Abnormal Psychology Intro Pg 531 537 Abnormal Psych

Abnormal Psychology Intro Pg 531 -537
 manifest in people’s thoughts and behaviors. It’s difficult")
Abnormal Psych Ø Psych Disorders (D/O) manifest in people’s thoughts and behaviors. It’s difficult to determine what constitutes “abnormal. ” What’s the difference between odd, little quirks we all have and a legitimate mental illness? l l M – Maladaptive – makes it difficult to function – in work, school or relationships A – Atypical – most people don’t do it; unusual I – Irrational – there is no logical explanation for the behavior D – Disturbing – it is disturbing to self or others

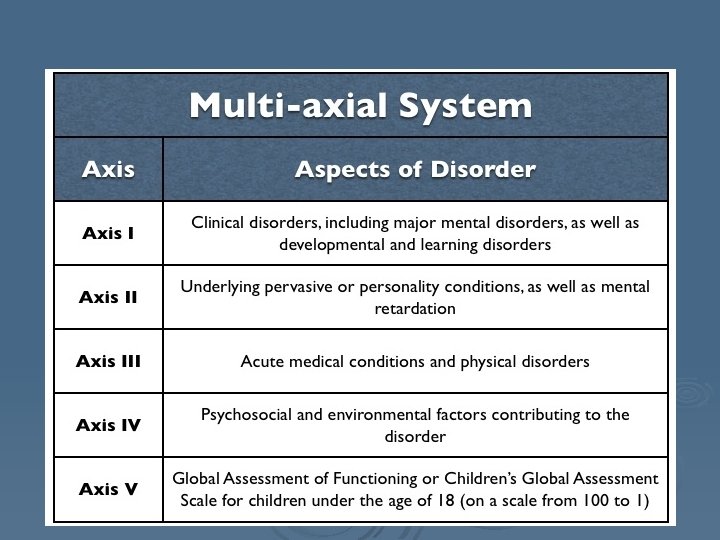
DSM - V How do we know when someone has a D/O? Ø Diagnostic Statistical Manual of Mental Disorders Ø l l Has hundreds of disorders Doesn’t discuss cause or treatment Only discusses symptoms for diagnosis/labeling Highly reliable (80%. . . what does this mean? )

David Rosenhan ØBeing Sane in Insane Places: Øhttps: //www. youtube. com/watch? v =D 8 Oxd. GV_7 lo Øhttps: //www. youtube. com/watch? v =j 6 bm. Z 8 c. VB 4 o ØWhat do YOU think of Rosenhan’s study?

Pros and Cons of Labeling Pros Cons Get help – you know what you have and can deal with it - meds, counseling, treatment Ø Insurance – once officially diagnosed, insurance will help cover costs Ø Reliability/consistency among professionals Ø Legal competence – “insanity” is a legal, not medical term Ø Self-fulfilling prophecy Ø Stigma – mistreated by society (? ) Ø l Ø David Rosenhan Study Always have label

Perspectives – Approach treatment differently Ø Psychoanalytic – childhood, fixation, unconscious Ø Humanistic – low self esteem, failure to reach potential, needs not being met Ø Behavioral – environment, conditioning, modeling Ø Cognitive – dysfunctional thoughts Ø Socio-cultural – dysfunctional culture, society Ø Biomedical/Physiological – chemical imbalance, gene, inherited

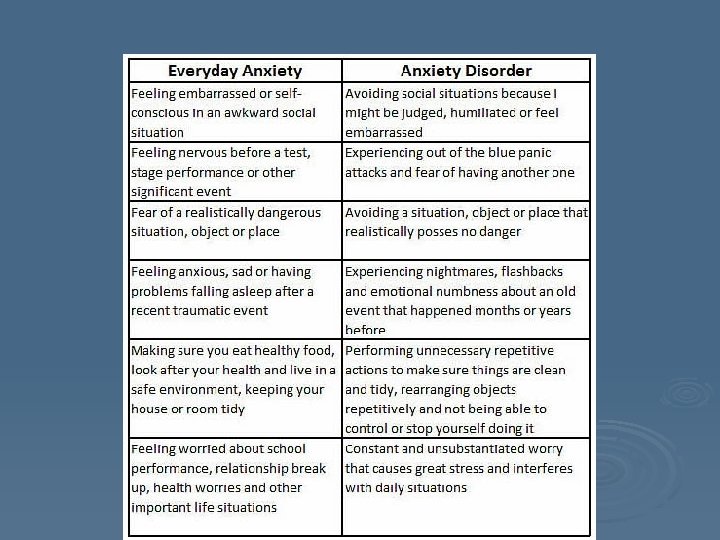
ANXIETY D/O All Anxiety D/O share the common symptom of anxiety. Abnormalities may be…. 1. ) Level of Anxiety – excessive 2. ) Irrational trigger for anxiety 3. ) Prolonged timing for anxiety

PANIC ATTACKS Acute episodes of intense anxiety without any apparent provocation (you feel like you are in a life or death emergency situation – but you are not) Ø Sympathetic NS kicks in Ø l l l Choking sensation Trembling Hyperventilating Distress Sweating or peaked

PHOBIAS Ø Intense unwarranted fear of a situation or object. Fear is way out of proportion to real danger. Some stimuli are easier to avoid and therefore less debilitating) l Claustrophobia – fear of small places, confinement l Arachnophobia – fear of spiders l l l Agoraphobia – fear of public places – may refuse to leave home and world becomes smaller and smaller Social Phobia – fear of embarrassing oneself in public Many phobias are created from a panic attack and classical conditioning (remember the story of my nephew and the elevator)

GENERALIZED ANXIETY D/0 Ø Ø Ø 6 months or more of unwarranted, excessive, constant, unrealistic worry Person always feels jittery, nervous, worried Unusual not in the level of anxiety but in the duration – i. e. symptoms are commonplace, persistence isn’t 2/3 sufferers are women Often associated with perfectionist personality l l l Insomnia Ulcers Irritable bowel Muscle aches Head aches

GAD Prevalence
 Ø Ø Ø Obsessions: persistent, recurring, disturbing, unwanted thoughts –")
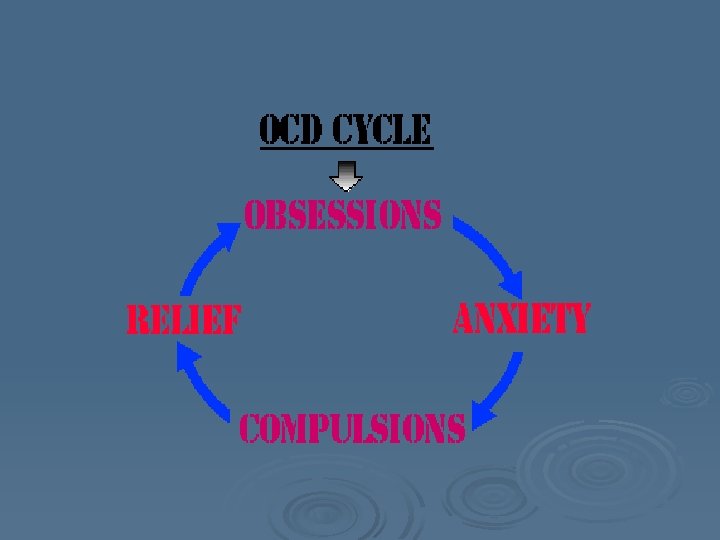
Obsessive Compulsive D/O (OCD) Ø Ø Ø Obsessions: persistent, recurring, disturbing, unwanted thoughts – cause extreme anx Compulsions: ritual or routine that relieves the anx temporarily (compulsions are negative reinforcement – removes/reduces anx temporarily) Most with OCD realize their obsessions are irrational and their compulsions are unnecessary, but cannot stop Prevalence @ 3% of population Usually appears in late teens, early adulthood Men and women =

OCD – Common compulsions Ø Cleaning Ø Checking Ø Repeating Ø Hoarding Ø Compulsions can become extremely maladaptive and interfere with normal functioning (school, work, relationships)

Post Traumatic Stress D/O PTSD Ø Flashbacks/nightmares after a person’s involvement in a troubling or disturbing event Ø Relive the trauma Ø Experience extreme anx Ø Common for soldiers coming back from war

Theories of Cause - ANX Ø Psychoanalysis – unresolved uncon conflict, overactive superego Ø Behaviorist – classical conditioning (phobias), modeling (anx – likely had overly anxious, worrisome parents/environment) Ø Cognitive – dysfunctional thoughts, unrealistic expectations, fears Ø Biology/physiology – genetic predisposition l l Meds – anti-anxiety (depressants) Xanax, Valium
 Experience extreme or inappropriate emotions")
MOOD D/O (Affect D/O) Experience extreme or inappropriate emotions
 Ø")
Major Depression Ø “common cold” of psychology (highest prevalence of any mental illness) Ø 2 weeks of symptoms with no clear reason Ø Disrupts normal functioning Ø Symptoms – loss of appetite, fatigue, change in sleep patterns, lack of interest in previously enjoyable activities, feelings of worthlessness, hopelessness, tired/lethargic, suicidal thoughts Ø Women 2 X as likely as men Ø Rate of depression increased with each generation and diagnosed at earlier age

Suicide Ø Ø Ø 3 -1 suicide – homicide Women more likely to attempt, but men twice as likely to succeed…. why? Suicide rates higher among white, rich, nonreligious, single, widowed, divorced…. why? People seldom commit suicide while in depths of depression (lack energy and initiative). Suicide attempt actually more likely when person experience slight upswing from depths of depression TED talk Kevin Briggs – Bridge Between Suicide and Life: https: //www. ted. com/talks/kevin_briggs_the_bridge_be tween_suicide_and_life

 Ø Ø Ø 1% of population Men and women = Extreme")
Manic Depression (Bipolar) Ø Ø Ø 1% of population Men and women = Extreme mood swings Depression – looks like major depression Mania – high energy, racing thoughts, grandiose ideas, soaring confidence, sense of invincibility, risky behaviors Link between MD and creativity/genius?

Manic Depression

Manic Depression Ø Treatment – lithium Left untreated – symptoms get worse and mood swings get more dramatic Ø Fires of Mind – Manic Depression https: //www. youtube. com/ watch? v=Ki 6 QOf. Zf. CSk Ø
 Depression during winter months – cold, dark Ø Normal depression")
Seasonal Affect D/O (SAD) Depression during winter months – cold, dark Ø Normal depression symptoms that follow seasonal patterns Ø Almost non-existent in ward, sunny climates Ø Treated with special light bulbs Ø

SAD

Causes of Mood D/O Ø Psychoanalytic – uncon conflict, over powerful superego Ø Behaviorist – social modeling; reinforcement/attention Ø Biology – lower levels of serotonin cause depression anti-depressants – increase serotonin levels by blocking reuptake Ex: Zoloft or Prozac l

Causes of Mood D/O - Cognitive Ø Aaron Beck – depression results from unreasonable thoughts about your cognitive triad – yourself, your world, and your future

Causes of Mood D/O – Cognitive – Attribution Style Failures Successes Ø Internal – I suck Ø External – I got lucky Ø Global – I suck at everything Ø Stable suck – I’ll always Ø Specific – on just this one test Ø Unstable last – it won’t

Causes of Mood D/O Cognitive Learned Helplessness Martin Seligman Prior experiences cause person to believe they are unable to control aspects of their future that are indeed controllable Ø When undesirable things occur person feels unable to improve situation Ø Leads to passivity and depression Ø

Learned Helplessness

Schizophrenia One of more severe and debilitating mental D/O

ØAnderson Cooper CNN – Schizophrenia simulation Øhttps: //www. youtube. com/watch? v =y. L 9 UJVtg. PZY

Schizophrenia Ø Schism – literally means a split mind or break from reality (NOT multiple personality) Ø Surfaces in young adulthood Ø Exists in 1% of population – strong genetic component Ø Nature/Nurture at work

Schizophrenia - Symptoms Ø Delusions – beliefs with absolutely no basis in reality. Cannot be corrected with logic Delusions of Grandeur – possess great power or influence l l Delusions of Persecution – people out to get you – makes schizophrenia very difficult to treat – don’t trust anyone, don’t take meds

Schizophrenia - Symptoms Ø Hallucinations – False sensory perceptions (you see or hear things that are not really there) l Auditory Hallucinations most common – hear voices l Inappropriate Language • Word Salad • Neologisms • Clang Associations

Schizophrenia - Symptoms Ø Catatonia – catatonic state Ø Inappropriate Emotion – laugh at something sad, cry at something funny l Flat Affect – no emotion

Schizophrenia - Symptoms Positive – addition of atypical behaviors Negative – subtraction of normal behaviors Ø Delusions Ø Flat Affect Ø Hallucinations Ø Inappropriate Emotion Ø Inappropriate Language

Causes – Biological/Nature Ø Dopamine hypothesis – higher levels of Dop Anti-psychotic drugs act as antagonists for dopamine – they block receptor sites to lower dopamine levels Ø Haldol/Thorazine Ø Help control + symptoms of hallucinations and delusions Ø Side effects – muscle stiffness/tremors, weight gain, slow cognitive functioning Ø

Causes – Biological/Nature Ø Brain abnormalities – schizophrenics have large ventricles and more brain asymmetry Ø Family prevalence l l l 1% general prevalence 10% if parent is schizo 45% if both parents Almost 50% identical twin How do you know it’s not ALL nature? ? ?

Schizophrenia – Nature/Nurture Ø 1 st Hit = genetics Ø 2 nd Hit – Nurture/Environment l l l Viruses Drugs Brain trauma Stress Etc…….

Personality D/O Well established, maladaptive ways of behaving that negatively affect people’s ability to function. Personality D/O are less maladaptive than other mental illnesses– may function in school or work but typically strain close, long-term relationships.

Narcissism Ø Extreme selfishness – cannot see others’ perspective Ø Difficulty with empathy Ø Entitlement Ø Need for adoration – power Ø Fantasy of beauty or ideal love Ø Exaggerates talents/accomplishments to appear superior Ø Manipulation/exploitation of others

Anti-Social Personality D/O Ø Disregard for safety of self or others Ø Lack of remorse/guilt – lack moral conscience Ø Deception – lie easily Ø Risky impulsive behavior Ø No empathy – little regard for others’ feelings Ø Disregard societal rules/authority Ø Aggressive or violent behavior Ø Unable to maintain close relationships

Anti-Social Personality D/O Ø More prevalent among males Ø High incidence in criminal/incarcerated population Ø Must be 18 to get diagnosis Ø Teen boy exhibiting same symptoms = Conduct Disorder Not all ASPD become serial killers but all serial killers are ASPD

Dependent Personality D/O Ø See self as helpless/incompetent; lack confidence Ø Look to others to take the lead, make decisions, or provide support Ø Inability to make decisions – even common, every day ones Ø Overly sensitive to criticism Ø Fear being alone – stay in bad/abusive relationships, go from one relationship to another Ø Avoid disagreeing with others – fear conflict

Histrionic Personality D/O Ø Overly dramatic – as if performing for others Ø Display of excessive emotions and yet seems shallow/fake Ø Need for attention Ø Dresses provocatively, excessive flirt Ø Overly concerned with physical appearance Ø Needs constant approval/reassurance Ø Easily swayed of influenced by others

Personality D/O – Causes/Treatment Often caused by family dynamics, parenting styles Ø Deeply ingrained, chronic habits Ø Stronger basis in Nurture/Environment Ø Difficult to treat Ø l l Often no magic medicine Person themselves rarely sees that they have a problem Often able to function at work or school Greatest fall-out is in close, long-term relationships – family, marriage

Somatoform D/O Patient manifests with a physical problem but there is no physiological cause – underlying cause is psychological

Hypochondriasis Ø Physical complaints with no physiological cause Ø Chronic Ø Often feel poorly, sick Ø Absent from work/school Ø Always convinced have illness

Conversion D/O ØAcute ØWake up blind or partially paralyzed ØTest after test reveals no physiological cause

Dissociative D/O Involve dysfunction of memory or altered sense of identity

Ø Psychogenic l l Amnesia - no biological cause Cannot remember things Periods of time blacked out Unfamiliar with environment May be brought on by traumatic event Psychogenic Fugue – sudden and complete loss of identity Caused by severe stress Assume new identity – leave home, find new identity elsewhere
 Ø Multiple l l l l l Personality Appearance of")
Dissociative Identity D/O (DID) Ø Multiple l l l l l Personality Appearance of 2 + distinct identities in one person Identities may or may not be aware of each other Identities may vary in age, gender, handedness Much more common in women Often from severely traumatic, abusive or neglectful environment Difficult to treat – extensive, long term therapy Some Psychologists question if it is a real D/O Often confused with schizophrenia – NOT same thing – Oprah Clip – DID patient https: //www. youtube. com/watch? v=n 2 atzoa. A 2 NI

DID

Remember other D/O Ø Sexual l Fetishes, pedophilia, zoophilia Voyeurs Sadists/Masochists Ø Eating l l D/O Anorexia Bulimia Ø Substance Abuse – Alcohol, Drugs Ø Developmental D/O l Autism, ADD/ADHD (both higher in boys)

Commonalities of all D/O? ? Ø MAID Ø Stress - makes D/O surface or makes it worse Ø Most a combo of nature/nurture Ø Many surface in young adulthood (late teens, early 20 s) Ø Strain on families Ø Difficulty finding right medicine, right dosage, and almost always unwanted side effects

D/O and Gender Skews Males Females Ø Alcohol/drug abuse Ø Depression Ø ADD/ADHD Ø Generalized Anxiety Ø Anti-social or conduct D/O Ø DID Ø Autism Ø Anorexia or Bulimia Ø ADD/ADHD
- Slides: 68