) Androgens: Danazol- Gestrinone - Danazol- Taken continuously - - Dosage: 200 mg daily; - MBL reduction 90% over 3 months - - Expensive - Troublesome side-effects (Hypo-estrogenic & androgenic, muscle cramps, hot flushes)

- Gestrinon . dose 2. 5 mg twice a week for 12 weeks. Its also has androgenic side effects
 Gonadotropin releasing hormone analogues (Gn Rha): - Causes amenorrhea - Used in special")
e) Gonadotropin releasing hormone analogues (Gn Rha): - Causes amenorrhea - Used in special circumstances - Expensive - Troublesome side-effects (hypoestrogenic, bone loss, hot flushes, vaginal dryness) -
. Reviews show that it induced amenorrhea& decrease fibroid size, notable")
Anti-progestational agents. �Mifepristone(RU 486). Reviews show that it induced amenorrhea& decrease fibroid size, notable adverse effect is the development of endomometrial hyperplasia
 Surgical therapy of DUB: if medical therapy for 3‑ 6 months failed A)")
II) Surgical therapy of DUB: if medical therapy for 3‑ 6 months failed A) Dilatation and curettage: Arrest of the bleeding, if it is severe or persistent, particularly hyperplastic endometrium. Curettage is essentially a diagnostic & not a therapeutic procedure.
 Endometrial ablation techniques: Electrocautery, laser, cryoablation, or thermoablation Become an alternative to hysterectomy")
B) Endometrial ablation techniques: Electrocautery, laser, cryoablation, or thermoablation Become an alternative to hysterectomy for treatment of DUB. Any ablation technique should adequately destroy the basal layer of endometrium. Most women will not experience long term amenorrhea after treatment
 � C) Hysterectomy: is the final step Advantages:")
Surgical therapy of DUB (cont. ) � C) Hysterectomy: is the final step Advantages: 1‑ complete cure 2‑ Avoid medical treatment 3 - Remove any missed pathology

Disadvantages: 1 - Major operative procedure 2 - Long hospitalization 3 - Significant morbidity 4 - Long term sequel (pain ‑ urinary dysfunction ‑ sexual dysfunction)
Has little place in treatment of DUB. Used in Radiotherapy for treatment of DUB:")
III)Has little place in treatment of DUB. Used in Radiotherapy for treatment of DUB: patients in need for hysterectomy but unfit for operation. External irradiation of the ovaries is performed aresulting in amenorrhea in 95% of cases.
- Slides: 57