ABNORMAL FUNCTION OF STOMATOGNATHIC SYSTEM Part3 ABNORMAL FUNCTION

ABNORMAL FUNCTION OF STOMATOGNATHIC SYSTEM Part-3
 Mouth breathing � If the palate is high")
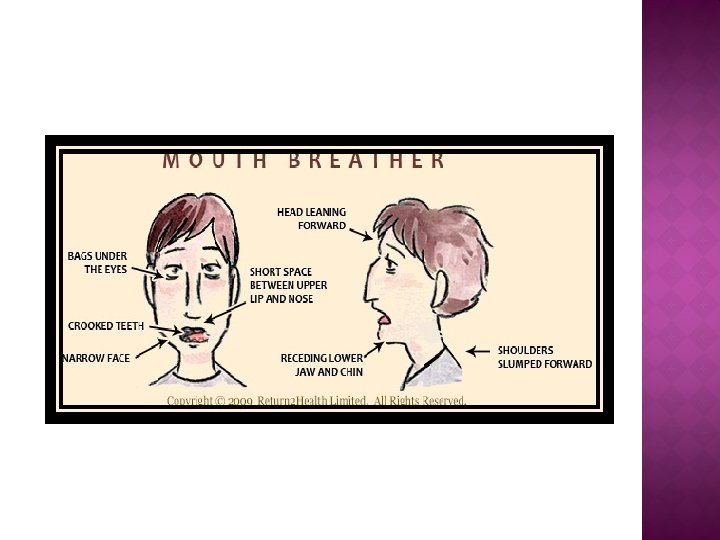
ABNORMAL FUNCTION OF STOMATOGNATHIC SYSTEM 1) Mouth breathing � If the palate is high and narrow, the dorsum of tongue does not fit against the palatal vault every where and a potential away exist between tongue and palate. � If in addition, lips do not meet, the oral airway is complete from open lips to the oro-pharynx. So air can be drawn in and expired just as easily through mouth cavity as through nasal cavities. � Mouth breathing is more commonly seen in children and decreases with age. Also more common during sleeping.

Classification Obstructive Habitual Anatomical • Seen in adenoid facies. • increased resistance to or a complete obstruction of the normal flow of air thorough nasal passages • A child who continuously breathes through his mouth by force of habit, although the abnormal obstruction has been removed. • Whose shorter upper lip does not permit closure without under efforts.
 Naso-pharyngeal obstruction • Nasal deformities – DNS • Irritation or thickening of")
Etiology ) Naso-pharyngeal obstruction • Nasal deformities – DNS • Irritation or thickening of mucosal membrane of nose • Bone pathology • Enlarged adenoids. Mouth habits • Thumb sucking • lip biting, • finger or nail biting, • tongue thrusting Abnormal development • Macro-glossia • Short upper lip Psychosomatic problems • May also show mouth breathing

Effects of mouth breathing Tongue position is low and forward to keep oral airway open. Gingivitis and increased dental caries Labial flaring of maxillary anterior teeth. Frequently marked overbite Hyper trophy of lower lips Dryness of mouth Affected gingiva is demarked from unaffected gingiva, the junction has been referred by ‘Worwick’ as tension ridge.
 Bruxism � A conscious or subconcious act. � overrides the protective neurologic mechanism")
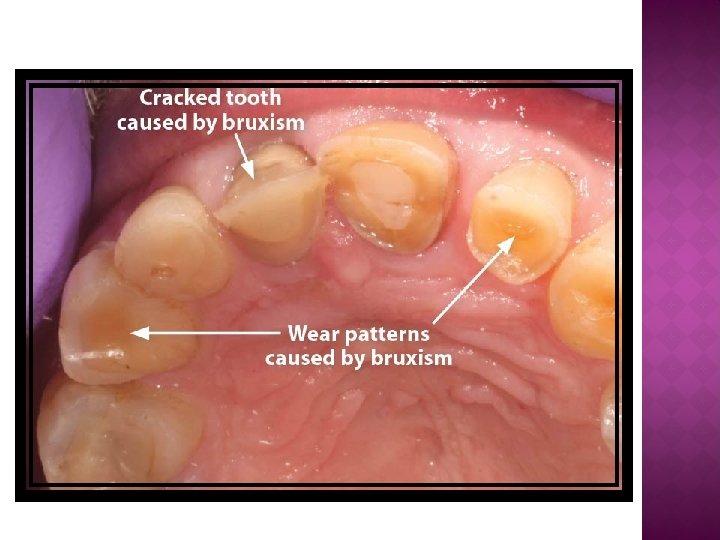
2) Bruxism � A conscious or subconcious act. � overrides the protective neurologic mechanism of masticatory system. � Increase in tonic activity in the jaw muscles. � Emotional or nervous tension, pain or discomfort and occlusal interferences are the factors that can increase muscle tonus and lead to non-functional clenching. Effects TMJ pain • Tenderness of masticatory muscle Incisal wear, • occlusal facets headache • tiredness of masticatory muscles.
 Psychic tension � Nervous children may develop bruxism 2) Occlusal discrepancies �")
Etiology 1) Psychic tension � Nervous children may develop bruxism 2) Occlusal discrepancies � Increased muscle tonus � Also seen in epilepsy, meningitis chorea.
 Tongue thrust � Also known as perverted or deviated swallow, retained infantile swallow,")
3) Tongue thrust � Also known as perverted or deviated swallow, retained infantile swallow, tooth apart swallow, tongue thrust syndrome or abnormal swallow. � Masseter muscle activity is prevented and as a consequence these is no molar contact during deglutition. Active mentalist muscle is noted.

� Classification �Anterior tongue- upper and lower incision. �Lateral or posterior – premolar and molar region �Combined � Incidence and duration of tongue thrust High incidence in school going children and patients with respiratory problem. � Fletcher associates reported following incidence � At age 6 years 52. 3% 8 years 38. 5% 9 years 49. 9% 10 years 34%
 Simple tongue thrust � This is localized posturing forward of the tongue during")
a) Simple tongue thrust � This is localized posturing forward of the tongue during rest and active function with localized anterior openbite.
 Complex tongue thrust � Forward tongue posture, tongue thrusting during swallowing, contract of")
b) Complex tongue thrust � Forward tongue posture, tongue thrusting during swallowing, contract of perioral muscles, excessive buccinator hyperactivity. When all these symptoms present the pattern is often called as complex tongue thrust.

Etiology � Bottle feeding � Hereditary or inherited � Oral habits – Thumb sucking, open bite � Ankyloglossia or macroglossia may cause tongue thrust. � CNS disorders – severe enough to prevent normal adult swallow. � Tonsillar tissue – If enlarged, can create destruction in oro-pharyngeal area posterior to root of tongue.

Effects of tongue thrust � Anterior openbite � Lateral or posterior open bite � Proclinated upper incisors � Hypotonic upper lip and appear retracted or short � Bilateral narrowing of maxillary arch
 Lisping and stammering � These are commonly occurring speech defects. � Speech defect")
4) Lisping and stammering � These are commonly occurring speech defects. � Speech defect create difficulty for the child while speaking. Lisping � This speech defect involves change of sound of letters and words.

Etiology � Main cause is continuity of infantile mode of speech. � If the tongue is moved forward without mandible and lies on top of lower incisors lisping may result. � Certain malocclusions like openbite, maxillary protrusion, mandibular retrusion and mal-aligned tooth also cause lisping.

Stammering � In stammering the child fails to produce any sound for sometime. These create emotional tension and difficulty in social adjustment. Etiology � Hereditary � Due to emotional tension � Lack of balance among two hemispheres of the brain. � Auditory amnesia

CLINICAL CONSIDERATIONS � Before any treatment is started or during diagnosis all functions of stomatognathic system if not proper , it can be primary etiologic factor in a malocclusion. � Many dysfunctions are acquired in the early stages of development. � Malocclusions that are acquired as a result of dysfunctions can usually be treated simply by elimination of disturbing environmental influences, which will foster normal development.

Respiration � Chair side, we should check for breathing weather it is nasal or oro-nasal. � It is diagnosed by the following test : - Giving a sip of water to patient and ask to keep it in mouth By placing cotton in between nose and mouth. Mouth mirror test. � Later , habit breaking appliances and also different exercises. - like deep breathing, - vigorous exercises, -playing on blowing type of musical instruments -and lip exercises.

Mastication � The masticatory apparatus teeth, muscle of mastication, TMJ movement should be thoroughly checked. � In case of bruxism there is presence of occlusal fact, or occlusal interference, pain in TMJ or tenderness of muscles of mastication. � So therapy includes elimination of triggering elements, mainly discrepancies between, centric relation and CO by occlusal adjustment, by giving occlusal bite plate, protective mouth guard or rubber splints.

Deglutition � Between 2 to 4 years of age mature swallow is seen in normal developmental patterns. � If the infantile swallowing can persists well after 4 years of life and is then considered a dysfunction or abnormal. � A proper diagnosis of tongue thrust should be done on the basis of clinical features or by checking the swallowing patterns. � Circum oral tension is being used as diagnostic criteria by many clinicians. � After diagnosing a tongue thrust habit it should be properly treated.

� If the tongue thrust is present at 3 to 9 years of age no appliance therapy is usually indicated only the dentist instruct the patient how to swallow correctly. � On recall appointments if the openbite improves or remains same, this approach is continued until 9 years of age. � If open bite continues to increase intraoral therapy is indicated. � If tongue thrusting is associated with lisping, only a speech therapist should be encouraged to correct the speech problem using articulation therapy.

Speech � During diagnosis attention should be given towards speech also. � The etiology of speech problem should be recognized and proper treatment should be given. � The presence of speech defects in childhood is due to lack of sufficient training and maturity. � As these factors are provided the speech defects disappears. The guardians and teachers should therefore encourage childrens to pronounce correctly. � If defect continued till late age when they removed by means of surgery.
- Slides: 24